


Abstract
Background: Transforming growth factor beta-1 (TGF-β1) participation in breast cancer development and metastasis is well-established, however, the clinical meaning of its circulating levels in women with breast cancer is poorly understood. Aim: To characterize the levels of TGF-β1 in plasma from women with breast cancer and to associate them with the main clinical factors associated with disease prognosis. Patients and Methods: TGF-β1 levels were measured by Enzyme-linked immunoassay (ELISA). Clinicopathological data were also assessed. Results: Women bearing triple-negative tumors presented significantly reduced levels of this cytokine when compared to the other subtypes (p=0.0338). Patients with metastases exhibited lower levels of TGF-β1 than the non-metastatic cohort (p=0.0442). Patients with early-onset disease had the highest plasma TGF-β1 levels (p=0.0036). Doxorubicin chemotherapy induced a reduction in TGF-β1 level, promptly after drug infusion (p=0.0494). Patients with TGF-β1 levels lower than 20 pg/ml exhibited a tendency to have a reduced overall survival in a 40-month follow-up. Conclusion: Lower levels of circulating TGF-β1 are associated with a poor disease prognosis.
Transforming growth factor beta (TGF-β) is a family of growth factors that affect both normal and neoplastic processes in the mammary gland. This pleiotropic cytokine is well-implicated in regulating tissue remodeling and apoptosis in normal breast development (1). The role of TGF-β1, the most abundant isoform of TGF-β, in normal breast is based on its tumor suppressor functions. However, in breast cancer, this cytokine has tumor-promoting functions, especially in cells that evade TGF-β1-regulating properties during metastatic progression (2).
Effects of TGF-β1 can be systemically observed beyond the tumor microenvironment, since virtually all cells present with TGF-β receptors (1). TGF-β also displays a redox-sensor function, as evidenced during experimental radiation response (3). It has been implicated in several processes, mediated by reactive species, particularly inflammation, aiming at the restoration of homeostasis. This redox-sensor activity seems to further regulate the reactive oxygen species (ROS) production in chronic processes (3).
Some important evidence regarding this cytokine has been reported in human breast cancer. Analysis of gene expression signatures reveal that TGF-β signaling regulates the expression of some chemokines during disease progression and is associated with poor patient prognosis, mainly in those with estrogen-positive tumors (4). On this regard, the impact of TGF-β in cancer has become so evident that an anti-TGFβ therapy has been explored and improved (5-10). Over the years, the role of TGF-β in mammary tumorigenesis has been established in vitro (11-13), as well as in situ by studies in resected tumors from patients, especially in metastatic conditions (14-16). Furthermore, members of the TGF family are also predictors of poor response to chemotherapy in women with breast cancer (17).
Although the role of TGF-β in breast tumors has been successfully established, the characterization of its circulating levels in patients and its clinicopathological meaning in human breast cancer is poorly understood. Thus, the aim of this study was to provide a comprehensive characterization of TGF-β1 circulating levels in plasma from breast cancer women concerning the main factors associated with disease prognosis, as disease stage, tumor molecular subtype, metastatic status, age at diagnosis, chemotherapeutic regimen/response, as well to come up with the 40-month survival profile of patients according to its levels.
Patients and Methods
Patient selection and design of the study. This prospective study enrolled a total of 101 women. A group of 61 women diagnosed with ductal infiltrative carcinoma of the breast, were recruited at the Londrina Cancer Institute, Londrina, Paraná, Brazil, from January 2009 until September 2011, and 40 healthy women were selected as age-paired volunteers to comprise the healthy control group. This study was approved by the Research and Ethics National Council (CAAE 0009.0.268.000-07) and all practices were approved by the Institutional board. All participants provided informed consent. Patients' clinical history was assessed and included age at diagnosis, weight, comorbidities, TNM-staging (tumor-node-metastasis classification of breast cancer) and hormonal status.
Patients were divided into cohorts classified according to clinical and biochemical parameters regarding breast cancer prognosis and progression, as follows: disease stage, molecular subtype of breast tumor, presence or absence of primary tumor, occurrence of metastasis, age at diagnosis, type of chemotherapy and its impact after infusion, chemotherapy resistance, incidence of death and survival rates.
The control group consisted of healthy women, age-paired with patients (34-78 years), without previous history of any type of cancer, chemotherapy, hormonal or antioxidant therapy, or chronic diseases. Women were excluded if they were currently smoking, had hepatic, cardiac or renal dysfunction, obesity, use of drugs, hypertension, sedentarism, diabetes and other eventual chronic conditions. Sample was obtained from whole blood collected before chemotherapy infusion in heparinized vacuum tubes (10 ml) and plasma was separated by centrifugation at 1,400 ×g during 5 min. Aliquots were stored at −76°C until analysis.
