


Abstract
Background: Chemotherapy given every third week is currently the mainstay in the treatment of metastatic breast cancer (MBC). However, bi-weekly dosing might offer a better dose intensity, with better tolerability and response rates. This hypothesis was tested in a phase II study on bi-weekly paclitaxel combined with capecitabine. Patients and Methods: Nineteen patients [median age was 60 (range: 43-68) years] with MBC were treated with paclitaxel (Taxol®) 120 mg/m2, with 1-h infusion on days 1 and 15, and capecitabine (Xeloda®) 2650 mg/m2/day orally given at two doses on days 1-7 and 15-21 on a 28-day cycle. Metastatic sites included the bone (68%), lung (63%) and liver (47%), and 95% of patients had more than one sites of metastasis. Results: In the response evaluation, one complete and 12 partial responses (overall response rate 68%), two stable disease cases and two progressive disease cases were observed. The median duration of response was 13.4 (range: 3.9-43.5) months. Progression-free and overall survival were 13 (95% CI=10.8-15.3) months and 23 (95% CI=17.7-29.1), respectively. A total of 140 (median 8, range 1-28) cycles were delivered. Grade 3-4 toxicity was uncommon: neutropenia was observed in 5% of the cycles; pulmonary problems in 1.4%; pain in 1.4%; and hand-and-foot syndrome, tiredness and arthralgia/myalgia, each in 0.7% of the study treatment cycles. Conclusion: Bi-weekly dosing of paclitaxel and capecitabine seems to yield promising responses in advanced breast cancer, with an acceptable adverse-event profile.
In several studies, including a Finnish multi-center trial and a recent meta-analysis, weekly paclitaxel has proven to be a well-tolerated and effective treatment for advanced breast cancer (1-6). In addition, a newer cytotoxic agent, capecitabine, an oral pro-drug of 5-fluorouracil, has been shown to be active in both early and metastatic breast cancer (MBC) (7-12). Capecitabine is metabolized in the liver and in cancerous tissues. The final step of conversion to fluorouracil is catalysed by thymidine phosphorylase, which has been shown to be present at high concentrations in breast tumours (13). Docetaxel, paclitaxel and cyclophosphamide administration has been shown to increase the tumour-tissue thymidine phosphorylase concentration in xenograft models, suggesting that these agents might act in a synergistic fashion with capecitabine (7, 9, 12). A combination of docetaxel and capecitabine in a 3-week schedule was proven to be effective in the treatment of both MBC (response rate of 42%) and early breast cancer (13-14).
Bi-weekly dosing of paclitaxel either alone or in combination with gemcitabine and doxorubicin or cisplatin has been evaluated in the treatment of advanced breast cancer (15-17), with a response rate of up to 85%. Higher dosing of capecitabine (“dose-dense”) combined with oxaliplatin was shown to be more effective than normal dosing in advanced colorectal cancer (progression-free survival of 11 vs. 6 months, p=0.0013) (18). Haematological toxicity was equal between groups, but diarrhoea was more pronounced at the normal capecitabine dose (44% vs. 31%). In contrast, hand-and-foot syndrome was slightly more frequent at the higher dose of the drug (22% vs. 31%).
The primary end-points of this single-institute study were efficacy, tolerability and progression-free survival for a dose-dense treatment schedule of bi-weekly paclitaxel combined with capecitabine.
Patients and Methods
Patients. In this phase II trial, 19 patients with histologically- or cytologically-proven, evaluable or measurable MBC were enrolled. Other major inclusion criteria were no more than two previous chemotherapy regimens for metastatic disease; Eastern Co-Operative Group (ECOG) ≤2 or Karnofsky score ≥70%; expected survival of more than 3 months; no chemotherapy for 3 weeks; neutrophils ≥1.5; thrombocytes ≥100; creatinine ≤1.5× the upper normal limit (UNL); bilirubin or/and alanine transferase (ALAT) ≤3× UNL, except in the case of liver metastases; bilirubin <60 μmol/L and/or ALAT <5× UNL. Major exclusion criteria were other malignancy; brain metastases; a major heart disease within 6 months, such as heart infarction; motor neuropathy >2 WHO; previous treatment with paclitaxel or capecitabine; current infection; and mental disorder preventing written informed consent. Known Her-2-positive patients without earlier trastuzumab treatment received first-line treatment with trastuzumab. The patients' baseline characteristics are shown in Table I. The study was approved by the Ethical Committee of Tampere University Hospital (R04082M). All patients were informed and signed the patient informed consent form.
