


Abstract
Background: Sirolimus is a potent blocker of mammalian target of Rapamycin (MTOR), with anti proliferative activity. Its potential for the management of oral cancer has been suggested. Our aim was to establish an analytical method for determining sirolimus levels in human saliva and to calculate the blood vs. saliva ratio in individuals using sirolimus chronically in order to evaluate the total oral tissue exposure. Patients and Methods: Chemiluminescent microparticle immunoassay technology (CMIA) was used to determine the blood and saliva levels of sirolimus in four transplant patients chronically-treated with sirolimus. Results: An analytical method for determining sirolimus levels in human saliva was established. We demonstrated that saliva levels were on average six times lower than blood levels. Conclusion: The specific sensitive analytical method showed that the saliva levels of sirolimus are significantly lower than blood levels, thus reinforcing the rationale for the use of topical oral sirolimus to enhance availability, efficacy and safety for treating oral malignancies.
Oral sirolimus (Rapamycin) was introduced in 1999 as an immunosuppressive agent mostly prescribed for kidney transplant patients. Sirolimus is a potent blocker of mammalian target of rapamycin (MTOR) pathway, with antiproliferative effects (1). The mTOR pathway is responsible for normal cell division, proliferation and anabolism. The efficacy of sirolimus as an anticancer agent has been demonstrated in a number of solid tumor types including head and neck squamous cell carcinoma (HNSCC) (2). Its inhibitory effects on the mTOR pathway have also been noted in numerous cell types and animal models, enabling its clinical use in cancer management (3, 4). There are current clinical trials regarding the efficacy of sirolimus in the treatment of various malignancies, including HNSCC (www.clinicaltrials.gov, October 2012 for “head and neck” and “sirolimus”). It is important to note that oral squamous cell carcinoma (OSCC) accounts for most of the cases of oral cavity and oropharyngeal cancer worldwide and is the major cause of HNSCC (5). Although sirolimus is a very promising candidate for the management of oral cancer and of oral potentially malignant disorders (PMD), it has severe side-effects, such as metabolic and hematopoietic disorders, when systemically administered, which obviously restrict its use (6). Topical treatment strategies, e.g. oral pastes and washes, have been used successfully to treat various oral pathologies, including oral lichen planus, recurrent aphthous stomatitis and radiation-induced mucositis (7). Topical application of sirolimus in the form of mouthwash has been shown to be efficient in the treatment of chronic erosive oral lichen planus (a PMD) with negligible absorption and only minor side-effects (8). In order to develop a topical delivery method for sirolimus, it must be possible to determine salivary levels of the medication and to characterize the mucosal exposure to the drug in systemically-treated patients. The aim of this work was to evaluate saliva sirolimus levels in kidney transplant patients chronically treated with oral sirolimus and compare them with blood levels. The first aim was to adapt an analytical method, used routinely to determine blood levels, to measure salivary levels. The second aim was to calculate the ratio between blood and saliva levels of sirolimus, and characterize the total i.e. systemic and local exposure of the oral mucosa to the drug.
Patients and Methods
Study design. Patients treated with oral sirolimus were included in the study. For all patients, blood levels of the medication were stable. Blood and salivary samples were collected and analyzed at the same time. All patients signed informed consent forms and an examination of the oral cavity was performed; clinical findings and oral symptoms, if any, were recorded along with the medical status of the patient. Five milliliters of unstimulated saliva and five ml of whole blood were collected. The coded samples were kept at −80°C, until analysis. The ratio between blood and saliva levels was calculated. Routine clinical examinations, laboratory tests and treatments were recorded for each patient. The study was approved by the Institutional Review Board.
Patients' details.
Patients. Kidney transplant recipients from the Nephrology and Hypertension Services unit at the Hadassah Medical Center, treated for at least three years with oral sirolimus as prophylaxis against rejection, were included in the study. Patients under the age of 18 or with liver dysfunction were excluded.
