


Abstract
Background: This study aimed to evaluate the necessity for the partial volume effect (PVE) correction of the maximum standardized uptake value (SUVmax) in 18F-fluorodeoxyglucose positron-emission tomography (FDG-PET) for predicting outcome in patients with non-small cell lung cancer (NSCLC). Patients and Methods: A total of 191 patients, with tumor diameters ranging from 10-37 mm, underwent pre-operative FDG-PET and curative resection. The SUVmax (Pre-SUV) of the primary tumor was corrected (Cor-SUV) using a recovery coefficient curve based on phantom experiments. Results: The 5-year overall survival (OS) and disease-free survival (DFS) of the patients with high Pre-SUVs were lower than those with low Pre-SUVs (p<0.001 and p=0.002, respectively). The 5-year OS and DFS of patients with high Cor-SUVs were significantly lower than those with low Cor-SUVs (p<0.001 and p=0.005, respectively). Conclusion: Even without PVE correction, SUVmax was able to predict for outcome in patients with NSCLC.
Lung cancer is the most common malignant disease, and has the highest mortality and morbidity of all types of cancer worldwide (1). In Japan, lung cancer has the third highest morbidity following gastric cancer and colon cancer, and in 2008 mortality due to this disease surpassed that of all other cancers (2, 3). In 2004, the 5-year survival rate for patients with resected lung cancer in Japan was 69.6% (4). When compared with other types of cancer, the outcome of lung cancer treatment is not yet considered satisfactory.
Prognostic factors for non-small cell lung cancer (NSCLC) are tumor size, histological type, lymphatic or vessel invasion, differentiation, nodal involvement, and the standard uptake value (SUV) in 18F-fluorodeoxyglucose positron-emission tomography (FDG-PET) (5-7). Out of these prognostic factors, the SUV is available before treatment and is of considerable clinical importance. The SUV is widely used for the discrimination of malignant and benign lesions, clinical staging of the node factor, prediction of prognosis, and evaluation of the effects of chemotherapy and radiotherapy (8-12). Recently, it was proposed that the SUV might be used for the selection of patients for limited surgery, because it correlates with the aggressiveness of NSCLC (13, 14).
The spatial resolution of PET scanners is low (4-6 mm of the half-maximum full width). The limited spatial resolution of PET scanners does not allow for the resolution of small structures because of the partial volume effect (PVE) (15). The PVE results in an underestimation of the accumulation of radioisotope in tumor (16). This effect is most prominent for small tumors. In clinical practice using FDG-PET, the SUV may be more useful in NSCLC after PVE correction. The aim of the present study was to evaluate the necessity of removing the PVE by correcting the SUV in patients with NSCLC.
Patients and Methods
Patients. Curative resection without induction therapy was performed in 393 patients with NSCLC who underwent preoperative FDG-PET at Hokkaido University Hospital between January 1999 and December 2008. Out of these patients, 191 who had a tumor ranging in size from 10-37 mm in diameter in imaging studies and had undergone systematic lymph node dissection were included in this study. The reason for limiting tumor size to this range was that the data available from the phantom study for correction were limited to spheres of 10-37 mm in diameter, as described later. Patients with cN2 diseases underwent endobronchial ultrasound transbronchial aspiration. Unless pathological diagnosis was multiple-station N2 disease, the patient underwent upfront surgery without adjuvant surgery following our institutional protocol.
The clinicopathological data were obtained from the medical charts. The maximum SUV (SUVmax) of the primary tumor, measured by a nuclear physician using FDG-PET within 90 days prior to surgery, was used in this study. Tumor size in the imaging study was measured by thoracic surgeons on chest computed tomographic (CT) images obtained around the same time as FDG-PET was undertaken. Patients basically underwent a lobectomy with systematic mediastinal lymph node dissection for curative-intent therapy, and sometimes a bilobectomy or pneumonectomy according to the location and extent of the tumor. The following patients underwent segmentectomy with systematic lymph node dissection: elderly patients, patients with deteriorated respiratory function, patients in poor general condition secondary to systemic disease, and patients suspected of having non-invasive cancer such as bronchioloalveolar adenocarcinoma. Video-assisted thoracoscopic surgery (VATS) was performed in all cases except those with chest wall invasion, bronchial invasion or pulmonary vessel invasion.