Immunohistochemical staining of tumor samples. Patients were divided in three cohorts, classified according to immunohistochemical criteria for defining breast cancer intrinsic subtypes, based on molecular receptors expression profile (18): Luminal, HER-2 enriched and triple-negative groups. Formalin-fixed paraffin embedded biopsies from patients were immunostained with primary antibodies against estrogen receptor (ER), progesterone receptor (PR) and human epithelial growth factor receptor 2 (HER-2) (Dako, Denmark) and identified by light microscopy as positive or negative, based on stained areas and intensity.
TGF-β1 analysis. TGF-β1 levels in plasma were determined using a commercial antibody-specific RSG ELISA kit (eBiosciences, San Diego, USA) employing internal controls, as proposed by the manufacturer and analyzed with an ELISA microplate reader at 490 nm. Plasma samples were previously acidified to activate latent TGF-β1 to its immunoreactive form. The limit quantification was 2 pg/ml. The results were calculated in pg/ml by fitting to a standard curve, obtained using human recombinant TGF-β1.
Oxidative stress profile. Total antioxidant capacity of the plasma (TRAP) and the erythrocytic reduced glutathione content (GSH) were used to determine the antioxidant profile, while nitric oxide levels (NO) and plasma malondialdehyde (MDA) represented the pro-oxidative status. All methods were performed as previously published (18, 19).
Statistical analysis. Analyses were carried out in duplicate sets and data were expressed as the distribution of individual values and the respective medians. Parameters were compared by the Mann-Whitney test. Survival rates were evaluated by the Kaplan-Meier method and the log-rank test was performed. A value of p<0.05 was considered significant. Spearman's test was also performed to verify possible correlation among parameters. All statistical analyses were performed using the GraphPad Prism version 5.0 (GraphPad Software, San Diego, USA).
Clinicopathological characterization of patients.
Results
Clinicopathological characterization of the patient cohort is provided in Table I. The median age at diagnosis was 59.1 years and all enrolled women were diagnosed with infiltrative ductal carcinoma of the breast. The molecular receptor status presented a distribution frequently observed in the general population. TNM staging displayed an equivalent distribution between early (TNM-I and -II) and advanced (III and IV) disease.
TGF-β levels in plasma were screened and categorized according to clinical parameters. Patients evaluated by TNM staging did not exhibit any differences in TGF-β levels (Figure 1A). With respect to the molecular classification of breast cancer subtypes (Figure 1B), it was observed that patients bearing triple-negative tumors presented significantly lower levels of TGF-β when compared to the general cohort of women with breast cancer (p=0.0338). The surgical removal of the primary tumor mass did not affect the TGF-β1 level in the plasma when compared to patients still bearing the primary tumor (Figure 1C). Plasma TGF-β1 levels were also diminished in patients suffering distant metastases when compared to those with non-metastatic disease (p=0.0442). Women presenting early-onset (<45 years of age) of disease had higher levels of TGF-β when compared to those that had late-onset (age ≥45 years, p=0.0036).

Clinical parameters and transforming growth factor beta-1 (TGF-β1) level from patients diagnosed with ductal infiltrative carcinoma of the breast. Plasma TGF-β1 level was distributed according to TNM staging classification (A), breast tumor subtype (B), presence (T) or absence (NT) of the primary tumor (C), occurrence (M) or not (NM) of distant metastasis (D) and age at diagnosis of disease (E). Groups were compared by the Mann-Whitney test. *Statistical difference when compared to control, #when compared to all patients diagnosed with breast cancer (p<0.05), ΔSignificant difference between metastatic (M) and non-metastatic (NM) groups; *signficant difference between patients classified according to age at diagnosis. CTR (healthy control group); CA (all patients bearing ductal breast cancer enrolled in the study); ED (early-stage patients, TNM I and II), AD (advanced stage patients, TNM III and IV); LUM (patients bearing luminal breast tumors); HER+ (patients bearing HER-2 amplified tumors); TN (patients bearing triple-negative tumors).

Chemotherapy evaluation and transforming growth factor beta-1 (TGF-β1) levels from patients diagnosed with ductal infiltrative carcinoma of the breast. Plasma TGF-β1 level was distributed accordingly to Doxorubicin (DOX) or Paclitaxel (PTX) treatment (A); before (BT) or after (AT) chemotherapy (B); and sensitivity (S) or resistant (R) to treatment (C). Groups were compared by the Mann-Whitney test. *Significant difference between CA and AT groups; #significant difference between AT and BT groups, and DOX and PTX groups (p<0.05). CTR (healthy control group); CA (all patients bearing ductal breast cancer enrolled in the study).
