


Abstract
Aim: To evaluate survival outcomes of patients in pStage II-III rectal cancer treated with adjuvant 5-fluorouracil-based radiochemotherapy and toretrospectively analyzethe impact of prognostic variables on local control, metastasis-free survival and cause-specific survival. Patients and Methods: A total of 1,338 patients, treated between 1985-2005 for locally advanced rectal cancer, who underwent surgery and postoperative 5-fluorouracil-based chemoradiation, were selected. Results: The actuarial 5- and 10-year outcomes were: local control 87.0%-84.1%, disease-free survival 61.6%-52.1%, metastasis-free survival 72.0%-67.2%, cause-specific survival 70.4%-57.5%, and overall survival 63.8%-53.4%. Better outcomes were observed in patients with IIA, IIIA stage. Multivariate analyses showed that variables significantly affecting metastasis-free survival were pT4 and pN2, while for cancer-specific survival those variables were age >65 years, pT4, pN1, pN2, distal tumors and number of lymph nodes removed ≤12. Conclusion: This study confirmed that among stage II-III rectal cancer patients there are subgroups of patients with different clinical outcomes.
Colorectal cancer is the fourth and third more common tumor in Italy for males and females, respectively, with cancer mortality rates cumulative for both sexes of 40-50%. Between 1998 and 2002 rectal cancer was seventh in new neoplasms at diagnosis representing 8% of all cancer deaths cumulative for both sexes (1).
In the 1990s and 1980s, a series of randomized trials evaluating for postoperative, adjuvant, radiochemotherapy for locally advanced rectal cancer (AJCC sixth edition stage group II-III) (2) demonstrated a benefit in terms of local control (LC), disease-free survival (DFS), cause-specific survival (CSS) compared to surgery-alone or surgery followed by adjuvant chemotherapy or radiotherapy-alone (3-12).
Among potential benefits of adjuvant treatment combined is the possibility to select patients based on histopathological staging of disease and operative findings, while the main disadvantage is worse acute toxicity, ranging between 40-60% overall. The long-term high-grade toxicity of postoperative radiochemotherapy appears to be limited, ranging between 2 and 9%, including small bowel ileus and fibrosis (3-13).
Historical studies highlighted that the standard adjuvant combined treatment is 5-fluorouracil (5-FU)-based chemotherapy with a radiation pelvic dose ≥45 Gy (8-14). In 1990, a US (NIH) Consensus Conference recommended postoperative radiochemotherapy with concurrent 5-FU given as a protracted infusion as a standard treatment for rectal cancer in p-Stages II and III (15).
The most important factors influencing local recurrence, DFS and CSS are: pathological stage, surgical procedure (R0-R1-R2, margin status, adequate lymphadenectomy), tumor grade, lymphatic and vascular invasion, tumor site (low, medium, high rectum or recto/sigmoid junction), age, local recurrence/survival ratio and sex (14, 16-33).
Two pooled analyses conducted on randomized studies confirmed the different prognostic impact of pathological stages II and III because of heterogeneity of their pT and pN subgroups. These data were further confirmed by final results of a population-based surveillance study (SEER) (34-36). Although a randomised German trial (CAO/AIO/ARO-94) showed a benefit in LC, acute and late toxicity and sphincter saving rate for preoperative chemoradiation over postoperative chemoradiation (37), and guidelines endorsed by the Oncology Society with two consecutive European consensus conferences recommended the preoperative approach (38-39), postoperative chemoradiation is still performed for locally advanced rectal cancer in clinical practice.
A pooled analysis was carried out by the Gastrointestinal (G.I.) Working Group of the Italian Association of Radiation Oncology (AIRO) with the aim of reporting the outcome on 1,338 patients with pStage II-III rectal cancer treated with adjuvant 5-FU-based radiochemotherapy out of a total of 5,844 patients observed, analyzing the impact of several variables on LC, metastasis-free survival (MFS), CSS and reporting data of acute and late toxicities.
Patients and Methods
The reviewed cases were patients treated between 1985-2005 for locally advanced rectal cancer. Centers which participated on a voluntary basis in the study were asked to indicate how many patients were treated postoperatively among the total number of patients observed in the time period considered. Moreover, the Centers were asked to provide a path of minimal data with the goal of establishing a benchmark activity in Italy.