The clinical and pathological staging was based on the fifth or sixth editions of the Union Internationale Contra le Cancer (UICC) staging system for tumor-node-metastasis (TNM) classification, which was re-classified according to the seventh edition.
Our Institutional Review Board approved this retrospective study (009-0215) and waived the requirement for informed consent.
FDG-PET. Patients had to fast for at least 6 h. Using a whole-body scanner (ECAT EXACT HR+; Asahi-Siemens, Tokyo, Japan), FDG-PET was performed 60 min after injection of 4.5 MBq/kg body weight of FDG. Patients were asked to remain resting and quiet, and to void just before scanning. Scanning was performed from the cranial base to the groin, with a 3 or 4 mm slice thickness and a 10 mm spatial resolution. Scanning encompassed an emission scan (2 min) and a transmission scan (2 min). Image reconstructions were performed using a Fourier rebinning and ordered subsets expectation maximization (FORE OSEM) method with one iteration and 32 subsets. If a localized area with higher uptake than the surrounding normal tissue was present, lesions were considered positive for FDG uptake. FDG uptake was evaluated as the SUV that was calculated by the scanning software using the following formula: SUV=C(mCi/ml)/ID(mCi/kg), where C is defined as the radioactivity at a voxel, and ID is defined as the injected dose per kg of patient body weight.
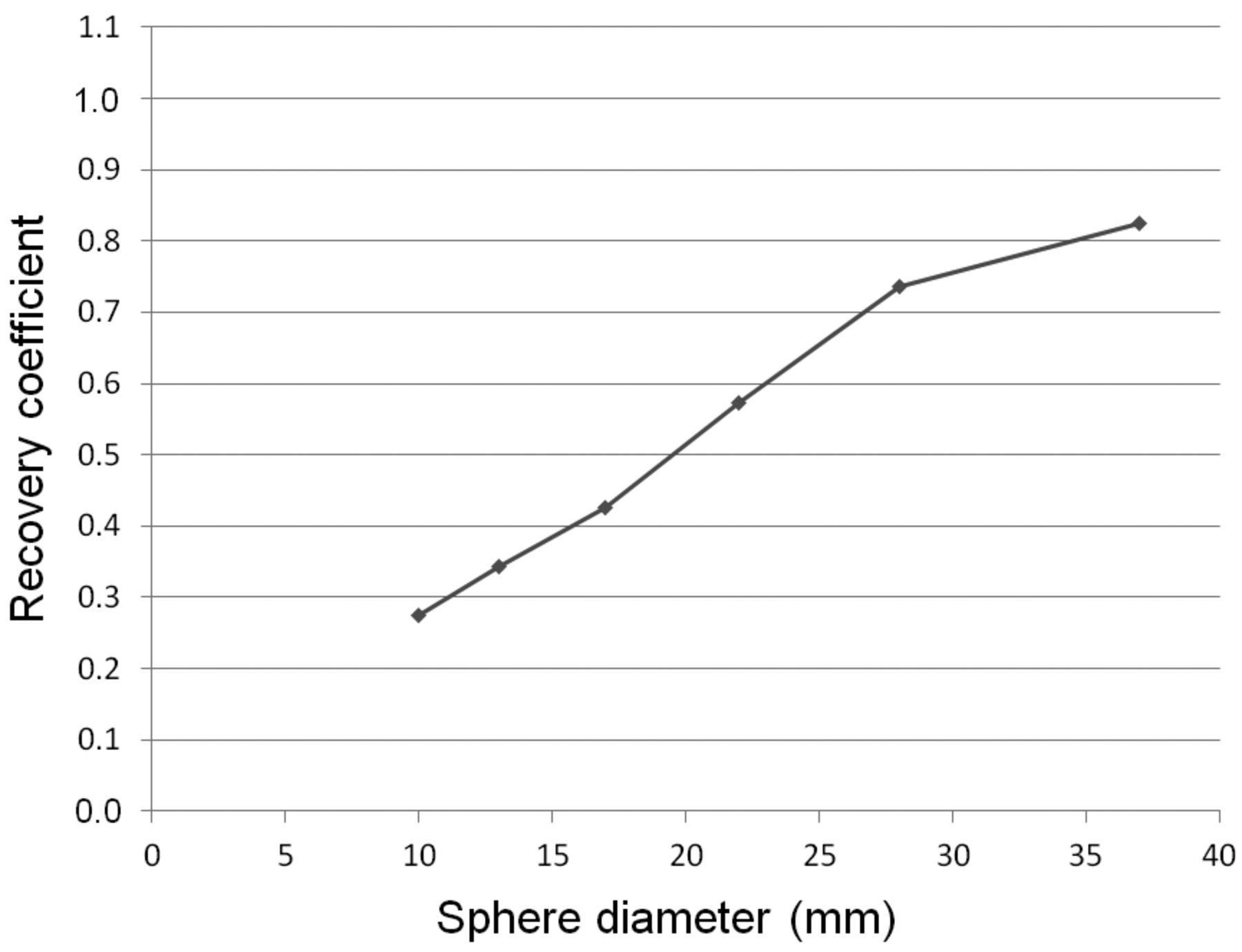
Correction of SUVmax. Firstly the phantom experiment was performed using the PET scanner as detailed above. The cylinder phantom had six different-sized spherical compartments (10, 13, 17, 22, 28 and 37 mm in diameter). The background was filled with 7.3 kBq/ml of FDG. The spheres were filled with 30 kBq/ml of FDG. Scanning was performed seven times with a 2 min emission scan and a 2 min transmission scan. The FORE OSEM method was used for image reconstruction. The uptake of the ‘hot’ spheres and the background of the 6 spheres were measured. Based on these values, the recovery coefficient (RC) curve was evaluated (Figure 1): RC=Measured sphere activity/true sphere activity.
