


Abstract
Metastatic pancreatic malignant melanoma is considered to be a highly aggressive neoplasm, and only few metastasectomies for lesions originating from the skin or the ocular region have been reported. We report a case of resection of pancreatic metastasis of malignant melanoma originating from the nasal cavity. An isolated pancreatic tumor was detected in a 46-year-old man who had undergone proton-beam therapy for nasal melanoma 12 months earlier. He underwent distal pancreatectomy with splenectomy and the pathological diagnosis was metastatic malignant melanoma. We review cases of malignant melanoma metastatic to the pancreas and further discuss their incidence, therapeutic strategy, and outcome of mucosal melanoma of the head and neck.
Metastatic pancreatic tumors clinically account for fewer than 2% of all pancreatic malignancies (1, 2), and potentially resectable metastasis to the pancreas comprises 1.5-3.0% of all cases of pancreatic resection for neoplasms (2-4). Pancreatic metastases are often detected during follow-up of the primary lesion. The operative indication may differ between primary cancer and metastasis. According to a review of 243 patients with resected metastatic pancreatic tumors, the sites of origin were renal cell cancer (61.7%), colorectal cancer (7.8%), melanoma (4.9%), sarcoma (4.9%), lung cancer (3.3%), gastric cancer (3.3%), gall bladder cancer (3.3%), and breast cancer (2.5%) (1). A few decades ago, resection was usually not considered to be indicated for metastatic melanoma of the pancreas, because of multiple organ involvement and high morbidity and mortality after pancreatic surgery, but recent advances in diagnostic modalities and surgical techniques have made it acceptable. Surgical metastasectomy has the unique potential to cure the cancer or even provide palliation, whereas systemic chemotherapy for malignant melanoma only modestly improves survival. The indication for metastasectomy is limited to cases with a fair general condition, good disease control of the primary lesion, an isolated pancreatic tumor, and findings on imaging studies indicating resectable tumor. The original sites for malignant melanomas are mostly the skin of the head, neck, and lower extremities due to their frequent exposure to sunlight; however, malignant melanoma can occur in various mucosal sites where pigment cells are present. The etiopathogenesis, incidence, and clinical behavior of mucosal melanoma are considered to be different from those of skin melanoma. We present a case of pancreatic resection for metastatic melanoma originating from the nasal cavity and discuss clinical- and treatment-related issues of the condition.
Case Report
A pancreatic mass was detected in a 46-year-old man during follow-up of malignant melanoma of the nasal cavity. Seventeen months earlier, he had consulted an otorhinologist with bloody rhinorrhea and was diagnosed as having malignant melanoma of the left nasal cavity, clinical stage of T3N0M0, according to the International Union Against Cancer (UICC) classification, after detailed imaging studies and biopsy (Figure 1). The tumor did not show melanin pigment macroscopically. Proton beam therapy (PBT) was delivered with a total of 60 Gy equivalents (GyE) in 15 fractions (5) and complete remission was confirmed six months after the initiation of PBT (Figure 1). However, systemic screening studies after another six months detected a solitary mass of 33×31 mm in the pancreatic body (Figure 2). Blood tests showed only slightly elevated carbohydrate antigen 19-9 levels of 57.4 U/ml (normal range <37 U/ml). Solitary metastasis, well-controlled primary cancer, good general condition, and the patient's wish led to the decision to operate. Intraoperative findings did not reveal other abnormalities in the peritoneal space, and distal pancreatectomy with splenectomy as well as regional lymphadenectomy was performed. The postoperative course was uneventful and the patient was discharged on postoperative day 11. Macroscopic and histological findings with immunohistochemical profile, consistent with the findings of pre-treatment biopsy of the nasal cavity lesion, confirmed the diagnosis of metastatic melanoma of the pancreas (Figures 3 and 4). One out of 27 lymph nodes was found to be positive for metastasis. Unfortunately, metastases of the lung, skin, and intraperitoneal space were detected three months after the operation. The patient died 10 months postoperatively in spite of receiving systemic chemotherapy for recurrent disease.

Images before and after proton beam therapy (PBT). a: Initial facial Magnetic resonance imaging (MRI), axial slice. b: Initial facial MRI, coronal slice. An irregular mass in the left nasal cavity, 40×32×20 mm, extending to the ethmoid sinus, is shown. c: Pre-treatment positron emission tomography (PET) showed significant fluorodeoxyglucose accumulation (FDG) with a maximum standardized uptake value of 13.1. d: PET after PBT showed loss of FDG accumulation in the lesion.
