


Abstract
Aim: To assess the treatment outcomes of chemoradiation for cervical lymph node metastases from an unknown primary site (CUP), and to identify for prognostic factors. Patients and Methods: Thirty patients diagnosed as having CUP, and receiving chemoradiation as a definitive treatment were included in the analysis. Locoregional control (LRC), disease-free survival (DFS), and overall survival (OS) rates were estimated, and the factors affecting treatment outcomes were analyzed. Results: After a median follow-up period of 25 months for surviving patients, the two- and five-year LRC, DFS, and OS rates were 56%/45%, 46%/36%, and 69%/52%, respectively. On univariate analysis, lower performance status (PS; p=0.001), and limitation of disease to level 2 or 3 lymph nodes (p=0.009) were significantly associated with better DFS. Low PS (p=0.002) was significantly associated with better LRC. No late toxicity of grade 3 or greater was observed. Conclusion: Definitive chemoradiation for CUP was well-tolerated, with improvement of DFS/LRC for those with good PS and disease limited to level 2 or 3 lymph nodes.
Cancers of unknown primary sites are defined as a heterogeneous group of metastatic tumors for which a standardized diagnostic work-up fails to identify the site of origin at the time of diagnosis (1). Cervical lymph node metastases from an unknown primary site (CUP) account for approximately 2-9% of all head and neck cancer cases (2, 3). When a thorough investigation, including physical examination, computed tomography (CT), magnetic resonance imaging (MRI), positron-emission tomography (PET), ultrasonography, and panendoscopy, followed by biopsies from suspicious sites, and even tonsillectomy, fail to detect the site of primary lesion, a diagnosis of CUP will be performed. The optimal treatment for these patients remains unclear, as results from randomized comparative trials are lacking; a randomized trial for this purpose conducted by the European Organization for Research and Treatment of Cancer (EORTC) was prematurely closed due to insufficient accrual of patients (4). Although the optimal treatment is unclear, neck dissection followed by postoperative radiation seems to be the most widely accepted approach (5). Therefore, reports concerning the role of chemoradiation as a definitive treatment for CUP are limited. The purpose of this study was to assess the efficacy and toxicities of chemoradiation as the primary, definitive treatment for CUP, and to identify the factors which influence treatment outcomes.
Patients and Methods
Patients' characteristics. Thirty consecutive patients who were diagnosed with CUP at our institutions from 1995 to 2012, and treated with chemoradiation as the primary treatment were included in the present study. The medical records were retrospectively reviewed. Tumor stages were classified using the UICC TNM classification for head-and-neck tumors, seventh edition (6). Patients who were diagnosed with distant metastasis, or were followed-up for less than three months were excluded from the study. All patients underwent thorough examinations, and no obvious primary tumors were detected. Physical examination, panendoscopy, and CT scan were performed for all cases. Most patients underwent CT scans from the neck to at least the chest, and neck MRIs. Twenty-three (77%) underwent PET or PET/CT before diagnosis. All patients had histologically confirmed malignant tumors, and 23 (77%) were squamous cell carcinomas (SCC). All patients were treated with curative intent. The cervical lymph node (LN) levels were determined according to the Danish Head and Neck Cancer Group (DAHANCA), European Organization for Research and Treatment of Cancer (EORTC), Groupe Oncologie Radiotherapie Tete et Cou (GORTEC), National Cancer Institute of Canada (NCIC), Radiation Therapy Oncology Group (RTOG) consensus guidelines (7), referring to the CT of each case. The patient characteristics are summarized in Table I.
Radiotherapy. Radiotherapy (RT) was performed five days per week, with conventional fractionations (1.8-2 Gy per fraction). CT-based, 3-dimensional conformal RT was used in all cases. Intensity-modulated radiotherapy (IMRT) was not performed. The median total dose was 70.2 Gy (range=43.2-74.2 Gy). The median total treatment period was 57 days (range=38-74 days). X-Ray irradiation of 4-15 MV were used for all cases, and 6-11 MeV electrons were used for radiation boost in 21 (70%) cases. All patients received RT to the bilateral neck, including the pharyngeal axis. The initial RT field encompassed bilateral level 1 to 5 LN areas and the retropharyngeal (RP) LNs besides swollen LNs. Prophylactic irradiation of 40-50.4 Gy was administered followed by a radiation boost to the gross tumor volume. An exception was one patient who received RT using antero-posterior opposing fields encompassing the bilateral neck below the mentum, mediastinal and the hilar LNs; the mediastinal and the hilar LNs were included as prophylactic irradiation. This patient received only 43.2 Gy without a radiation boost. As the swollen LNs were located at the lower neck and the histology showed small cell carcinoma, we could not rule out small cell lung cancer as the primary lesion.