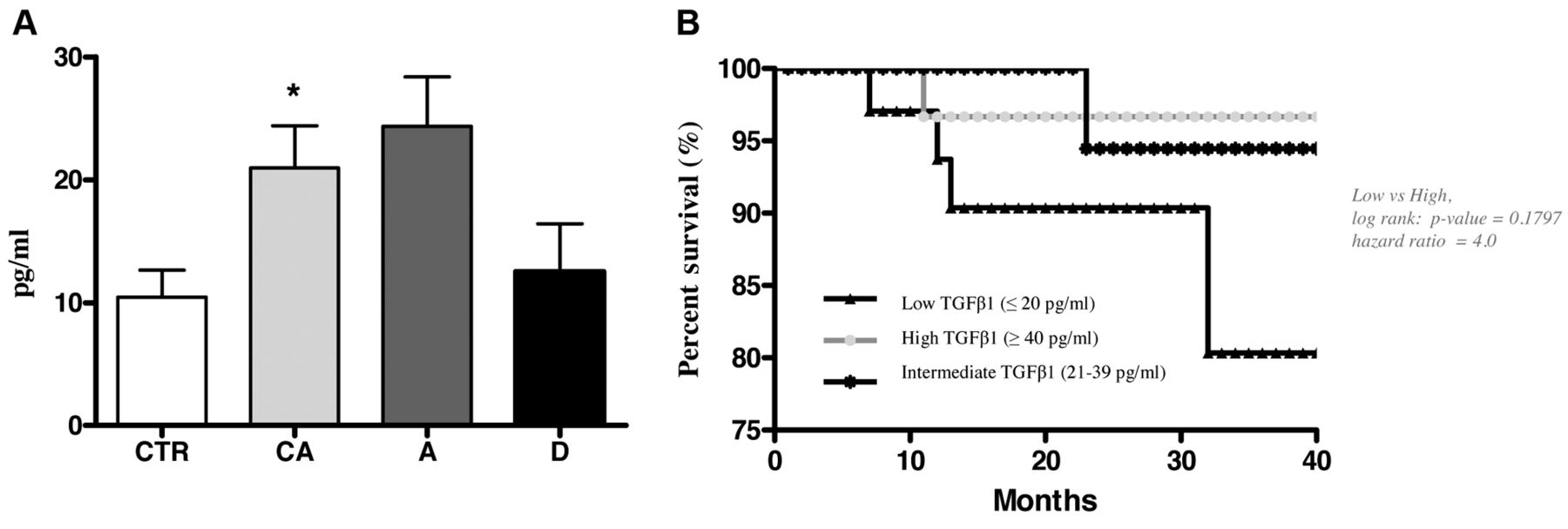
Figure 2A shows that TGF-β1 levels depended on the type of chemotherapeutic regimen, since patients undergoing doxorubicin chemotherapy, as monotherapy presented a significant reduction in plasma TGF-β1, when compared to patients that received only paclitaxel as treatment (p=0.0088). TGF-β1 levels in patients with breast cancer were higher compared to these in healthy controls (p=0.0435, Figure 2B). Furthermore, the evaluation of TGF-β1 in patients after treatment with paclitaxel plus doxorubicin, compared before and after infusion showed that chemotherapy promptly reduced TGF-β1 to levels to a smaller extent than those observed in patients with breast cancer without any treatment (p=0.0494). In relation to chemotherapy response (Figure 2C), TGF-β1 levels did not differ between patients with responsive and those with resistant disease.

Survival profile and transforming growth factor beta-1 (TGF-β1) level from patients diagnosed with ductal infiltrative carcinoma of the breast. Plasma TGF-β1 levels were distributed according to analysis of the number of alive and dead patients (A). Overall survival of patients based on TGF-β1 level, evaluated during a 40-month follow-up (B). Groups were compared by the Mann-Whitney's test. *Statistical difference when compared to control and # when compared to all patients diagnosed with breast cancer (p<0.05). CTR (Healthy control group); CA (all patients bearing ductal breast cancer).
Analysis of the survival profile (Figure 3) indicates that the TGF-β1 levels in the cohort of patients who survived and the group that died, did not differ significantly (Figure 3A). In order to understand the impact of the TGF-β1 levels on survival rates (Figure 3B), patients were categorized as having low (≤20 pg/ml), intermediate (21-39 pg/ml) or high (≥40 pg/ml) circulating levels. Although no significant differences were found, patients with lower levels of TGF-β1 (p=0.1797) tended to present the lowest survival rate when compared with patients bearing high TGF-β1 levels.
An overview of the correlation between TGF-β1 levels and oxidative stress parameters is presented in Table II. A significantly positive correlation was observed between the TGF-β1 level in plasma and the erythrocytic antioxidant content, represented by GSH levels (p=0.0231).