Using the RC curve, the RC was then calculated according to the tumor size measured in the imaging study. Finally, the SUVmax of the primary tumor was corrected using the correction formula: Corrected SUVmax=Normal lung SUVmax + (tumor SUVmax – normal lung SUVmax)/RC (17).
Because the RC curve obtainable in the phantom experiment was sizes ranging from 10-37 mm, patients with tumors that ranged from 10-37 mm in diameter were included in our study.
Statistical analysis. This study examined whether or not the corrected SUVmax of the primary tumor (Cor-SUV) reflected the invasiveness of NSCLC more strongly than the non-corrected SUVmax of the primary tumor (Pre-SUV), using the pathological node factor and patient survival times as end-points. Using a receiver operating characteristics (ROC) curve to predict lymph node metastasis with the SUVmax of the primary tumor, the area under the curves (AUC) were compared before and after PVE correction was applied to FDG-PET (Pre-AUC and Cor-AUC). The overall survival (OS) time was defined as the period between the date of operation and the date of death, or the last date of confirmed survival. The disease-free survival (DFS) time was the period between the date of operation and the date of recurrence, or the last date of confirmed recurrence-free survival. The survival rate was calculated using the Kaplan-Meier method and was compared using the log-rank test. All statistical analyses were performed using Stat Flex (Ver 6; Artech Co., Ltd., Osaka, Japan). A p-value of less than 0.05 was considered to indicate a significant difference.
Results
Patients' characteristics are detailed in Table I. With a median follow-up period of 55 months (range=12-138 months), 53 patients had recurrence, 18 of which were locoregional; 41 patients had distant metastasis and 38 patients died (27 from cancer and 11 from other diseases). The 5-year OS was 79.0% and the 5-year DFS was 69.5%.