Chemotherapy. All 30 patients received chemotherapy, and the majority (29/30, 97%) concurrently. As concurrent chemotherapy, 15 patients received a cisplatin- and 5-fluorouracil-based regimen. Methotrexate and leucovorin, or docetaxel were added. The remaining 14 patients received a platinum-based agent alone, or 5-fluorouracil alone. As neoadjuvant or adjuvant chemotherapy, 5-fluorouracil was administered in most cases.
Follow-up, toxicity assessment, and statistics. All actuarial survival and control rates were calculated from the beginning of RT, using the Kaplan-Meier method. Overall survival (OS) was defined as death from any cause. Disease-free survival (DFS) was defined as the time to the first treatment failure, and locoregional control (LRC) was defined as the time to the first in-field relapse. Toxicities were described by Common Terminology Criteria for Adverse Events (CTCAE) version 3.0 (8). Acute toxicities were defined as toxicities occurring within three months from the beginning of RT, and late toxicities were defined as toxicities occurring later than this.
Statistical analyses were performed using SPSS statistical software (version 19.0; SPSS Inc., Chicago, IL, USA). The Log-rank test was used for univariate analysis to identify prognostic factors which predicted treatment outcomes. Multivariate analysis was not performed due to the small number of patients. A p-value of <0.05 was considered to be statistically significant.
Results
Local control and failure patterns. After the initial treatment, 16 patients (53%) showed complete response, whereas 12 (40%) had progressive disease, and two (7%) stable disease. After a median follow-up of 25 months (range=7-91 months) for surviving patients, the two- and five-year LRC rates were 56% and 45%, respectively. Disease recurrences were observed in 18 (60%) patients after the primary treatment. The recurrences presented inside the radiation field in 15 patients (50% of the whole cohort, 83% of all recurrences), and as distant metastases in five patients (17% of the whole cohort, 28% of all recurrences). Both in-field relapse and distant metastases were seen in three (10%) patients. Among the in-field relapses, twelve were LN metastases, two were emergence of the primary tumor, and one had both. Five patients received salvage surgery after the primary treatment. Four patients received salvage surgery for residual or recurrent tumors inside the radiation field. In one case, the recurrent tumor exhibited postauricular LN metastasis, which was outside the radiation field, and was excised. On the other hand, three patients received re-irradiation to the neck. Two of them had residual or recurrent tumor inside the initial radiation field. In the other case, the primary tumor emerged in the maxillary sinus, which was outside the initial radiation field. This patient underwent re-irradiation of 50 Gy to the maxillary sinus and the neck. Emergence of the primary tumor after the treatment was observed in four (13.3%) cases. The lesions were located at the base of tongue, hypopharynx, thyroid, and maxillary sinus, respectively.
Patients' characteristics.

Overall survival curve of the whole cohort. Median overall survival: 85 months.
Survival. The 2- and 5-year OS and DFS rates were 69%/52%, and 46%/36%, respectively (Figure 1). Twelve deaths were recorded; 11 out of the 12 patients died from disease progression, one patient died from lung cancer, not related to the cervical lesion. The median OS was 85 months.
Prognostic factors. The results of the Kaplan-Meier analysis and the log-rank tests for DFS and LRC are summarized in Table II.
Univariate analysis identified no factor that significantly affected OS. Patients with PS 1-2 had a trend towards poorer OS compared to those with PS 0, but the difference was not statistically significant (p=0.062). However, PS was significantly associated with DFS (p=0.001). In addition, patients with metastatic lesions limited to level 2 or 3 LN areas exhibited a significantly better DFS rate compared to those with involvement of other areas (p=0.009, Figure 2).
PS was also significantly associated with LRC (p=0.002). Patients with emergence of the primary tumor during the follow-up period had a trend toward poorer LRC, but the difference was not statistically significant (p=0.071).