All patients underwent extirpative surgery followed by postoperative 5-FU-based chemoradiation without additional cytotoxic drugs in the therapy schedule.
The collected data were coded as to gender, age at surgery (≤65 years vs. >65 years), tumor location (low rectum, mid rectum or upper rectum or recto/sigmoid junction), pathological stage (II vs. III), T-stage (T1-T2, T3 or T4), N-stage (N0, N1 or N2), number of removed lymph nodes (≤12 vs. >12), margin status (negative, positive, missing), grading (G1-G2 or G3), histology and surgery rectal anterior resection (RAR) vs. abdomino-perineal resection (APR) or Hartmann procedure.
Tumor site was defined as low for tumors located within 5 cm of the anal verge, as mid rectum for tumors located at a distance of between 6 and 10 cm, and as upper rectum or rectosigmoid junction for tumors >10 cm to 15 cm by rigid proctoscopy or pathology report.
Acute and late toxicity were graded as per the Radiation Therapy Oncology Group (RTOG) criteria (40).
Local recurrence was defined as pelvic relapse after surgery and was histologically or radiologically proven. The follow-up evaluation started at the surgery date.
Statistical analysis. The evaluated variables were analyzed as follow: all qualitative factors were summarized as frequency and percentage, and all quantitative factors as mean and standard deviation or median and range, where appropriate. The Kaplan Meier method was used to calculate the 60-month rates of DFS and CSS. Time to LC and MFS was estimated using the method of cumulative incidence.
The follow-up was defined as the time interval between surgery and death due to disease or, for the other curves (LC, DFS and MFS), as the time between surgery and the first verified event. In patients in which none of the events occurred, the observational time interval was defined as the period from surgery to the last follow-up visit. The Kaplan-Meier method was used to also estimate DFS, MFS and CSS at 60 months and 120 months of follow-up, after stratifying patients for T stage, N stage, pStage and all other factors. Statistical significance between curves was evaluated using the log-rank test. Multivariate analyses were performed using the Cox proportional hazards model by backward elimination to determine independent prognostic factors with significant impact on LC, MFS and CSS. Covariates included in the Cox model were: age, gender, T and N stage, margin status, grading, tumor location, surgery and number of removed lymph nodes. Calculating the exponential of the regression coefficients from the Cox model provided an estimate of the hazard ratio (HR) and the 95% confidence interval (95% CI) (41). A p-value of 0.05 or less was considered statistically significant. All statistical analyses were performed using SPSS® software 11.0 (SPSS Inc., Chicago, IL, USA).
Results
The study closed in March 2008. Contributions from the fourteen participating centers are presented in Table I for a total number of 1,338 recruited patients out of a total of 5,844 patients observed in the same selected time period. Out of 5,844 cases of colorectal cancer, 1,581 were excluded due to lack of minimal data needed for their evaluation in this study, 2,925 were excluded for having received preoperative radiotherapy or no radiotherapy, leaving 1,338 evaluable cases.
Characteristics of patients and treatment features are shown in Table II.
The AJCC sixth edition pathological stage was II for 496 patients (37.1%) and III for 842 patients (62.9%).
All patients received adjuvant postoperative pelvic irradiation with concurrent and systemic 5FU-based chemotherapy schedules. The most frequently used adjuvant therapy schedule consisted of six chemotherapy courses with concomitant radiation therapy during the third and fourth course. The median total radiotherapy dose was 48 Gy (range=28-60 Gy) (1.8-2.0 Gy/day for five days a week), with a median time interval of 14 weeks between surgery and initiation of radiotherapy. Patients were treated by standard 2- to 4-field techniques. The median patient age was 63 years (range=27-86 years): 750 patients (56.1%) were aged ≤65 years and 588 (43.9%) were >65 years. The median follow-up was 56 months (range 6-203 months).
Out of 448 disease recurrences, 96 were local failure (LF) alone and 294 were distant metastases (DM) alone. A total of 427 patients had died of disease.
The actuarial 5-year outcomes were LC 87.0%, DFS 61.6%, MFS 72.0%, CSS 70.4% and OS 63.8%, respectively. At 10 years, the actuarial LC, DFS, MFS, CSS and OS were 84.1%, 52.1%, 67.2%, 57.5% and 53.4%, respectively (Figure 1).