All patients had a median Pre-SUV of 2.4 (range=0.5-14.5) and a median Cor-SUV of 4.2 (range=0.5-19.4). Using a ROC curve to predict lymph node metastasis after FDG-PET had been undertaken using the Pre-SUV and Cor-SUV methods, the Pre-AUC was not significantly different from the Cor-AUC (0.809 vs. 0.792; p=0.749; Figure 2).
In patients with adenocarcinoma that did not involved (N−; n=123) or that involved lymph nodes (N+; n=26), the Pre-AUC was not significantly different from the Cor-AUC (0.847 vs. 0.834; p= 0.821; Figure 3a). In patients with N− squamous cell carcinoma (n=26) and N+ squamous cell carcinoma (n=9), the Pre-AUC was not significantly different from the Cor-AUC (0.692 vs. 0.671; p=0.883; Figure 3b).
Similarly, in patients with tumor sizes of ≤30 mm (N−, n=131; N+, n=26), the Pre-AUC was not significantly different from the Cor-AUC (0.804 vs. 0.785; p=0.769; Figure 4a).
The OS and DFS were compared in the 191 patients using the median Pre-SUV and Cor-SUV values as cut-off values (Figure 5). The 5-year OS of patients with a Pre-SUV ≤2.4 was significantly higher than that of patients with a Pre-SUV >2.4 (90.8% vs. 67.1%; p<0.001; Figure 5a). The 5-year OS of patients with a Cor-SUV ≤4.2 was significantly higher than that of patients with a Cor-SUV >4.2 (93.7% vs. 63.3%; p<0.001; Figure 5b). The 5-year DFS of patients with a Pre-SUV ≤2.4 was significantly higher than that of patients with Pre-SUV >2.4 (78.2% vs. 60.5%; p=0.002; Figure 5c). The 5-year DFS of patients with a Cor-SUV ≤4.2 was significantly higher than that of patients with a Cor-SUV >4.2 (76.7% vs. 62.7%; p=0.005; Figure 5d).

Recovery coefficient (RC) curve based on the phantom experiment. The RC was defined as the ratio of the measured sphere activity to the true sphere activity, based on the phantom experiment performed using a cylinder phantom with six different-sized spherical compartments (10, 13, 17, 22, 28 and 37 mm in diameter) filled with 18F-fluorodeoxyglucose.
Discussion
The aim of the present study, using FDG-PET, was to evaluate the utility of PVE correction in relation to predicting the outcome of patients with NSCLC who underwent curative resection without induction therapy. After the phantom experiment involving FDG-PET, the SUVmax of the primary tumor was corrected using the correction formula. Using a ROC curve to predict lymph node metastasis by means of the SUVmax of the primary tumor, the AUC was compared before and after PVE correction. It was found that the SUVmax was an equally strong predictive factor of lymph node metastasis and prognosis, whether with or without PVE correction. Furthermore, OS and DFS times were compared using the median Pre-SUV and Cor-SUV values as cut-off values. The Pre-SUV was shown to be as good a prognostic factor, as was Cor-SUV. Even in the patients with small tumors where FDG accumulation was underestimated because of the PVE, the SUVmax without PVE correction was considered clinically useful.
The SUV is a semi-quantitative parameter regarding uptake of FDG, and has been reported to be a useful prognostic factor for patients with NSCLC. Berghmans et al. reviewed 13 studies and reported that a high SUV was associated with poor prognosis (10). Moreover, the SUV reflects the malignant grade of NSCLC. Vesselle et al. reported that the SUV was associated with tumor proliferation (18). Recently, FDG-PET has become crucial in deciding the therapeutic strategy for patients with NSCLC.