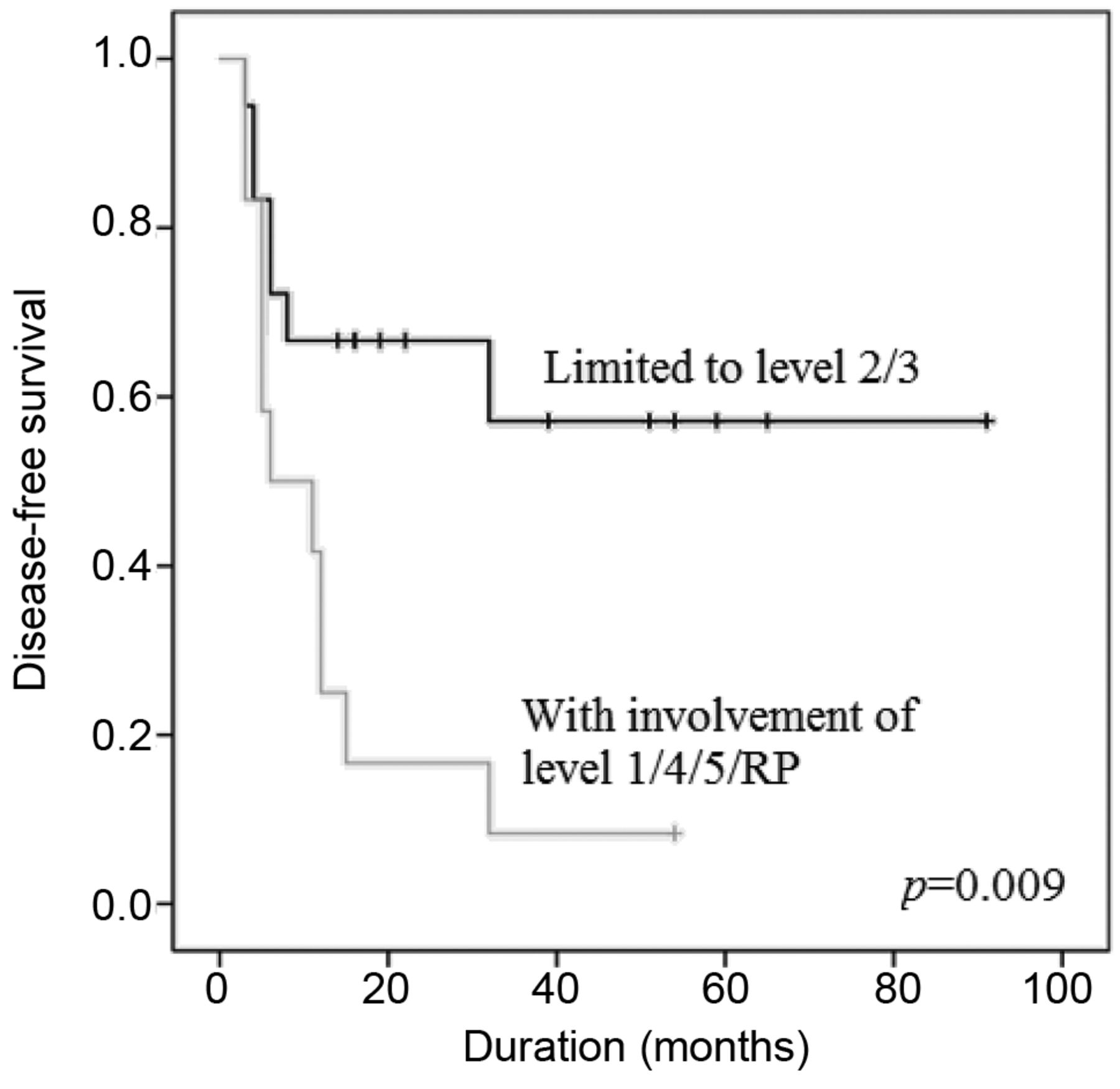
Disease-free survival curves with regard to the level of nodal involvement. Patients with metastatic lesions limited to level 2 or 3 lymph node areas exhibited a significantly better disease-free survival rate compared to those with involvement of other areas.
Toxicities. Treatment-related deaths did not occur. Grade 3 and 4 acute hematological and non-hematological toxicities are summarized in Table III. The most common acute non-hematological grade 3/4 toxicity was mucositis, which was observed in 15 patients (50%). The most common acute grade 3/4 hematological toxicity was lymphocytopenia, observed in 25 patients (83%). All acute toxicities were manageable and temporary. No late toxicity greater than grade 3 was observed. However, 13 patients (43%) complained of grade 2 xerostomia.
Discussion
Although various therapeutic approaches are used for CUP, its optimal treatment has not been yet identified. Cerezo et al. described that although neck dissection followed by RT is the most widely accepted treatment, other curative options exist, which include neck dissection alone, nodal excision followed by RT, or RT alone (5). As neck dissection followed by RT is regarded as the mainstream of curative treatment, most studies assessing treatment outcomes and prognostic factors of CUP include cases treated with surgery. To the best of our knowledge, the present study is the first to report on prognostic factors for patients with CUP treated with definitive chemoradiation.
Fakhrian et al. analyzed the results of 65 patients with CUP of SCC who were treated with RT (79% also received neck dissection). On univariate analysis, extracapsular spread, resection status (R0 vs. R1/R2), involved neck LN level (1-3 vs. 4-5), and Karnofsky index were significant factors for better OS and recurrent-free survival (RFS), and lower nodal stage for OS. On multivariate analysis, R1/R2 resection status and involvement of level 4 LNs were significant factors for poorer OS and RFS (9).
