


Abstract
Aim: To determine the maximum tolerated dose of hypofractionated radiotherapy (HFRT) plus concurrent metronomic chemotherapy in patients with hormone-refractory prostate cancer (HRPC). Patients and Methods: A Phase I clinical trial was performed with cohorts of three to six patients per group. Eligible patients had HRPC without distant metastases. The radiotherapy dose was escalated in a stepwise fashion as follows: 60, 65, and 70 Gy at levels 1, 2, and 3, respectively (25 fractions: levels 1-2, and 26 fractions: level 3). Results: Nine patients were enrolled. The radiotherapy dose was escalated from 60 to 70 Gy without any dose-limiting toxicity. The most common grade 1/2 toxicities were hematuria, dysuria, diarrhea and rectal-perirectal pain. The overall objective response rate was 9/9 (100%) (95% CI=66.4%-100%). The median time-to-progression was 19 months. Conclusion: In the challenging setting of HRPC, HFRT up to 70 Gy with concurrent metronomic chemotherapy was well-tolerated and yielded encouraging disease control.
Radiotherapy (RT) represents an important therapeutic option for non-metastatic prostate cancer (1). Furthermore, patients with intermediate and high-risk disease benefit from the integration of RT with androgen-suppressive therapy (AST) (2, 3). Another treatment option in non-metastatic prostate cancer is represented by AST alone (1). However this therapeutic modality is associated with a higher incidence of recurrences, especially in the pelvic region. Treatment of patients with pelvic recurrence during AST is problematic (4). RT is effective in palliating locally recurrent or progressive hormone-refractory prostate cancer (HRPC) (5, 6), with a better loco-regional control if doses higher than 60 Gy are delivered (5). Unfortunately the majority of these patients would be expected to develop distant metastasis and subsequently die of disease soon after referral for RT (5). The local effect of RT cannot be increased by AST because of the refractory nature of these tumors. Moreover, no significant effect on microscopic metastatic disease can be expected. Concurrent chemotherapy may represent an alternative possibility of intensification of RT in these patients. However, only few studies have been performed with this therapeutic modality in prostate cancer. In addition, some studies reported a high degree of toxicity by combining RT with either 5-fluorouracil (7) or docetaxel (8).
The anti-tumor and anti-angiogenic activity of chronic administration of cyclophosphamide (CTX), at low doses with no prolonged drug-free breaks, has been shown in various experimental models of human prostate cancer (9). Phase II clinical studies have obtained interesting results using metronomic oral CTX in combination with dexamethasone (10) in patients with HRPC. Metronomic CTX was safe and well-tolerated with a prostate-specific antigen (PSA) decline of more than 50% in 22/32 (69%) of patients with response duration of eight months (10). This very high tolerability could theoretically facilitate the association of metronomic chemotherapy with RT.
A further subject of interest is the mechanism of action involved in the combination of RT with metronomic chemotherapy. In fact, metronomic chemotherapy is effective in preventing tumor angiogenesis (11) and RT has been shown to kill proliferating endothelial cells, suggesting that inhibiting angiogenesis may sensitize endothelial cells to the effects of radiation (12). Moreover, targeting the vasculature may paradoxically increase oxygenation within tumors, thereby enhancing RT efficacy (12). Finally, it has been observed that the use of RT for cancer is also associated with therapeutic challenges that are distinct from those that might be expected with antiangiogenic agents. Thus, the use of angiogenesis inhibitors in combination with RT should help overcome limitations, leading to enhanced efficacy and diminished toxicity (12).
However, experience of the association between metronomic chemotherapy and concurrent RT is scarce (13, 14). In particular, it is not known whether metronomic chemotherapy may be safely combined with standard doses of RT to the pelvis. Based on these premises, the purpose of this study was to evaluate the feasibility of a combined treatment of external-beam RT with CTX-based metronomic chemotherapy in patients with pelvic relapse of HRPC during AST.
Patients and Methods
Study characteristics. The study was conceived as a prospective dose-escalation study. All patients consecutively followed at our Radiotherapy Unit matching the inclusion criteria were enrolled. The trial was approved by the Institutional Review Board (# 01-2011).
Study objectives. The primary study end-point was the definition of the maximum tolerated dose (MTD) of RT combined with a fixed dose of metronomic chemotherapy. Secondary objectives of the study were the overall response rate (ORR) and progression-free survival.