Overall, 71/427 patients (16.6%) died with local recurrence alone, while 220/427 patients (51.5%) died with metastasis alone; 54/427 patients (12.6%) died with both local recurrence and metastasis.
Factors affecting LC, MFS and CSF prognosis (Figure 1): Univariate analysis. On univariate analysis (Table III), significant adverse factors for LC were T3 (p-value=0.020) and T4 (p=0.001), N2 disease (p-value =0.014), and high histological grade (G3) (p-value=0.001).
Accrual of 1,338 patients by radiotherapy center.
Adverse factors for MFS were male gender, age >65 years (p=0.027), T4 (p=0.018), N2 disease (p<0.001), high histological grade (G3) (p=0.012), low rectum tumor location and APR.
CSS was significantly affected by male gender, age >65 years (p<0.001), pStage III (p<0.001), T4 (p<0.001), N1 and N2 disease (p=0.020 and p<0.001), number of removed nodes ≤12 (p=0.031), high histological grade (G3) (p<0.001), low rectum tumor location and APR resection (Table III).
In particular, pStages IIIC (T2-4 N2), IIIB (T4 N1), IIB (T4 N0) and IIA (T3 N0), had worse results for LC and MFS than did pStage IIIA (T1-2 N1), while pStages IIIB (T3 N1) and IIB (T4 N0) had similar LC and MFS results. Surgical margin status was not a significant adverse factor for any outcome. In Figure 2, we present LC, MFS and CSS by stage grouping.
Factors affecting LC, DFS and overall Survival (OS) (Figure 1): Multivariate analysis. Multivariate analysis was conducted applying a Cox proportional hazard model by backward elimination. The variables inserted in the model were: gender, age, tumor location, pT, pN, number of removed lymph nodes, surgery and histological grade. For LC outcome, no variable had a statistically significant impact in multivariate analysis.
The strongly statistically significant unfavorable variables on MFS rates were pT4 tumors (HR=3.25, 95% CI=1.03-5.98; p=0.047), and pN2 nodal status (HR=2.69, 95% CI=1.76-4.11; p<0.001).
For CSS rates, a negative impact was recorded for age >65 years (HR=1.37,95% CI=1.02-1.85; p=0.037), pT4 tumors (HR=3.42, 95% CI=1.52-7.68; p=0.003), p N1 (HR=1.96, 95% CI=1.35-2.84; p<0.001), pN2 (HR=2.61, 95% CI=1.77-3.85; p<0.001), low rectum tumor location and number of lymph nodes removed ≤12 (Table IV).
Toxicity results. Because of the retrospective nature of this study, it was possible to correlate acute and late toxicity data with the radiation therapy technique only for a small group of patients (n° 424). Acute and late toxicity were assessed using RTOG scale (40). No fatal event was observed. The incidence of acute grade 3 or 4 toxicity was 15% for GI, 7% for GU and 3% for cutaneous effects. Twenty-seven patients (3.5%) experienced grade 3 late toxicity: GI effects in 19 patients, GU effects in six patients and skin effects in two patients. Forty-two patients (5.2%) experienced grade 4 late toxicity in terms of intestinal obstruction: these complications were successfully managed surgically.
Demographic, histological and treatment characteristics of patients.
The acute and late GI and GU toxicity occurred particularly in patients submitted to opposed anteroposterior (AP/PA) radiation technique (77 patients): grade 3-4 GI and GU acute toxicity occurred in 53% (41 patients) and 27% (21 patients), respectively, while grade 3-4 GI and GU late toxicity occurred in 23% (18 patients) and 10% (8 patients) respectively. Twenty-seven patients (35%) in the subgroup of those treated with an AP/PA technique experienced grade 4 GI late toxicity in terms of bowel obstruction surgically-managed
With regard to chemotherapy schedules, timing of drugs administration in term of acute and late toxicity in the same subgroup of patients (424).

Kaplan-Meier curves of local control, disease-free survival, metastases-free survival and cause-specific survival.
Univariate analysis of prognostic variables in term of 60-month cause-specific survival, metastasis-free survival and local control in 1,338 patients.
Discussion
The randomised German trial (CAO/AIO/ARO-94) (37), two consecutive European consensus conferences (38, 39) and a preoperative radiochemotherapy approach for locally advanced rectal cancer is recommended. However, postoperative chemoradiation is still performed in clinical practice in Italy, especially in the rural areas where the risk of preoperative under-staging, the waiting lists for radiotherapy centers and the lack of respect for the current recommended guidelines are the main reasons for the prescription of a postoperative treatment.