Results of Kaplan-Meier analysis and log-rank tests of prognostic factors for disease-free survival and locoregional control.
In the current study, patients with lesions limited to level 2 or 3 LN areas had better DFS than those with involvement of other areas. To the best of our knowledge, this is the first study to report on this favorable prognostic factor.
Issing et al. analyzed 167 patients with CUP, and evaluated the frequency of the primary tumor origins. The most common origin was the oropharynx (38.9%), including tonsilla palatine and the base of the tongue, followed by hypopharynx (22.3%), nasopharynx (11.1%) and larynx (11.1%) (10). Cianchetti et al. evaluated 236 patients with CUP who had SCC and upper neck presentations, with the bulk of the adenopathy in level 2 or 3. After thorough examination, occult primary sites were detected in 53.4%, and the most common sites were the tonsillar fossa (44.7%) and the base of the tongue (43.9%) (11). According to these reports, CUP seems to include a substantial number of lesions originating from the oropharynx or hypopharynx. It is reported that oropharyngeal and hypopharyngeal carcinomas have the propensity to metastasize initially to level 2 followed by 3, and isolated ‘skip’ metastases are rare (12, 13). Assuming that the origins of the LN metastases are those sites, it is possible to consider that cases with metastatic lesions limited to level 2 or 3 areas have relatively early-stage disease compared to those with involvement of other LN areas. This interpretation may account for the favorable DFS rates for those cases on univariate analysis. However, the difference should be proven to be significant on multivariate analysis, which requires a larger cohort; in addition, a longer follow-up is required to validate this hypothesis.
There are few reports with respect to the use of definitive chemoradiation against CUP. Shukla et al. analyzed 140 patients who were initially treated with either concurrent chemoradiation or RT alone. Patients receiving surgery as the primary treatment were not included in their analysis. The results showed improved response rates along with improved DFS and OS for patients treated with chemoradiation. They reported a median OS of 21.5 months for the radiation-alone group, and 43 months for the chemoradiation group (14).
Grade 3 and 4 acute toxicities experienced under treatment with chemoradiation for patients with CUP.
We report on a 5-year OS rate of 52% and a median OS of 85 months. These rates are in the range of other studies (4, 9, 14-16). Szutkowski et al. analyzed 90 patients with CUP who received various treatment modalities, including surgery and postoperative RT, primary chemoradiation, and RT alone. The 5-year OS rate was 24% for the entire cohort. In the group undergoing surgery and RT, the rate was 43%, whereas those undergoing chemoradiation or RT alone it was only 2% (15). However, it is difficult to compare since their cohort mainly consisted of patients with advanced diseases, e.g. 63% of N3 disease (and N2a-N2c for the rest), and selection bias is unavoidable even inside the cohort. Beldi et al. also reviewed data from 113 patients with CUP who were treated with RT with or without surgery (52% received surgery). They reported on 5-year OS rates of 40.7% for the entire group and 46.6% for the SCC subgroup (4). In general, previously reported 5-year OS rates from retrospective studies ranged between 0 and 67% (9). Our treatment outcomes demonstrated no inferiority to these studies, which mainly consist of patients who underwent surgery and postoperative RT.
In the current study, the majority (82%) of the recurrences occurred inside the radiation field. Improvement in LRC is therefore required. Options to be considered include IMRT. This technique is reported to improve dose homogeneity (17, 18), and a rise in the LRC rates is expected. Villeneuve et al. presented data of 25 patients with CUP treated with IMRT and chemotherapy, with or without surgery. In spite of the same median total radiation dose as our study (70 Gy), 84% of the patients achieved complete nodal response. Patients with incomplete nodal response after IMRT underwent planned neck dissection, and the subsequent 3-year OS, DFS, and LRC rates were all 100% (3).
In our study, the common acute hematological toxicities were lymphocytopenia, leukocytopenia, and neutropenia, which are possibly due to both RT and chemotherapy. They were all manageable and improved by either watchful waiting or the use of granulocyte colony-stimulating factor. Mucositis and dermatitis were the common acute non-hematological toxicities, which were also all manageable and temporary.
In conclusion, the treatment outcomes of CUP treated with definitive chemoradiation were in line with previously reported studies which included patients who underwent surgery and postoperative RT. However, locoregional relapses were common, requiring improvement in LRC. Toxicities were acceptable and well-tolerated. Several prognostic factors, including metastases limited to level 2 or 3 LNs as a newly-suggested factor, were implied. Larger clinical studies to validate these results are warranted.
- Received September 5, 2013.
- Revision received October 14, 2013.
- Accepted October 15, 2013.
- Copyright© 2013 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.