Discussion
English language publications on pancreatic resection for metastatic melanoma of the pancreas are listed in Table I (3, 4, 6-25). The primary sites of malignant melanoma in the reported cases were skin, ocular region, and unknown. Although other articles reported a wide range of the interval from therapy for the primary cancer to recurrence in the pancreas (median 6 years, range 1-24 years), the present case showed relatively early recurrence (one year) after PBT. This suggests that the natural history of malignant melanoma is variable. Our patient underwent PBT for the primary lesion because of unresectability, with concerns about cosmesis and function. Although the cancer behavior after PBT is not well-known, the biology of melanoma, especially mucosal melanoma in the head and neck, should be considered.
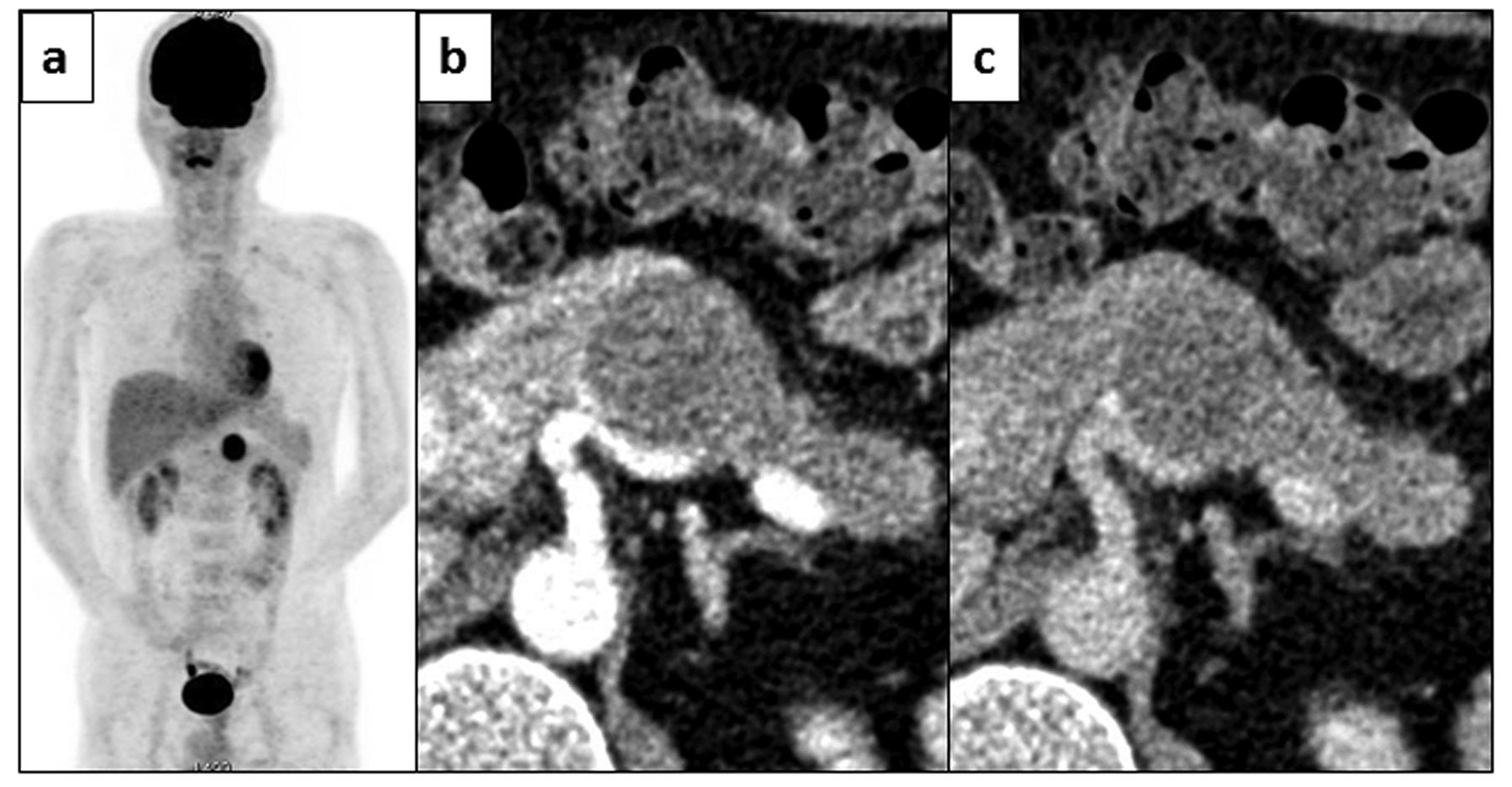
Preoperative images. a: Significant fluorodeoxyglucose accumulation with a maximum standardized uptake value of 10.6 was detected in the pancreatic body on positron emission tomography. No other significant accumulation was seen. b: Computed tomography (CT) of early enhanced phase. c: CT of late enhanced phase. The tumor was located in the pancreatic body, 33×31 mm, and was oval with a clear boundary, without calcification inside. Enhancement study showed prolonged enhancement of the tumor. No main pancreatic duct dilation was observed.