Treatment schedule. Pre-medication for paclitaxel included dexamethasone (10 mg i.v. 30 min beforehand), cetirizine (10 mg orally 30-60 min beforehand) and ranitidine (50 mg i.v. 30-60 min beforehand). Paclitaxel (Taxol®) 120 mg/m2, with a 1-h infusion on days 1 and 15, and capecitabine (Xeloda®) 2650 mg/m2/day orally as two doses on days 1-7 and 15-21 were given on a 28-day cycle.
Evaluation of response and toxicity. Each patient's medical history was recorded at baseline, and physical examinations and laboratory measurements were performed. Pre-treatment evaluation of disease staging was performed using computed tomography and bone scanning. The tumour response was evaluated according to the RECIST criteria every 8 weeks using computed tomography (19). These responses were confirmed within 4 weeks. Toxicities for every treatment cycle were evaluated according to the National Cancer Institute Common Terminology Criteria for Adverse Events (NCI-CTCAE), version 3.0 (http://ctep.cancer.gov/reporting/ctc.html). Briefly, the guidelines for dose modification were as follows. If grade 3-4 neutropenia or thrombocytopenia occurred, treatment was postponed for 1 week (allowing recovery to grade 0-2), the dose of paclitaxel was reduced to 100 mg/m2, and capecitabine was also postponed until recovery to grade 0-2. Reduction of paclitaxel was allowed to the level of 60 mg/m2. In the case of capecitabine-related grade 2-3 toxicity, the dose of capecitabine was decreased to 75% the initial dose, and in the case of grade 4 toxicity, the dose reduction after recovery was 50%. If the same toxicity occurred for a second time at the grade 2-3 dose, the dose reduction of capecitabine was 50%. In addition, if grade 2-3 toxicity occurred for a third time or grade 4 toxicity occurred for a second time, treatment with capecitabine was stopped.
Results
Patients. The median age was 60 (range: 43-68) years. Metastatic sites included the bone (68%), lung (63%) and liver (47%), and 95% of patients had more than one site of metastasis (Table I). Only 16% of patients had not undergone previous treatment for metastatic disease, while approximately half of patients had received taxanes or anthracyclines (Table I).
Efficacy. In the response evaluation, one complete and 12 partial responses (overall response rate of 68%), two stable disease cases and two progressive disease cases were observed (Table II). The median duration of the response was 13.4 (range: 3.9-43.5) months. The median duration of progression-free survival was 13.0 months (95% CI=10.8–15.3) and the median survival time was as long as 23.4 months (95% CI=17.7-29.1) (Figures 1 and 2).
Patients' baseline characteristics.
Side-effects. A total of 140 (median 8, range:1-28) cycles were delivered. Grade 3-4 toxicity was uncommon: Neutropenia was observed in 5% of cycles; pulmonary problems in 1.4%; pain in 1.4%; and hand-and-foot syndrome, tiredness and arthralgia/myalgia, each in 0.7% of the study treatment cycles (Table III).
Discussion
A high response rate and a long response duration, along with an acceptable toxicity profile, were shown in this pilot trial. Severe Grade 3-4 side-effects were recorded in less than 2% of the cycles, except for a 5% rate of neutropenia. In earlier studies, the dose-limiting toxicity of paclitaxel given every third week was neutropenia. Grade 3-4 neutropenia has been recorded in 65% of patients. In addition, 40-50% of patients complained of myalgia and arthralgia. Due to these side-effects, weekly paclitaxel is often used and well-tolerated (5, 6). Bi-weekly dosing is another option that allows docetaxel to be better-tolerated, resulting in significantly longer progression-free and overall survival in advanced castration-resistant prostate cancer in a recent study of our group (20). To develop better-tolerated and more effective combinations for treatment of advanced cancer, we tested bi-weekly dosing in advanced breast cancer. Capecitabine alone or combined with taxanes in a tri-weekly dosing schedule has been widely used in the treatment of advanced breast cancer and widely studied in randomised trials (11, 13, 14). According to the present pilot study, testing a bi-weekly combination of paclitaxel and capecitabine in randomised studies seems to be a viable option.