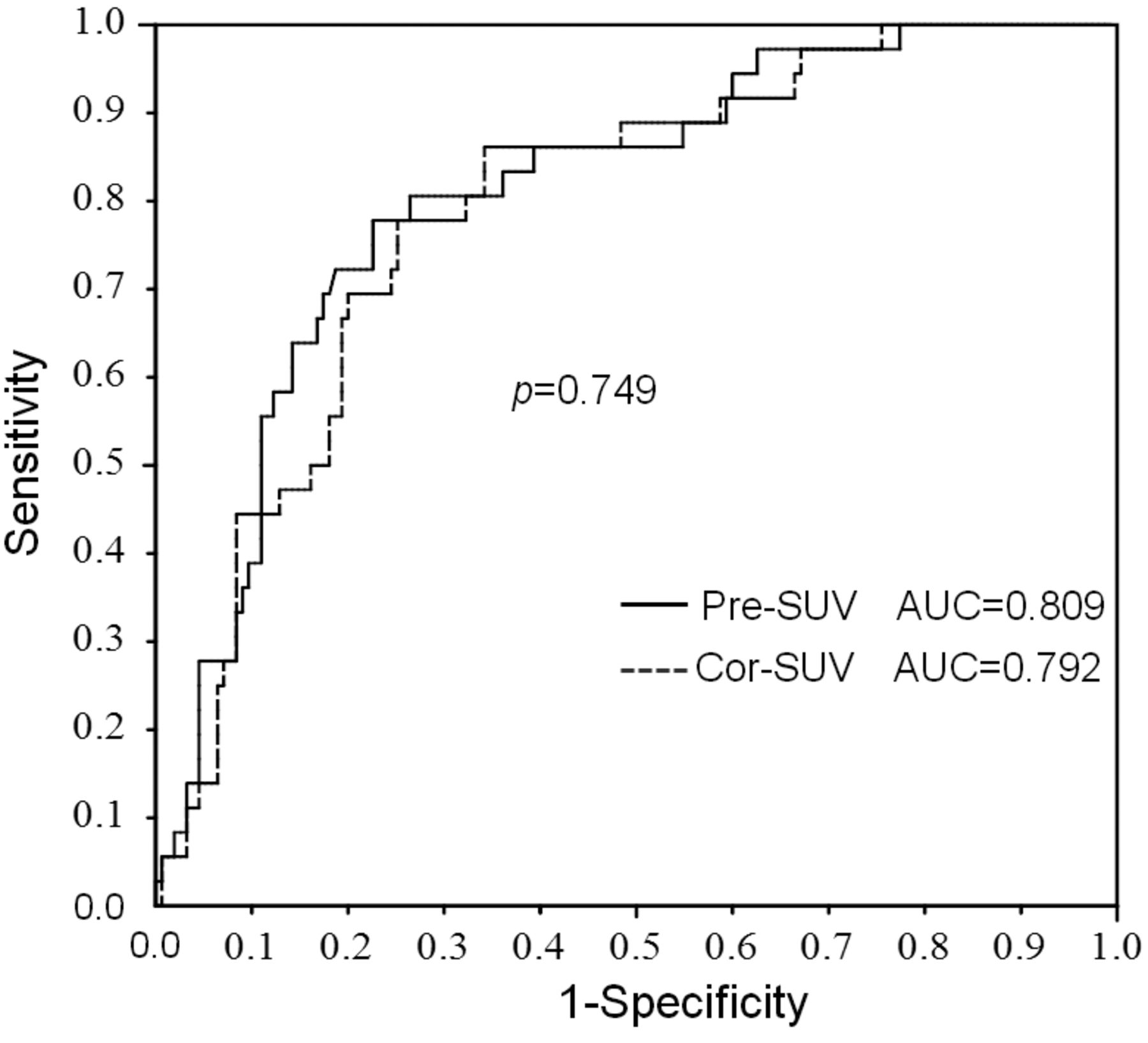
Receiver operating characteristics curve used to predict lymph node metastasis by means of the maximum standardized uptake value (SUVmax) of the primary tumor (Pre-SUV) and corrected SUVmax (Cor-SUV). The area under the curve (AUC) before partial volume effect (PVE) correction was comparable to that after PVE correction.