In this pooled analysis on 1,338 patients with locally advanced rectal cancer treated with adjuvant 5-FU-based radiochemotherapy, we retrospectively evaluated the outcome in terms of DFS, LC, MFS and CSS and analyzed the impact of several variables on LC, MFS and CSS.
The historical combined randomized postoperative 5-FU-based radiochemotherapy trials demonstrated an improvement of LC rate ranging between 83%-92% with a mean survival rate of 60% (53%-71%) (3-5, 9-14).
Two baseline pooled analyses (34, 35) and a recent SEER population-based rectal cancer analysis (36) evaluated the impact of different subgroups of AJCC (sixth edition) staging on clinical outcome. Gunderson and co-workers, in their pooled-analysis of 3,791 patients, analyzed the influence of T-N variables and pathological stage on LC, DFS and OS, showing that OS and DFS were dependent on both the T and N categories (34).
Multivariate analysis of factors having an influence on cause specific survival and metastases free survival as identified by Cox's proportional hazard model. The items in brackets are the referent (hazard risk equal to 1).
Five-year OS for stages IIA (T3 N0) and IIIA (T1-2 N1) ranged from 75%-79%, while 5-year DFS ranged from 65%-73%; the one for stages IIB (T4 N0), IIIB (T3 N1) and IIIC (T1-2 N2) ranged from 60%-67% with 5-year DFS of 48%-58%; the one for stages IIIB (T4 N1), IIIC (T3 N2) and IIIC (T4 N2) ranged from 37%-44% with 5-year DFS of 30%-36%.
Therefore, in terms of OS and DFS, pStage II (T3-4 N0) and pStage IIIA (T1-2 N1) were better than pStage IIIB (T3N1) and pStage IIIC (T3-4 N2), while 5-year LC is less affected by different subgroups of stages, ranging between 77% and 93% overall.
Based on these results, an intermediate-risk group (T3 N0; T1-2 N1), a moderately-high risk group (T4 N0, T1-2 N2, T3 N1) and high-risk group (T3 N2, T4 N1, T4 N2) were described and the authors concluded that different treatment strategies may be indicated for these different risk groups of patients.
Greene and co-workers analyzed the survival outcome from data of a National Cancer Data Base for 5,987 patients with stage III rectal cancer between 1991 and 1993. Survival was calculated using three subgroups (IIIA: T1-2, N1; IIIB: T3-4, N1; IIIC: any T, N2). Stage IIIA patients had an observed 60% 5-year survival, IIIB patients 41% and IIIC patients 29%, with significant differences (p<0.0001) in all stages (35). The authors affirmed that recommendations for sub-classifying patients with traditional stage III rectal cancer into three prognostic groups should be universally applied in decision-making of clinical practice.
In the SEER rectal cancer analysis from 1992 to 2004, Gunderson and co-workers compared the survival outcome of 35,829 patients of the SEER database (36) with 3,791 patients of a previous pooled analysis (34). Five-year OS for stages IIA (T3 N0) and IIIA (T1-2 N1) ranged from 78% to 85%; for stages IIB (T4 N0), IIIB (T3 N1) and IIIC (T1-2 N2) from 53.6% to 66.9%, and for stages IIIB (T4 N1), IIIC (T3 N2) and IIIC (T4 N2) from 22.1% to 49.9%. The data in the SEER population-based rectal cancer analysis confirmed the pooled analyses results with regard to the more favourable prognosis of patients with T1-2 N1-2 lesions (IIIA and IIIC stages, AJCC sixth ed.) and less favorable prognosis of patients with T4 N1 cancer (stage IIIB, AJCC sixth edn.), T3 N2 and T4 N2 (stage IIIC AJCC sixth edn.).
Both SEER and rectal pooled analyses data support the shift of T1-T2 N2 lesions from IIIC to IIIA or IIIB and T4 N1 tumors from IIIB to IIIC.
SEER rectal cancer outcomes also supported sub-dividing T4 (T4a vs. T4b), N1 (N1a vs. N1b) and N2 (N2a vs. N2b) categories of disease, showing different prognosis based on the different presentations of penetration depth of the tumor and number of lymph nodes involved, respectively.