Radiotherapy dose escalation. Patients were sequentially assigned to a specific dose level as detailed in Table I. RT dose escalation was based primarily on acute and subacute toxicity because late toxicity can occur months or years later. Acute-subacute toxicities were defined as those that occurred within six months from treatment. Toxicities registered at least six months after RT were defined as late toxicities. Dose-limiting toxicities (DLTs) were defined as any treatment-related non-hematological adverse effects rated as grade 3 or more, any hematological toxicity rated as grade 4 or more by National Cancer Institute Common Terminology Criteria for Adverse Events version 4.03 (CTCAE v.4.03) (15). If no DLT was not observed in any of the three patients at a given dose level, the trial proceeded to the next dose level, provided that at least three months of follow-up had occurred following RT for the third patient of the cohort. If a DLT occurred in one of the three patients at a given dose level, treatment of up to three additional patients at this dose level was required. If a DLT occurred in more than one patient of the three-patient cohort, dose escalation would stop, and the dose level below that would be considered as the MTD. If a DLT occurred in two or more patients of the expanded six-patient cohort, dose escalation would stop and the dose level below that would be considered as the MTD. If a DLT occurred in fewer than two patients of the expanded six-patient cohort, the trial proceeded to the next dose level. A 70-Gy total RT dose was selected at study initiation as the highest dose level to be evaluated considering the use of hypofractionated treatment. Late toxicities were continuously monitored even if patients showed disease progression.
Inclusion criteria. The following inclusion criteria were used: histological diagnosis of prostate adenocarcinoma, HRPC as evidenced by two consecutive (one-month interval) increases in PSA level in spite of a testosterone level in the castrate range and no distant metastases. When on an anti-androgen, withdrawal was attempted before inclusion and only patients who demonstrated progression after discontinuing this class of agent with at least a 50% increase in the PSA or objective evidence of increasing disease, were included. There was no limitation in the number of prior hormonal manipulations. Chest radiographs, computed tomography (CT) of the abdomen and pelvis, bone scan, PSA level and an electrocardiogram were performed at baseline. Other inclusion criteria were age >18 years, Eastern Cooperative Oncology Group (ECOG) performance status 0-2, adequate bone marrow function defined as follows: neutrophil count >1,500/μl, platelets > 100,000 ml, hemoglobin >9 g/dl, creatinine <1.8 mg/dl, total bilirubin <3mg/dl, lactate dehydrogenase (LDH) <3 normal value, aspartate aminotransferase (AST) <3 normal value, alanine aminotransferase (ALT) <3 normal value, alkaline phosphatase <3 normal value. Previous treatment with prostatic surgery was accepted.
Patients' characteristics (n=9).
Exclusion criteria. The following exclusion criteria were used: ECOG performance status >3; previous pelvic RT; presence of medical conditions which contraindicated radiation therapy: connective system disorders, acute diverticulitis, ulcerative colitis, pelvic inflammatory disease; comorbidities that in the opinion of the referring physician constituted a risk to clinical trial participation.
End-points and statistical analysis. Toxicity was evaluated by CTCAE v.4.03. Biochemical response and PFS were calculated based on the Prostate-Specific Antigen Working Group recommendations for outcome guidelines in Phase II trial (Table II) (16). The survival curves were calculated with the Kaplan-Meier method. Statistical analysis was performed with SYSTAT, version 11.0 (SPSS, Chicago, IL, USA).
Prostate specific antigen (PSA) response outcome definitions.
Radiotherapy. Treatment was simulated and performed with the patient in supine position. Patients were instructed to achieve stable conditions of bladder and rectal filling. Before CT simulation and each therapy fraction patients were invited to empty the bladder two hours prior to the procedure and drink 2 glasses of water right after; empty the bowel over the two hours prior to the procedure. As immobilization systems, a vac-lock and a lower-limb support were used. RT was planned based on CT simulation performed after oral administration of contrast with 5-mm slice intervals. The clinical target volume 1 (CTV1) included the prostate and seminal vesicles in patients with tumors not previously resected and local recurrence plus prostatic bed in patients previously treated by radical prostatectomy. CTV2 was defined as CTV1 plus pelvic lymph nodes (presacral, obturator, internal iliac and external iliac chains). The planning target volume 1 (PTV1) and the PTV2 were defined by adding an 8 mm margin (6 mm posteriorly) to CTV1 and CTV2, respectively. Intensity-modulated radiotherapy (IMRT) plans were generated using the Plato inverse treatment planning system (Plato B.V., Veeuendaal, the Netherlands). A class solution based on five co-planar beams consisting of different gantry angles (36°, 108°, 180°, 252°, 324°) was selected. In treatment plan calculation, the International Commission on Radiation Units and Measurements (ICRU) 62 recommendations were followed and QUANTEC dose-volume constraints (17) were respected. A daily online correction protocol of isocenter position was applied using portal imaging with set-up correction in case of deviations >0.3 cm in any direction (18). All stages of the treatment planning process were subjected to a systematic independent check procedure, as previously described (19). A dose of 45 Gy to the PTV2 (1.8 Gy/fraction) was prescribed to all patients. The following doses were prescribed to PTV1: level one: 60.0 Gy in 25 fractions (25 fractions of 2.4 Gy); level two: 65 Gy (25 fractions of 2.6 Gy); Level three: 70 Gy (25 fractions of 2.6 Gy followed by a fraction of 5 Gy delivered to the prostate or site of recurrence only).