Regarding the incidence of mucosal melanoma of the head and neck, it accounts for only 1.4-1.7% of all cases of melanoma in Western countries, versus 23.3% in Japan (26, 27). Mucosal melanoma confined to the nasal cavity comprises about 4% of all sinonasal malignancies and about 80% of melanomas in the sinonasal tract (26). Mucosal melanomas generally tend to be more aggressive and have a poorer outcome than cutaneous melanoma; however, the 5-year survival rate for mucosal melanoma of the nasal cavity is 31%, which is better than that of 14-17% for malignant melanoma of the head and neck, and 0% for malignant sinus melanoma (26, 28). According to the UICC TNM classification (7th edition) of malignant melanoma of the aerodigestive tract, T1 and T2 tumors equivalent to stage I and stage II are omitted, and the emergence of cancer inidicates T3 and stage III or more, because of the highly malignant potential. The most frequent sites of distant metastases of sinonasal melanomas are lung, liver, and bones (29). These data suggest that pancreatic metastasis of nasal cavity melanoma is quite rare and is considered to indicate a poor prognosis, even though melanoma of the nasal cavity itself has a relatively fair prognosis compared to other mucosal melanomas.

Macroscopic image of tumor cut surface of resected tumor specimen. In places, the tumor circumference did not have a clear boundary from normal pancreatic parenchyma, and the cut surface was yellowish-white (amelanotic) and solid.
With the advancement of pancreatic surgery, metastasectomy of malignant melanoma has been proven to be reasonable, although controversy exists due to its being quite an aggressive pathological condition. Reddy and Wolfgang reported the feasibility of pancreatic metastasectomy in a review of 243 patients, which showed 38.3% morbidity and 1-2% mortality. They also reported the outcome of pancreatic resection for 11 cases of metastatic melanoma, with a median survival of 14 months (1). In a review of 234 patients with metastatic pancreatic tumors, Masetti et al. reported that metastases from melanoma were associated with significantly shorter survival, with a hazard ratio of 4.14, compared with that for renal cell carcinoma (30). The results of multiple single-institution studies emphasized the importance of curative resection for metastatic melanoma, with a 5-year survival rate of 15-30% and median survival time improving from 5-8 months to 15-28 months after complete metastasectomy, while patients with long-term survival have been reported (3, 10, 31-33). Prognostic factors reported to influence survival of patients with metastatic melanoma are earlier primary tumor stage, absence of intervening lymph node metastases, an interval of more than three years after resection of the primary lesion, and first metastatic sites including skin, subcutaneous tissue, lymph nodes, and lung (33).

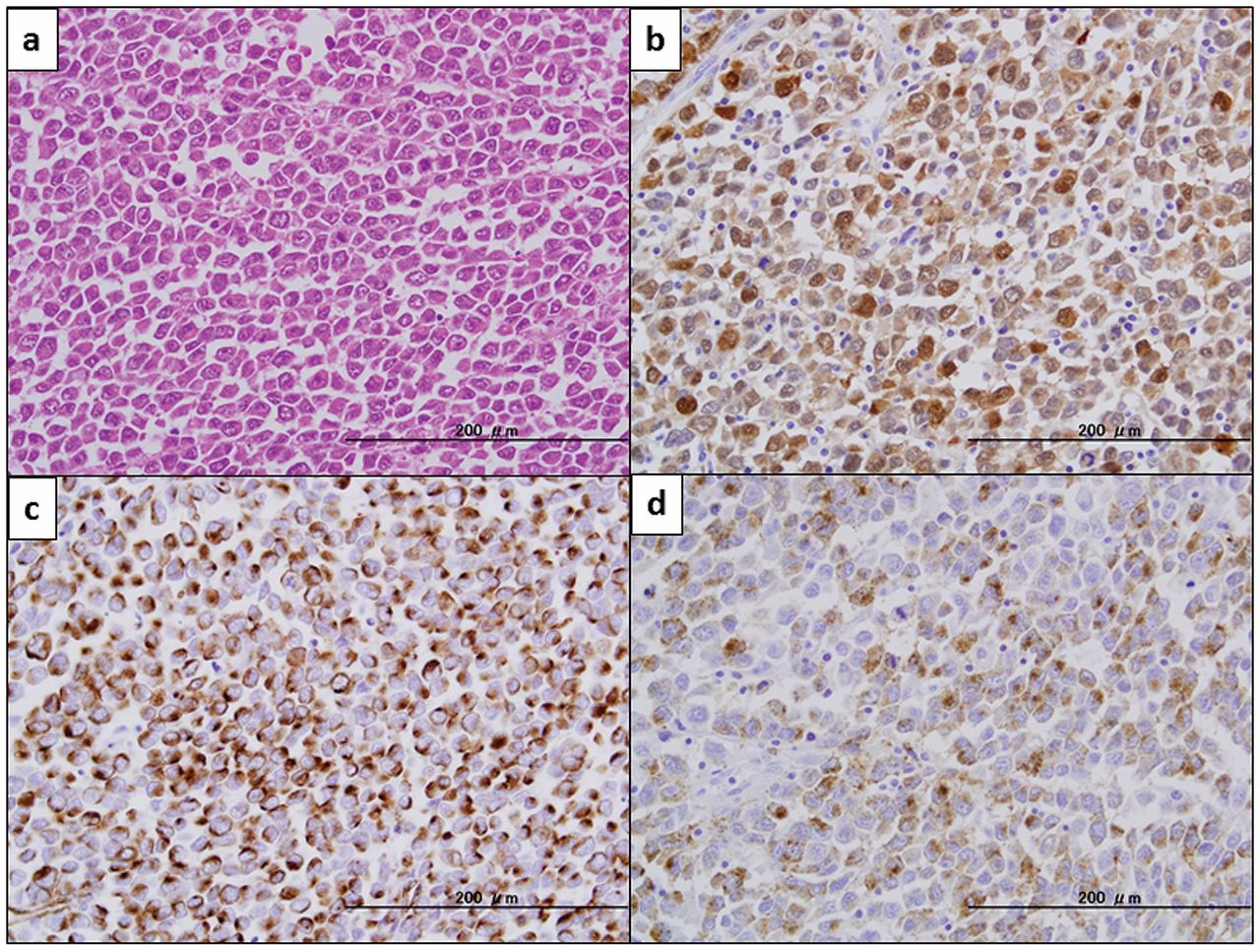