Our retrospective pooled analysis of 1,338 patients from 1985 to 2005 showed that LC, DFS, and CSS were 87.0%, 61.6%, and 70.4% respectively at 5 years and 84.1%, 52.1% and 57.5% at 10 years, and interesting differences were observed in terms of outcomes (LC, MFS and CSS) for TNM subgroups. Five-year CSS for stages IIA (T3 N0) and IIIA (T1-2 N1) was 79.8% and 80.4% respectively, while 5-year MFS was 81.9% and 84.5% respectively; for stages IIB (T4 N0) and IIIB (T3-4 N1) were 77.8% and 70.3%, respectively with 5-year MFS of 72.6% and 72.9%, respectively; and that for stage IIIC (T1-4 N2) was 55.2%, with 5-year MFS of 54.5%.
Moreover, the analysis confirmed LC is less affected by different subgroups of stages ranging between 80% and 98% overall, with unfavorable prognostic impact of T3, T4 tumors, N2 and G3 at univariate analysis.
Although with the limitations of a retrospective analysis, a small cohort of patients and of a non-certified quality of surgery, our results seem to confirm a high-risk for patients with pStage III C (T3/T4 N2 rather T1/T2 N2) and pStage IIIB (T4 N1) disease, moderately high-risk for pStage III B (T3 N1) and intermediate risk for pStage II (T3 better than T4 N0) and pStage III A (T1-2 N1).
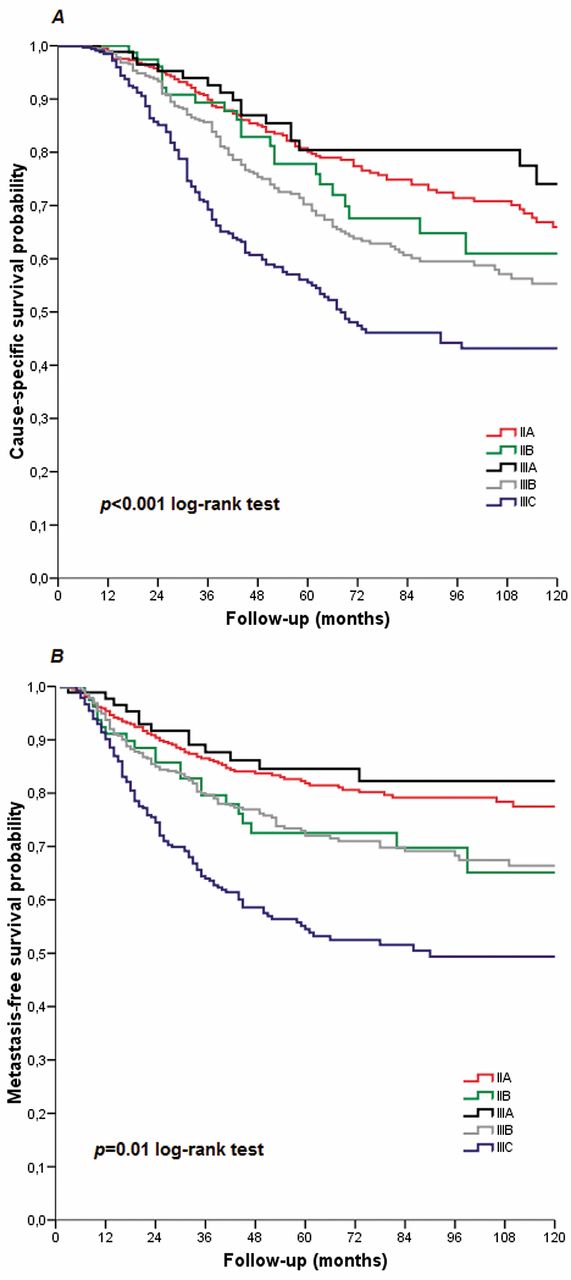
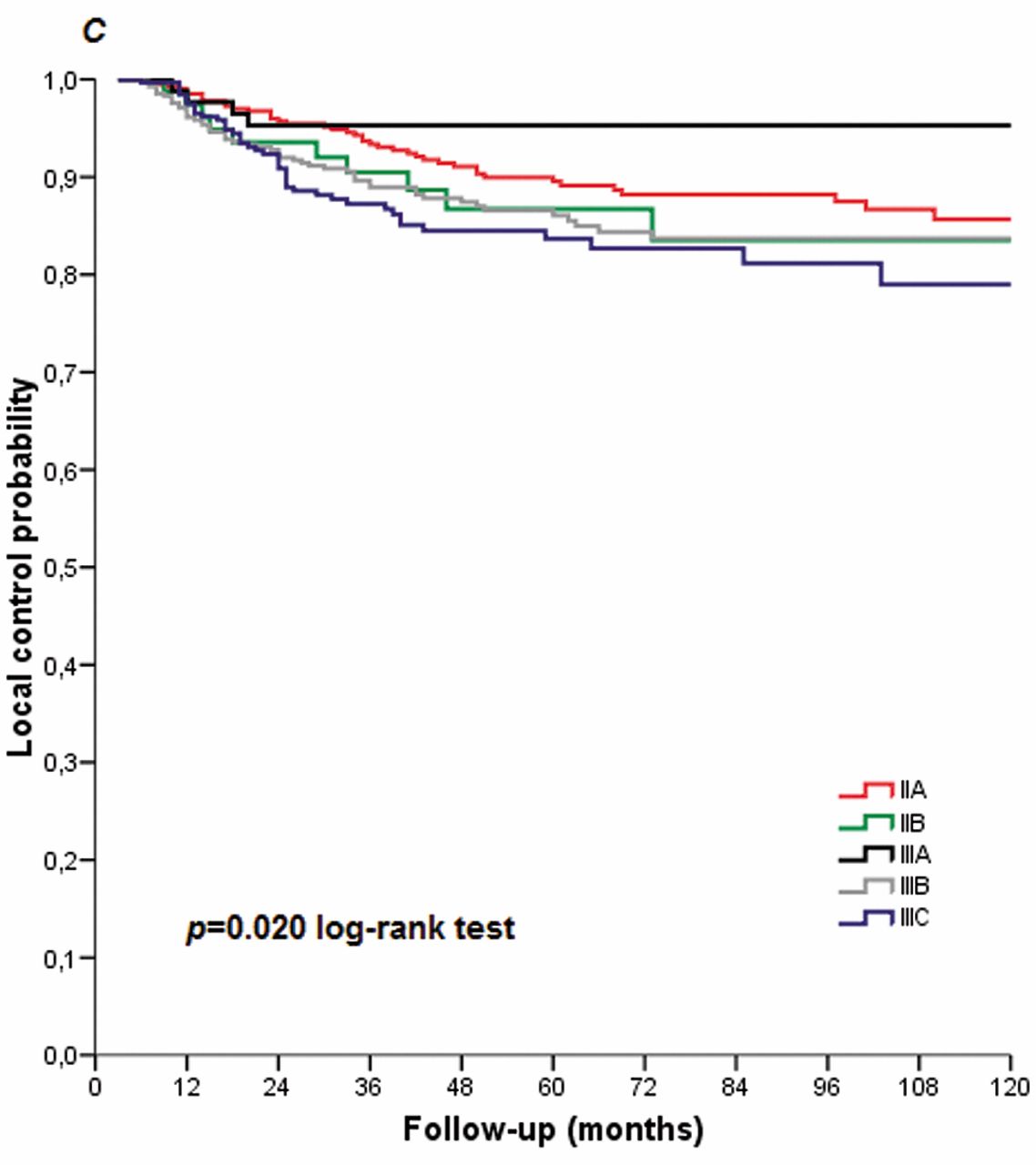
Impact of pStage on cause-specific survival (A), metastases-free survival (B) and local control (C).
Regarding other risk factors considered at univariate analysis, prognostic factors unfavorably influencing MFS were male gender, age >65 years, individual pT4 - pN2 variables, APR resection, G3 tumors and low tumor location.
Negative prognostic factors for CSS were male gender, age >65 years, pT4, pN1 and pN2 variables, number of removed nodes ≤12, APR resection, G3 tumors and low tumor location.
At multivariate analysis, age >65 years, p T4, p N1-2, low tumor location and number of removed lymph nodes ≤12 had a negative impact on CSS, while pT4 and pN2 variables had a negative impact on MFS.