Patient's characteristics.

Receiver operating characteristics curve used to predict lymph node metastasis by means of the maximum standardized uptake value (SUVmax) of the primary tumor (Pre-SUV) and corrected SUVmax (Cor-SUV) in terms of the histological type. In patients with adenocarcinoma (a) or squamous cell carcinoma (b), the area under the curve (AUC) before partial volume effect (PVE) correction was similar to that after PVE correction.
A number of factors affecting the SUV have been reported (19, 20). Out of these factors, the PVE is a major one that is difficult to correct for in clinical practice. There have been a few reports regarding correction of the SUV in NSCLC. Vesselle et al. carried out three clinical studies involving SUV correction in relation to FDG-PET. In the first study, they reported that the corrected SUV was significantly related to tumor proliferation in 39 patients with NSCLC (18). They indicated in the second study that the SUV could not be used as a prognostic factor, either before or after correction, in 208 patients with NSCLC who underwent pulmonary resection (21). In the third study Vesselle et al. reported that before correction, the SUV was related to the pathological stage, although after correction it was not (22). Our findings are consistent with these studies; in these reports, the SUV was corrected using the RC method in patients with tumors <28 mm in diameter.
In the current study, it was concluded that the SUV without PVE correction was clinically-useful in the assessment of the aggressiveness of resectable NSCLC at a single institute. Because evaluation of the SUV is affected by the instrument model used and its setup, and the reconstruction method and the scanning condition, it can differ even in the same person when FDG-PET is performed at another hospital (23). Thus, it is considered difficult to carry-out a multicenter analysis using the SUV. However, it was recently reported that it may be beneficial to evaluate correction of the SUV in large-scale prospective multicenter studies (24, 25). This is because multicenter analysis allows for accrual of larger patient numbers.
Although the current single-institute study was relatively large, there were several limitations. Firstly, even the diameters of tumors with a long craniocaudal axis were measured in axial section images on CT, and correction using such tumor size measurements led to potential overestimation of the SUV. Secondly, patients with tumors less than 10 mm in diameter were excluded from the study to avoid a stronger influence on PVE. In the RC curve plotted using data from the phantom experiment, data on tumors <10 mm in diameter were not available. Furthermore, correction for the presence of these small tumors was not precise because of the low accuracy of the SUV estimate. This was due to the limited spatial resolution of PET and the high RC, which markedly increased the error in calculating the Pre-SUV. Thirdly, the factors used in the evaluation of tumor aggressiveness were limited to the node factor, and the DFS and OS times. Other factors used for the evaluation of aggressiveness such as lymphatic and vessel invasion, differentiation and tumor proliferation were not available in our study.

Receiver operating characteristics curve used to predict lymph node metastasis by means of the maximum standardized uptake value (SUVmax) of the primary tumor (Pre-SUV) and corrected SUVmax (Cor-SUV) in terms of tumor sizes. In patient with tumor size ≤30 mm (a) or ≤20 mm (b), the area under the curve (AUC) before partial volume effect (PVE) correction was similar to that after PVE correction.

Survival curves and the maximum standardized uptake value (SUVmax) of the primary tumors. Overall survival curves after curative resection before (a) and after (b) correction of the SUVmax in all patients. Disease-free survival curves after curative resection before (c) and after (d) correction of the SUVmax in all patients.
Conclusion
In the current single-institute study, it was concluded that even though there may be underestimation of FDG accumulation due to the PVE, the SUVmax is clinically useful in the assessment of the aggressiveness of resectable NSCLC with diameters in the range 10-37 mm without PVE correction.
Footnotes
-
Conflicts of Interest
We declare that none of the Authors have any conflicts of interest.
- Received September 24, 2013.
- Revision received October 21, 2013.
- Accepted October 23, 2013.
- Copyright© 2013 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.