Analytical method. Levels of sirolimus in blood and saliva were determined using the chemiluminescent microparticle immunoassay (CMIA) assay according to the manufacturer's instructions, using an Architect i1000 analyzer (Abbott Laboratories, Abbott Park, IL, USA). This technique is routinely used for therapeutic drug monitoring of blood levels of sirolimus with calibration range of 0-30 ng/ml and limit of quantification (LOQ) of 2 ng/ml. (9). We calibrated the existing method by adding known concentrations of sirolimus dissolved in methanol to salivary samples. The calibration range of the assay was linear at concentrations of 0.325-5.0 ng/ml of sirolimus in human saliva (LOQ=0.325 ng/ml).
Statistical analysis. Statistical analysis was performed using the SPSS 18 software. Statistical significance was determined using an unpaired, one-tailed t-test. p-Values less than 0.05 were considered significant.
Results
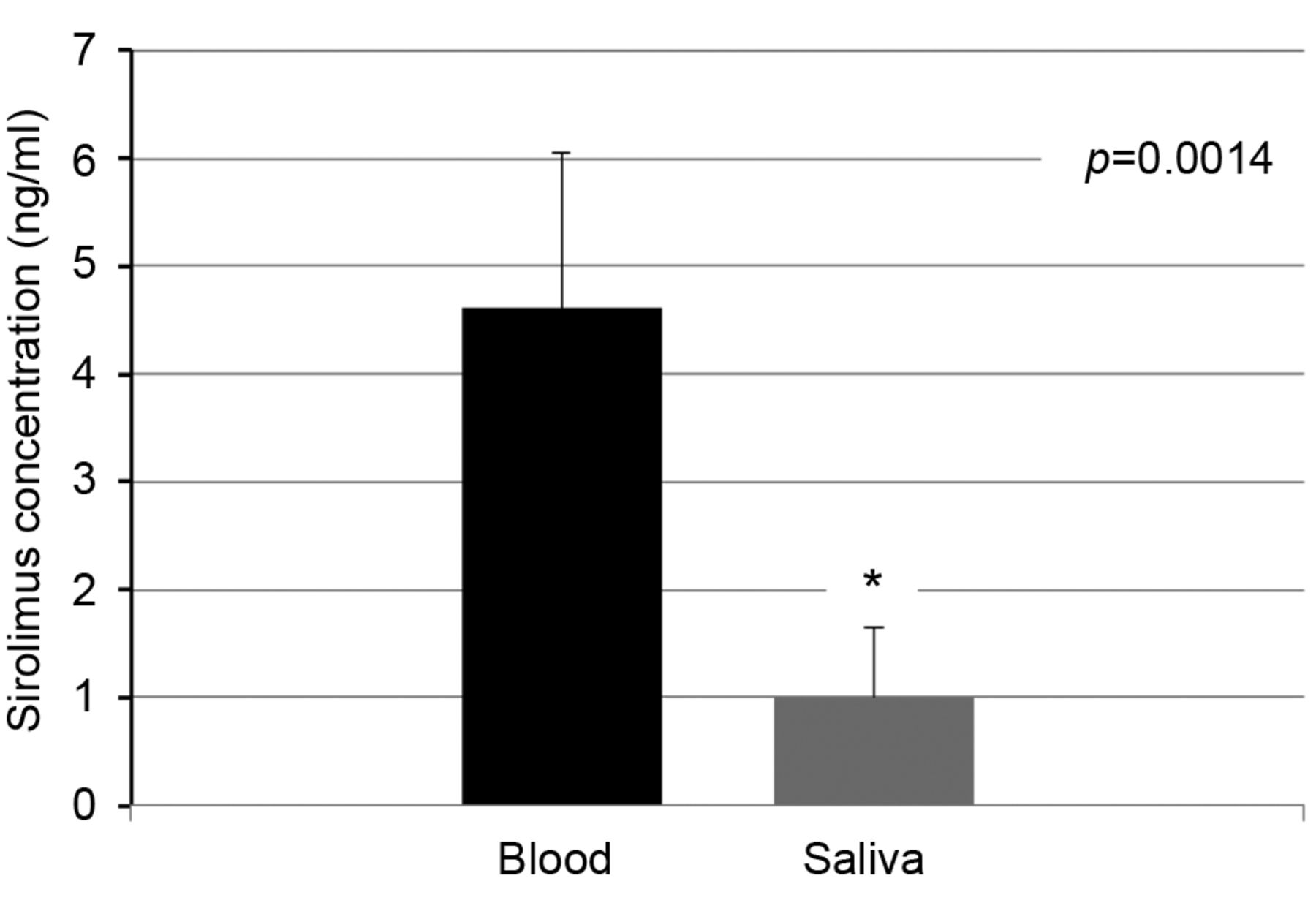
Four patients were included in the study; their details are presented in Table I. Blood and saliva samples were obtained together. Patient 1 received the medicine 12 hours, patient 2 18 hours and patients 3 and 4 24 hours before sampling. None of the patients had pathological lesions in their oral cavities. Whole blood and saliva levels of sirolimus are summarized in Table II and Figure 1. We found a significantly lower (approximately six-fold) sirolimus concentration in human saliva when compared to blood in chronically-treated kidney transplant patients. A substantial variability was observed among samples. No linear correlation was found.