Discussion
The prognostic utility of TGF-β in human breast cancer has been recently described. TGF-β has been implicated in diminished overall survival (20), early tumor progression (21) and enhanced breast cancer susceptibility (22). Nevertheless, an overview of this circulating cytokine in a context including the most relevant prognostic and clinical aspects of breast cancer disease is still lacking. Our study provides information regarding some of the known aspects and novel insights into aspects of TGF-β1 in breast cancer for the first time. Relevant findings include the occurrence of lower TGF-β1 levels detected in patients bearing the triple-negative tumor subtype, as well as in those carrying metastatic disease who are submitted to doxorubicin chemotherapy. On the other hand, high plasma levels were found in patients with early-onset disease (with age at diagnosis below 45 years). When stratified by TGF-β1 levels, it was detected that patients exhibiting low circulating levels of this cytokine (lower than 20 pg/ml) tended to a reduced overall survival when compared to those that presented with high TGF-β1 levels (up to 40 pg/mL).
Spearman's correlation of transforming growth factor beta-1 (TGF-β1) level and oxidative status of patients with breast cancer.
A global analysis of circulating TGF-β1 in women carrying breast tumors revealed the occurrence of high levels of this cytokine, when compared to healthy controls. Alterations in TGF-β signaling affect a variety of aspects of breast cancer development and progression, justifying its role according to disease staging (23). Sustained TGF-β expression in breast cancer is mainly associated with the advanced stages of disease (24), in agreement with the distribution of most of our patient cohort (about 65% in TNM stages III and IV).
Our results further indicate the existence of a differential profile of circulating TGF-β1 according to the molecular subtype of breast cancer. Patients bearing triple-negative tumors had significantly lower TGF-β1 levels when compared to both those with the luminal/HER2 subtypes and healthy controls. Although the estrogen pathway has a regulatory effect on TGF-β signaling in the breast, evidence supports the deregulation of such networks in breast cancer (25), reflected by our findings of reduced circulating TGF-β in the triple-negative cohort. A well-established fact, also described here, is that patients with metastatic disease present enhanced TGF-β1 levels when compared to those with non-metastatic and to healthy individuals. The metastatic potential induced by this cytokine is mainly related to its capacity to polarize the epithelial-mesenchymal transition of mammary epithelial cells and to ensure its malignant phenotype (26).
We further demonstrated that the circulating levels of TGF-β1 is significantly different in relation to the age at diagnosis. Patients presenting early-onset disease (under 45 years) exhibited higher levels of this cytokine in relation to older patients. High expression of both extracellular TGF-β and TGF-βR2 have been identified in breast tumors and are strongly associated with earlier age at onset (27), corroborating our findings.
Studies demonstrate that alterations in TGF-β signaling affect the toxicity of doxorubicin and enhance its antitumoral activity (28-30). We showed that patients undergoing doxorubicin-based chemotherapy display a reduction of circulating TGF-β1 when compared to untreated or paclitaxel-treated cohorts, but no alteration in the sensitivity profile was found. This profile was promptly observed after doxorubicin infusion, indicating that this drug is able to promote a swift reduction in the circulating levels of TGF-β1. The mechanism underlying this fact is not known.
Although not significant, we observed a tendency for reduced overall survival in women presenting TGF-β levels lower than 20 pg/ml. Alterations in TGF-β signaling are associated with poor outcome in breast cancer. A large cohort study demonstrated the occurrence of dysfunctions in the components of the TGF-β cascade in tumors and associated some of these aspects with shorter overall survival (31). To the best of our knowledge, this study is the first report highlighting this information on survival, according to stratification by circulating TGF-β1 levels. A continuous follow-up of such patients is necessary to enlighten the long-term meaning of these findings.
Finally, we found a significant positive correlation between plasma TGF-β and erythrocytic GSH content. The occurrence of oxidative stress in women with breast cancer is well-known (19, 33) and this can contribute to some pathological processes, mediated by TGF-β. The antioxidant system has been described as a protective mechanism against latent TGF-β activation in pathological processes (32), indicating that the positive correlation observed here between this cytokine and GSH levels may reflect TGF-β redox-sensor activity (3).
In conclusion, our data add new information which contributes to the better comprehension of the clinical meaning of circulating TGF-β1 in women with breast cancer. Furthermore, reduced circulating TGF-β1 seems to be a determinant of poor disease prognosis.
Acknowledgements
The Authors would like to thank Jesus Antônio Vargas for excellent technical assistance, and all of the participating women for making the study possible. This work was supported by Coordination of Improvement of Higher Education (CAPES), National Council of Scientific and Technological Development (CNPq), and Araucaria Foundation.
Footnotes
-
↵* These Authors contributed equally to this study
-
Conflicts of Interest
The Authors declare no conflicts of interest.
- Received November 8, 2012.
- Revision received December 4, 2012.
- Accepted December 5, 2012.
- Copyright© 2013 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}