Regarding nodal status, the prognostic role of nodal stage has been documented in several studies. Martenson and co-workers in their univariate analysis of Intergroup Protocol 0130 showed that the presence of positive nodes (>3) was the only factor influencing DFS and OS (42). Other studies evidenced the importance of the number of nodes removed (≥12) and the negative prognostic impact on clinical outcomes of the number of positive nodes removed (≥ 3) (16, 22, 27, 31, 42).
In our study, the mean number of nodes removed was 14 (range 0-65) and we showed a detrimental prognostic influence of removal of 12 or fewer on CSS at the multivariate analysis.
Factors such as tumor grade have been shown to influence survival, LC and metastasis rate (16,19,22) and G3 tumors were statistically significant negative factors in LC, MFS and CSS at our univariate analysis.
Regarding the prognostic role of age, the results are conflicting. Jatzko and co-workers found that age was not a significant factor at univariate analysis but it became significant at multivariate analysis because age ≥65 years influenced DFS (25). Myerson and co-workers did not find any influence of age on LC and DFS (19). Our study showed an impact of age (> 65 years) on MFS and CSS for both univariate and multivariate analysis, and a negative impact on CSS only for multivariate analysis.
Other variables have been considered as factors influencing LC, metastasis rate, DFS and CSS, such as lymphatic vascular invasion (43), negative surgical margins (16), tumor fixation at surgery, and gender (33).
We did not find statistical significance for surgical margins due to the few number of patients with positive and unknown margins (51 positive and 319 unknown, respectively).
With regard to tumor location, Benzoni and co-workers examined the clinical outcomes in patients which had been enrolled in a protocol of neoadjuvant chemoradiation followed by surgery for rectal cancer, distinguishing between intraperitoneal and extraperitoneal cancer (45). They diagnosed all local recurrences (13.8%) and all metastases (liver: 15.5%; lung: 10.3%; others: 8.6%) in extraperitoneal cancer and only one case of lung metastasis arose from intraperitoneal cancer. The DFS and OS were worse for extraperitoneal versus intraperitoneal rectal cancer (p=0.006 for both outcomes).
In our study we found a negative influence of extraperitoneal tumor location on MFS at univariate analysis and on CSS at multivariate analysis. This could not be merely explained by an incomplete lymphatic resection or inappropriate application of chemoradiation protocols. Extraperitoneal tumors, perhaps, could be more aggressive than intraperitoneal ones, spreading more precociously or have less sensitivity to adjuvant chemoradiation because of their localization, rather than differences in biological characteristics.
In this retrospective experience, an evaluation of the toxicity was also performed. Because of the retrospective nature of this study, it was possible to correlate acute and late toxicity data with the radiation therapy technique for only a small group of patients (424). Moreover, even if the toxicity data are quite selective, the observed results can still provide information on toxicity after postoperative radiotherapy and may support similar results from other studies (4-7, 9-10).
Acute GI and cutaneous toxicity RTOG grade 3 or more correlated with the findings from other series (4-7, 9-10), while we observed low rates of acute GU and hematological toxicity RTOG grade 3 or more. The late toxicity was very low and it was similar to the findings of historical studies (4-7, 9-10).
Comparing the toxicities reported with the radiotherapy technique, we recorded higher rates of toxicities in patients submitted to opposed AP radiation techniques, while no significant differences were noted for different doses and timing of drugs administration in term of acute and late toxicity in the same subgroup of patients.
Conclusion
For many years, the older editions of TNM staging represented the only powerful prognostic factor in treatment decisions in the adjuvant combined therapy for locally advanced rectal tumors with significant limitations related to the different prognoses for patients within the same stage (II-III) and a negative impact for the survival outcome, as shown by the main baseline studies such as the Pooled (34, 35) and SEER analyses (36). The seventh edition of the TNM classification (46), although with several limitations regarding the nodal status leading use the sixth edition still being used, took care of reviewing the stages and sub-stages also taking into account non-anatomical prognostic factors. Although with the limitations of a retrospective analysis, a small cohort of patients and a non-certified quality of surgery, our results seem to confirm a different prognostic trend within II-III substage of disease and provide a platform for further ongoing evaluations. In particular, the ongoing sharing of large databases allow for better analysis of the clinicopathological features and their prognostic impact through the development of models (47) that could promote tailored treatments for improving survival in rectal cancer.
- Received July 22, 2013.
- Revision received September 16, 2013.
- Accepted September 17, 2013.
- Copyright© 2013 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.