Primary end-point results of bi-weekly paclitaxel and capecitabine.
Most common adverse events during the 140 cycles of treatment. Numbers are % of the treatment cycles.

Kaplan-Meier progression-free survival curve from the start of treatment.
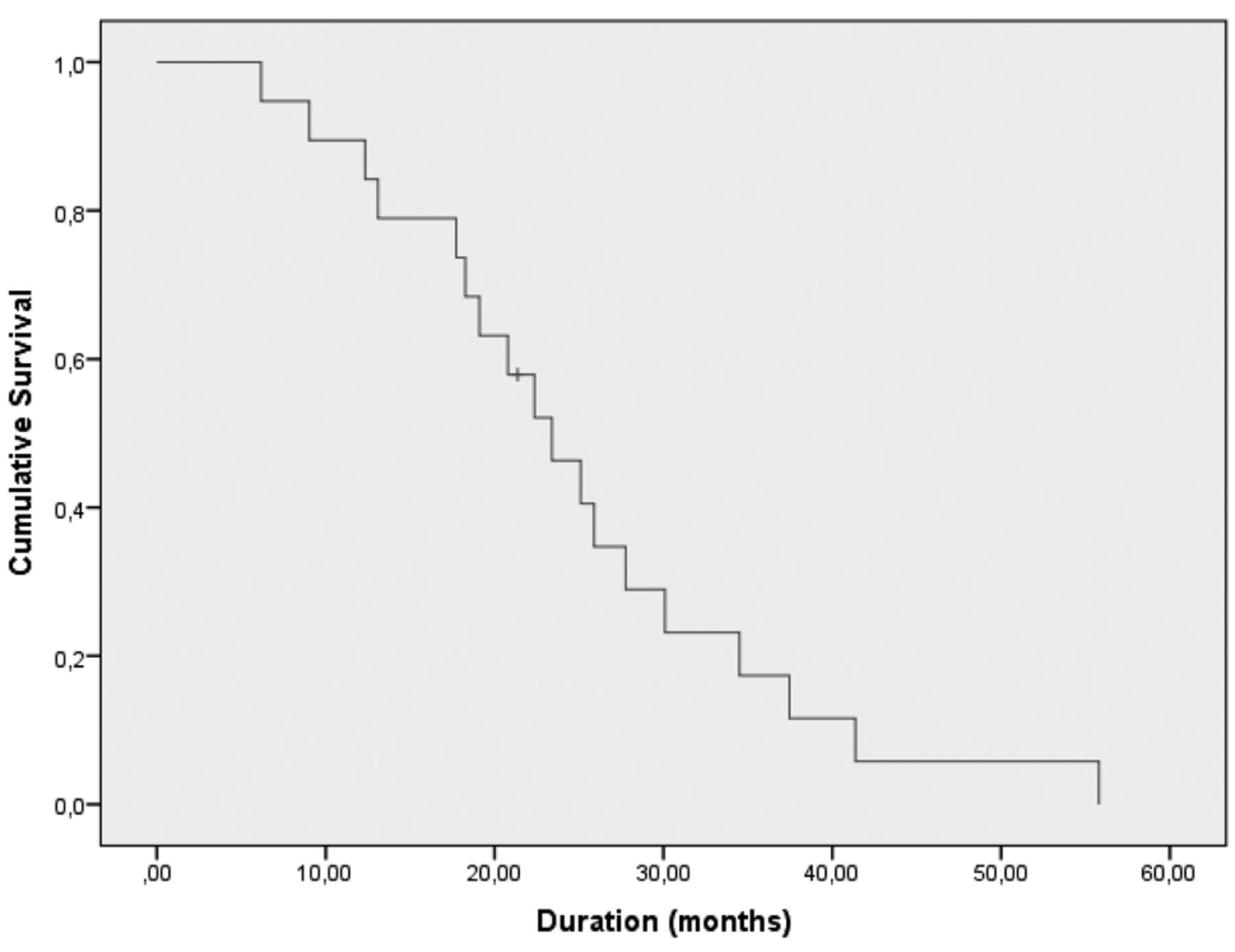
Kaplan-Meier survival curve for all patients from the start of treatment.