Concurrent chemotherapy. Chemotherapy started one month before the start of RT, and was discontinued one month after the end of RT. Patients received cyclophosphamide (50 mg every morning) and dexamethasone (1 mg every evening), orally.
Follow-up. A first clinical examination was performed 20 days following the end of RT for a complete evaluation of acute toxicity. Thereafter, patients were followed-up bi-monthly assessing treatment toxicity and prostate carcinoma control, based on history, physical examination, and PSA levels. Bone scans were obtained for the assessment of bone pain.
Results
A total of nine patients with locally-progressive HRPC were enrolled. The patients' characteristics are listed in Table I. The median age was 74 years (range=68-83 years). There were five primary and four recurrent cases after radical prostatectomy for HRPC. Two patients had metastatic involvement of pelvic lymph nodes. In all patients, anti-androgen withdrawal after total androgenic blockage had failed. The median follow-up time was 12 months (range=6-41 months). The most common grade 1/2 toxicities were hematuria, dysuria, diarrhea and rectal-perirectal pain, which were tolerable and manageable (Table III). No patient experienced any DLT and the RT dose was escalated from 60 to 70 Gy. The MTD was not reached until level 3 (Table IV). The objective ORR was 9/9 [100%; 95% confidence interval (CI)=66.4%-100%]. The median time-to-progression was 19 months (Figures 1). No patient treated with this regimen had locoregional failure as a first event (i.e. progression in the prostate or pelvic nodes). Distant metastases occurred in two patients. No patient presented with late toxicity of any grade.
Discussion
A phase I study was designed to evaluate the feasibility of the association of metronomic chemotherapy with standard doses of RT. The study demonstrated the feasibility of this association. Indeed the acute tolerance to RT was not impaired by concurrent metronomic chemotherapy, since no patient showed acute toxicity of a grade higher than 2.
To the best of our knowledge, this is the first report on the use of this combination. It is also the first report on the use of concurrent chemoradiation in prostate cancer refractory to hormonal therapy.
Acute toxicity according to the Common Toxicity Criteria (CTC) (15).
Acute toxicity versus dose level
From the point of view of the response rate (100%) and PFS (median=19 months), the results seem to be encouraging. The ORR, in particular, appears higher than the one recorded with metronomic chemotherapy-alone (22/32 patients, 69%) (10). This difference, however, could be due to patient selection since in this study, only patients without distant metastases were enrolled.