Histopathological appearance of resected tumor. a: Malignant cells with round to oval nuclei and clear nucleoli showed diffuse proliferation (hematoxylin and eosin, ×400). b: Positive immunohistochemical (IHC) staining of S-100 protein (×400). c: Positive IHC staining of vimentin (×400). d: Positive IHC staining with HMB-45 (×400).
Regarding the treatment modality for mucosal melanoma of the head and neck, complete removal with a clear surgical margin is the basic therapy for resectable lesions. As wide surgical resection in the head and neck is often difficult, radiotherapy is important for functionally and cosmetically inoperable cases. Recent reports have shown the same effectiveness in terms of local control by high-dose fractionated radiotherapy in comparison to curative surgery.
Postoperative radiotherapy was considered to be efficient for local control in patients with mucosal melanoma of the head and neck according to the studies by Krengli et al. (34) and Temam et al. (35), although they failed to show a survival benefit. Zenda et al. noted the safety and efficacy profiles of PBT, which provides a better dose distribution than does X-ray irradiation, with a 3-year survival rate of 58.0% for mucosal melanoma of the head and neck (5). Regarding chemotherapy, dacarbazine is often applied for disseminated malignant melanoma but the results have been disappointing, with low response rates (10-20%) and no significant improvement in survival or even lasting symptomatic relief (32, 36). Combination therapy with other drugs (cisplatin, nitrosoureas, taxanes, etc.) or the addition of biological therapy (interferon or interleukin-2) to standard chemotherapy results in a higher response rate but is associated with increased toxicity without significant survival benefit (31-33, 36). Immunotherapy, such as, lymphokine-activated killer (LAK) cell therapy, monoclonal antibodies targeting cytotoxic T-lymphocyte antigens (CTLA-4), or onamelatucel-L (Canvaxin) is also expected, and several trials are ongoing (16, 31, 32, 37). As KIT-activating mutations in mucosal melanoma have been discovered, KIT inhibitors are considered to have potential as effective agents for this aggressive tumor (26).
Pancreatic resection for metastatic melanoma of pancreas collected from English literature.
In summary, the outcome of resection for pancreatic metastatic melanoma originating in the nasal cavity bore comparison with previous cases originating in the skin and ocular region, even though our case showed early recurrence. Although promising effective therapy for disseminated mucosal melanoma, especially of sinonasal origin, is not established, it is unquestionable that aggressive surgical resection produces survival benefit for properly selected patients. Careful examinations, aggressive consideration of surgical intervention, curative resection for indicated cases, and a multidisciplinary approach during follow-up of the primary lesion or even after metastasectomy, are the keys to achieving a better outcome in these patients.
- Received November 21, 2012.
- Revision received December 5, 2012.
- Accepted December 6, 2012.
- Copyright© 2013 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Related Articles
Cited By...
- No citing articles found.