


Abstract
Clear cell adenocarcinoma arising out of endometriosis of the urinary bladder is a rare entity. The published literature has a dearth of information about this entity and its histogenesis. In the present case review we present a 59-year-old patient who was treated with robotic anterior pelvic exenteration and ileal conduit. The initial biopsy of bladder tumour purported a high-grade urothelial carcinoma, however the final specimen revealed a clear cell adenocarcinoma arising in endometriosis without any urothelial cancer. Early case reports refer to these lesions as mesonephric or mesonephroid adenocarcinomas but the current WHO nomenclature classifies them under non-urothelial epithelial neoplasms as clear cell adenocarcinomas. Here, we review the literature and discuss their origins.
Clear cell adenocarcinoma arising out of endometriosis of the urinary bladder is a rare entity. The published literature has a dearth of information about this entity and its histogenesis. Here we present a case of a 59-year-old female who was treated with robotic anterior pelvic exenteration and ileal conduit.
Report
A 59-year-old female was referred from her general practitioner to a tertiary urological clinic for management of a 7-year history of intermittent hematuria. Associated symptoms included abdominal pain “like period pain”, as reported by the patient. She was 10 years post-menopausal and medical history included hypercholesterolemia, two caesarian sections, 30 years previously, and tubal ligation. Physical examination was unremarkable. Urinary cytology showed atypical urothelial cells. Otherwise the blood results were all unremarkable.
Ultrasound showed a large mass of 36×24×28 mm on the superior bladder wall with normal upper tracts. Subsequent computed tomography scan of abdomen confirmed this mass and excluded evidence of any extravesicular spread or metastasis. Based on these findings, the patient underwent cystoscopy and transurethral resection of the bladder tumour. Endoscopic findings were suggestive of muscle invasive disease. A high-grade urothelial carcinoma with extensive (almost 100%) glandular differentiation and stromal invasion was diagnosed from the biopsy specimen (Figure 1).
Based on these findings, the patient was offered neoadjuvant chemotherapy with 2 cycles of cisplatin (Day 1; 1600 mg) and gemcitabine (Day 1, 8, 15; 124 mg) prior to robotic-assisted anterior pelvic exenteration and pelvic lymph node dissection with ileal conduit formation. Further staging with chest x-ray and bone scan was negative for metastasis.
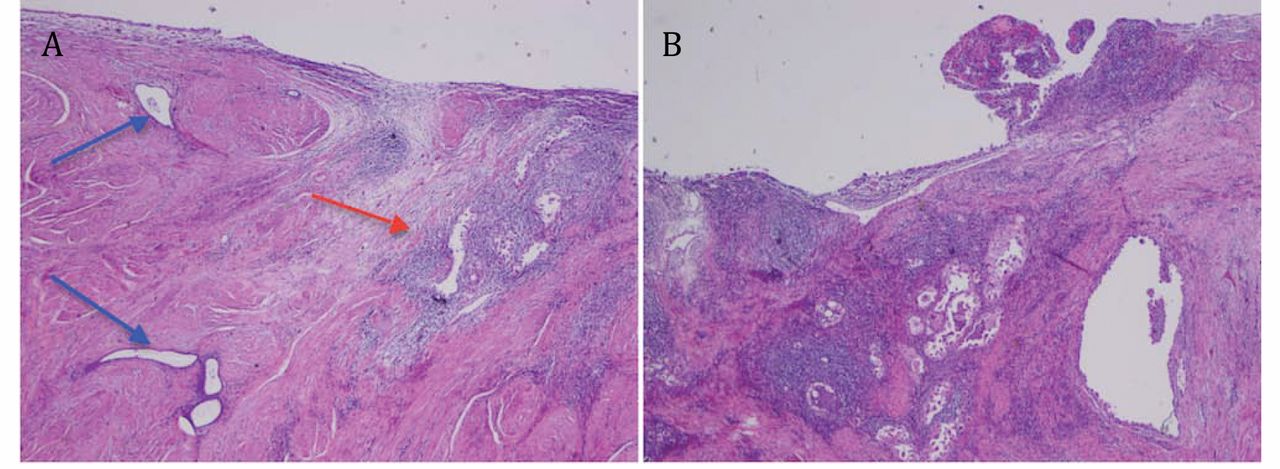
Interestingly, the definitive resection pelvic exenteration specimen revealed the true nature of the carcinoma: clear cell adenocarcinoma arising in endometriosis invading the outer half of the muscularis propria (Figure 2). There was no lymphovascular invasion, the margins were clear and 20 lymph nodes were identified as being negative for disease. There was no evidence of any primary urothelial malignancy. Medical Oncology consult was sought and the patient was given 3 cycles of adjuvant carboplatin (Day 1; 520 mg) and paclitaxel (Day 1, 8, 15; 138 mg).
There is no evidence of recurrence or metastasis after 12 months of follow-up.