Paclitaxel alone has also been shown to be well-tolerated. In an earlier phase I/II study, paclitaxel was started at a dose of 100 mg/m2, and the highest tolerated dose of paclitaxel was 160 mg/m2 bi-weekly. At the highest dose, the response rate, 67%, was very similar to ours (21). In another phase I-II study (n=20) with bi-weekly paclitaxel at a dose of 120 mg/m2 as a second-line treatment after anthracyclines or docetaxel, one complete and eight partial responses were observed, (OR=45%). Treatment tolerability was as good as for weekly paclitaxel (22). The bi-weekly dosing of paclitaxel might also be more cost-effective because fewer patient visits to the oncology unit are required.
When paclitaxel was combined with other cytostatic agents in the treatment of advanced breast cancer, the bi-weekly dose of paclitaxel varied from 90-135 mg/m2, which is why we chose to use paclitaxel 120 mg/m2. In those studies, the response rates have been very high: paclitaxel + cisplatin, 85% (21), and paclitaxel + doxorubicin + gemcitabine, 83% (CR=44%) (23). In addition, several studies have demonstrated the efficacy of capecitabine in the treatment of advanced taxane- or anthracycline-resistant breast cancer (13, 24). In two phase II studies, a combination of paclitaxel and capecitabine with the normal triweekly schedule (paclitaxel on day 1 at 175 mg/m2 and capecitabine on days 1-14 two times daily at 1000 mg/m2 or 825 mg/m2) yielded an objective response rate of 51% and median progression-free survival of 8.1 and 10.5 months, respectively (25, 26). In a randomised study, docetaxel combined with capecitabine was superior to docetaxel alone in terms of response rate, progression and overall survival (13), but we chose paclitaxel for our combination due to its good tolerability in weekly dosing.
Dosing of capecitabine was based on the results of a colorectal cancer trial (18). Before the current trial, the 1-week dosing of capecitabine was used only in this colorectal cancer trial, which included a two-dose level of capecitabine combined with oxaliplatin. In the other treatment arm, capecitabine was used at a daily dose of 3500 mg/m2 for 1 week, followed by 1 week off. The dose of oxaliplatin was 85 mg/m2 bi-weekly. In the other treatment arm, capecitabine was used at a daily dose of 2000 mg/m2 for 14 days, and the dose of oxaliplatin was 130 mg/m2 tri-weekly (21-day cycle). Thus, in the bi-weekly arm, the dose intensity of capecitabine was 31% higher than in the normal tri-weekly dosing arm. More responses were observed in the bi-weekly arm compared with the tri-weekly arm (54.5% vs. 42.2%), and the median progression-free survival was significantly higher in the dose-intensive arm (10.5 vs. 6.0 months, p=0.0013). Diarrhoea was more common with the normal dosing, and hand-and-foot syndrome was more common with the dose-dense schedule. In the present study, mild hand-and-foot syndrome was common, but severe hand-and-foot syndrome was recorded in only 0.7% of the cycles. The most common toxicities were neuropathy and tiredness, but these effects were usually mild. Alopecia was nearly universal (18). Thus, in the present study, we chose a higher dose of capecitabine for the 1-week dosing schedule.
In conclusion, in addition to a good response rate (67%) and adequate tolerability, both progression-free and overall survival were long in this pilot study, which might be due to the metronomic dosing of both drugs. The bi-weekly dosing of paclitaxel seems to be convenient for the patients and it also saves resources in the out-patient clinics. These findings need to be confirmed in larger randomised studies.
Acknowledgements
The Authors would like to thank the research nurses and Roche Inc.
- Received September 18, 2013.
- Revision received October 10, 2013.
- Accepted October 14, 2013.
- Copyright© 2013 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.