Sirolimus concentration in blood vs. saliva from four kidney transplant patients.
Discussion
Sirolimus has been extensively studied for the management of pathologies of the oral cavity, although its derivatives (rapalogs) are more commonly used as immunosuppressants. Currently there are clinical studies evaluating the efficacy of sirolimus in humans suffering from OSCC, oral PMD and oral lichen planus (www.clinicaltrials.gov). Based on reports and on the growing number of clinical trials, sirolimus is a potent mTOR inhibitor, and shows promise in the treatment of certain oral pathologies. In contrast to immune system cells which are only exposed to sirolimus through the blood, the cells of the oral mucosa can also be reached topically. Topical administration has many advantages including lower dose and systemic exposure, as well as enabling effective anatomical targeting and a much higher free (active) concentration of the drug. Mouth washes and oral pastes are common oral delivery systems. In order to develop a topical delivery system for sirolimus, a method for determining its concentration in the saliva is necessary. In this study, CMIA technology, usually used for routine blood monitoring, was used to our knowledge for the first time, to analyze sirolimus in human saliva and compare the salivary and blood levels at specific time points. These findings are important in light of the ongoing clinical trials, in which salivary levels of sirolimus have not been determined. Numerous drugs have been evaluated in human saliva in order to improve monitoring methods. Our results clearly demonstrate the low concentration of sirolimus in human saliva during systemic administration.

Average concentration of sirolimus in blood vs. saliva. Data are presented as means±SD (n=4).
This finding is congruent with those of other studies (10, 11) which compared salivary and blood levels of other medications. Salivary sirolimus concentrations were low, and did not correlate linearly with the whole blood concentration. In this study, we explored the blood vs. saliva ratio as a possible basis for topical oral use of sirolimus rather than just as a monitoring issue. The large variability observed among patients can be explained by the general polymorphism in the population, as well as the small sample size of the study. Our data contribute to understanding drug levels in the oral cavity in chronically-treated patients. The ratio between sirolimus blood vs. saliva levels quantifies the total exposure (blood and saliva) of oral mucosa to the drug and demonstrates the achievable sirolimus levels in systemic treatment.
In summary, we applied a sensitive analytical method to determine sirolimus levels in the saliva and demonstrated that those levels are significantly lower than the ones in the blood. These results emphasize the need for delivery methods with better topical oral biological availability and reinforce the rationale for using sirolimus topically for the treatment of responsive oral pathologies. Topical delivery will improve bioavailability in the oral cavity along with additional therapeutic benefits, including better efficacy of the targeting system, improved safety and increased compliance.
Acknowledgements
This study was supported by a Project Grant from the Israel Cancer Research Fund and the Joint Research grant of the Hebrew University and Hadassah School of Dental Medicine.
- Received November 26, 2012.
- Revision received January 7, 2013.
- Accepted January 9, 2013.
- Copyright© 2013 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.