Discussion
Similarly to our case, most published literature describes this condition almost exclusively in females and usually in their fifties or sixties (1). The majority of cases develop in association with urethral diverticula, but rare cases appear primarily in the bladder itself.
Although clear cell carcinoma of the lower urinary tract has been also described rarely in men, and in age ranges between 19 and 80 years, this group is heterogeneous and most represent clear cell change in otherwise typical urothelial carcinomas.
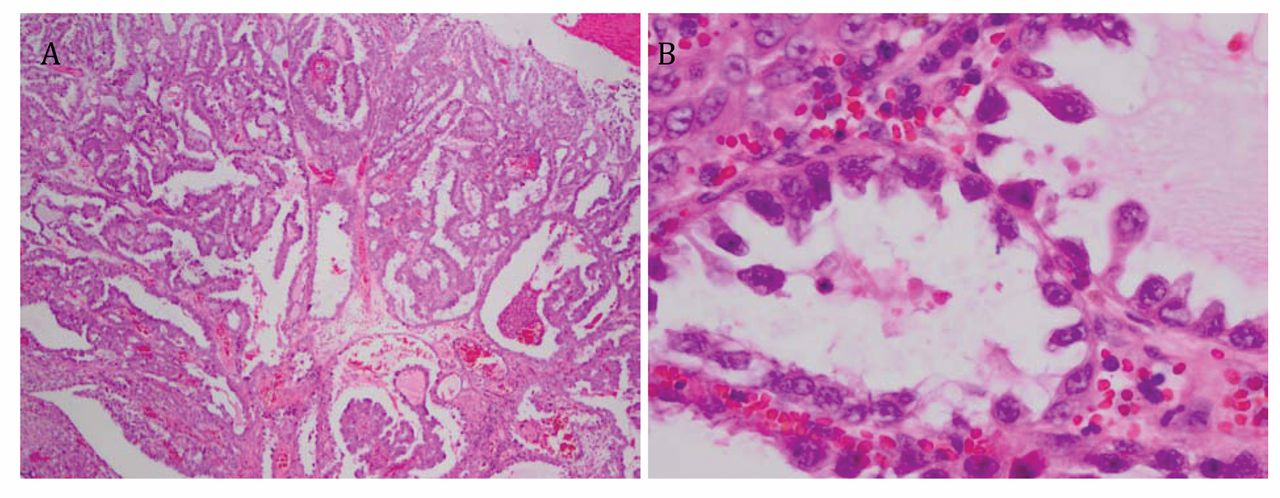
Hematoxylin and eosin stain of the bladder biopsy showing the papillary architecture with hobnail cells. (A: ×40, B: ×100).

Hematoxylin and eosin stain of cystectomy specimen. A: Blue arrows: endometriosis, red arrow: cancer. B: Residual papillary surface and invasive components. (A & B ×40).
Early case reports refer to these lesions as mesonephric or mesonephroid adenocarcinomas but the current WHO nomenclature classifies them under non-urothelial epithelial neoplasms, as clear cell adenocarcinomas (2). The published literature mainly focuses on theories of origin of these tumours – mesonephric or Mullerian. Tumours were found at the bladder neck, urethra, and posterior wall, and usually with a co-existing component of urothelial cancer (3).
In our case, the lesion was located on the postero-superior wall in a focus of endometriosis, without the presence of any primary urothelial cancer.
The theory of Mullerian origin is favoured based on three factors: its morphological similarity to tumours of this lineage within the female genital tract, that the tumours are largely found in women, and its frequent association with endometriosis (4). Immunohistochemical analysis of tumour samples does not reliably distinguish tumour origin, so it has been assumed that the embryonic origin varies with each case (5).
From a histological perspective, it is also important to consider benign clear cell lesions such as nephrogenic adenoma in the differential diagnosis (6). Both clear cell carcinoma and nephrogenic adenoma are well-characterised from a morphological viewpoint (7). Nevertheless, both are reported to express paired box gene-8, which can help differentiate less classical lesions from urothelial carcinoma (8).
Most patients undergo cystectomy as the only treatment. Only one case of radiotherapy treatment alone has been described, resulting in complete response of the localised disease (9).
Experience with chemotherapy is limited to an adjuvant setting. The drugs used include cisplatin and 5-fluorouracil 1, carboplatin and methotrexate (10), and adriamycin and cyclophosphamide (11), with or without radiotherapy.
Our patient had neoadjuvant and adjuvant chemotherapy along with robotic anterior pelvic exenteration and ileal conduit formation.
Conclusion
To out knowledge, this is the first case of this condition treated with robotic surgery following neoadjuvant chemotherapy. Endometriosis was co-located with the carcinoma and was also present at the aspect of the uterus. In our patient, there was no demonstrable urothelial malignancy in the final histology, indicating a Mullerian origin for this particular case.
- Received December 4, 2012.
- Revision received January 15, 2013.
- Accepted January 15, 2013.
- Copyright© 2013 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}