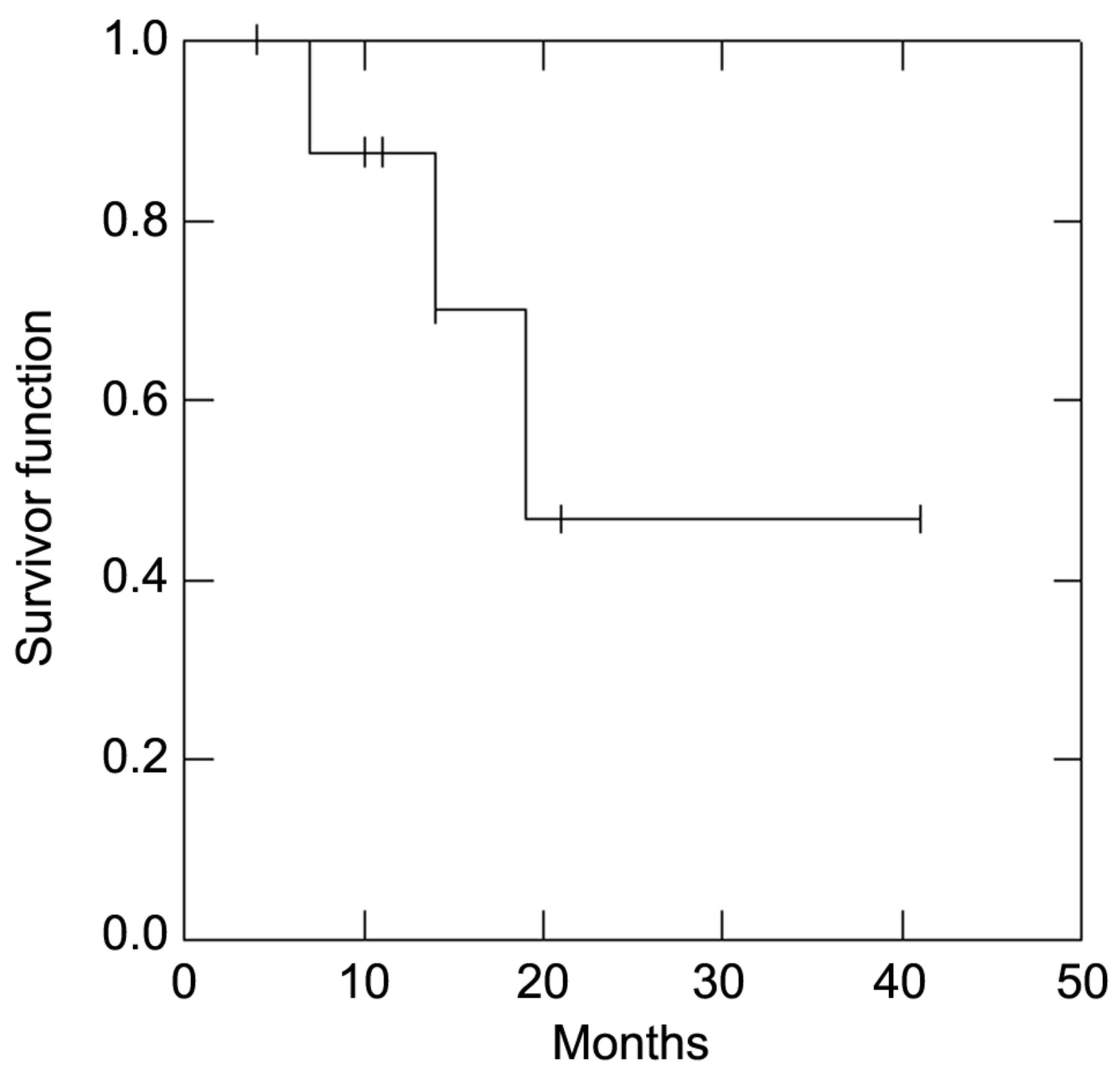
Kaplan-Meier survival estimate for the time to prostate-specific antigen progression.
At our center, a phase II study has been started to specifically evaluate the response and long-term control of disease. The study will also evaluate late toxicity associated with this therapeutic integration.
As previously mentioned, several studies have shown improved results by combining RT with neoadjuvant or adjuvant hormonal therapy. In particular, the use of AST in combination with RT improved patient outcomes in randomized trials (2, 3). However, AST is associated with side-effects such as fatigue, sexual impotence, hot flushes, anemia, anxiety, depression and osteoporosis, all of which have a negative impact on quality of life (1). Metronomic chemotherapy on the contrary is characterized by low toxicity. Therefore, based on the results of this study and on these theoretical assumptions, the role of metronomic chemotherapy could be evaluated as an alternative to hormone therapy in adjuvant treatment of patients with intermediate to high-risk disease. In addition, the use of this type of chemotherapy is characterized by low economic costs. Thus, this kind of integration may be useful to reduce the economic impact of adjuvant hormonal therapy.
Moreover new methods of metronomic chemotherapy based on different drug combinations may be tested in association with RT. Some of such attempts, for example, have shown high pre-clinical activity with the administration of metronomic CTX plus drugs targeting angiogenesis (20). Celecoxib, a cyclooxygenase-2 inhibitor, has both anti-angiogenic properties and anti-tumor activity. Phase II clinical trials using celecoxib in patients with a PSA recurrence (after radical prostatectomy and/or RT for their localized disease) have shown interesting activity, in terms of slowing PSA kinetics without relevant toxicities (21, 22).
Finally, in patients with very high-risk prostate carcinoma, a tri-modal therapy based on the combination of radiotherapy, AST and metronomic chemotherapy could be tested in order to improve the results of radio-hormono therapy.
Acknowledgements
We sincerely thank Ms. Milly Buwenge for reviewing and editing the manuscript.
- Received July 16, 2013.
- Revision received August 8, 2013.
- Accepted August 9, 2013.
- Copyright© 2013 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}