


Abstract
Background: Although p21 is an important component that regulates cell-cycle progression, no consensus has been reached about its clinicopathological significance in esophageal squamous cell carcinoma (ESCC). In the present study, we investigated its prognostic significance and correlation with cyclin-D1 (CCND1) expression in ESCC. Materials and Methods: The p21 labeling index (LI) was calculated by immunohistochemistry for 69 primary tumor samples obtained from patients with ESCC who had undergone curative esophagectomy, and correlations between p21 LI and various clinicopathological features, prognosis, and CCND1 LI were studied. Results: The p21 LI of these tumors ranged from 2.0% to 57.0% (median=28.4%, mean±SD=27.3%±13.0). p21 LI was positively correlated with CCND1 LI. When patients were divided into two groups using a p21 LI cut-off value of 30%, the 5-year survival rate of patients with p21 LI of ≥30% was 80.0%, which was significantly higher than that of patients with p21 LI of <30% (55.5%). Furthermore, when patients were divided into four groups according to p21 and CCND1 expression, the 5-year survival rate of patients with p21 LI of <30% and CCND1 LI of ≥45% was the lowest (44.4%). Multivariate analysis demonstrated that venous invasion, lymphatic invasion, and p21 LI were independent prognostic factors. Conclusion: Our results indicate that p21 LI is correlated with CCND1 LI and can be used as an independent prognostic factor for patients with ESCC following selection of a suitable cut-off value.
Esophageal carcinoma is an aggressive type of cancer constituting a major cause of cancer-related deaths worldwide (1, 2). However, although recent advances in surgical techniques and perioperative management strategies have improved the outcome of esophageal squamous cell carcinoma (ESCC) (3, 4), patients with advanced disease still frequently develop recurrence, and prognosis of these patients remains poor (5-7). To predict the treatment outcomes of patients with ESCC, it is important to understand the proliferative activity of ESCC tumor cells and its prognostic impact. Various molecular biological markers, such as cell cycle-related molecules, have recently been studied in patients with ESCC; however, predicting the risk of cancer progression and disease outcomes by these molecules remains uncertain.
p21 is a cyclin-dependent kinase (CDK) inhibitor that directly inhibits the activity of the cyclin-D1 (CCND1)/CDK4 complex. The active CCND1/CDK4 complex targets the retinoblastoma protein for phosphorylation, which allows for the release of E2F transcription factors that activate G1/S phase gene expression (8). Several studies have assessed the proliferative activity of ESCC using p21 expression (9-13). However, no consensus has been reached about the relationship between p21 and clinicopathological parameters. In addition, some reports have indicated that a high p21 labeling index (LI) was significantly correlated with good prognosis (9, 10), while others found that it was correlated with poor prognosis (11-13). Various p21 LI cut-off values were used in these studies. Thus, because the clinicopathological impact of p21 LI in ESCC is still disputed, further studies to verify its importance are necessary. In addition, to our knowledge, no reports have investigated the correlation between p21 and CCND1 in human ESCC samples by immunohistochemistry.
The objective of the present study was to analyze the p21 LI of human ESCC samples from our Institute, determine the relationships between p21 LI and various clinicopathological parameters, and calculate a suitable p21 LI cut-off value for predicting patient prognosis. Furthermore, as far as we are aware, this is the first report to show correlation between p21 LI and CCND1 LI in human ESCC samples using immunohistochemistry and to investigate the clinical significance of their mutual relationships.
Materials and Methods
Patients and primary tissue samples. ESCC tumor samples were obtained from 69 patients with histologically proven primary ESCC who underwent esophagectomy (potentially curative R0 resection) at the Kyoto Prefectural University of Medicine (Kyoto, Japan) between 1998 and 2007, and analyzed retrospectively. These samples were embedded in paraffin after 24 h of formalin fixation. Patient eligibility criteria were not having developed synchronous tumors or multiple metachronous tumors and not having received preoperative chemotherapy or radiation therapy. We excluded patients with non-curatively resected tumors or non-consecutive data. All patients gave their written informed consent for inclusion in this study. Relevant clinicopathological and survival data were obtained from the hospital database. Staging was principally based on the seventh TNM staging system (14).
Immunohistochemistry. Paraffin sections (3-μm thick) of tumor tissue were subjected to immunohistochemical staining for p21 and CCND1 using the avidin-biotin-peroxidase method. Briefly, paraffin sections were de-waxed in xylene and hydrated through a graded series of alcohols. Antigen retrieval was performed by heating the samples in Dako REAL Target Retrieval Solution (Glostrup, Denmark) for 40 min at 95°C. Endogenous peroxidase activity was quenched by incubating the sections for 30 min in 0.3% H2O2. Sections were incubated for one hour at room temperature with the following antibodies: p21 antibody (Cell Signaling Technology, Beverly, MA, USA) and CCND1 antibody (Abcam, Cambridge, UK). The avidin-biotin-peroxidase complex system (Vectastain ABC Elite kit; Vector Laboratories, Burlingame, CA, USA) was used for color development with diaminobenzidine tetrahydrochloride. Sections were counterstained with hematoxylin. These sections were then dehydrated through a graded series of alcohols, cleared in xylene, and mounted. Control sections of known positive ESCC were included in each antibody run, and negative control sections were produced by omitting the primary antibody.
Determining proliferative activity by immunohistochemistry was performed quantitatively by counting immunoreactive tumor cells. Only distinct immunoreactive tumor cell nuclei were counted. p21- and CCND1-labeled cells were quantified in five selected fields of the highest proliferative activity at ×400 magnification. The LI of each case was calculated as the number of positive cells divided by the total number of examined cells in all the examined fields.
Statistical analysis. Statistical analysis was carried out using the Student's t-test (for comparisons between two groups), Tukey-Kramer test (for multiple comparisons), or Fisher's exact test to investigate correlations between clinicopathological parameters and p21 LI. Survival curves were constructed using the Kaplan-Meier method, and differences in survival were examined using the log-rank test. Multivariate analysis of the factors influencing survival was performed using the Cox proportional hazard model. Differences were considered significant when the associated p-value was less than 0.05. All analyses were performed using statistical software (JMP, version 10; SAS Institute Inc., Cary, NC, USA). Correlation analyses were performed by creating Fit Y by X plots using JMP.
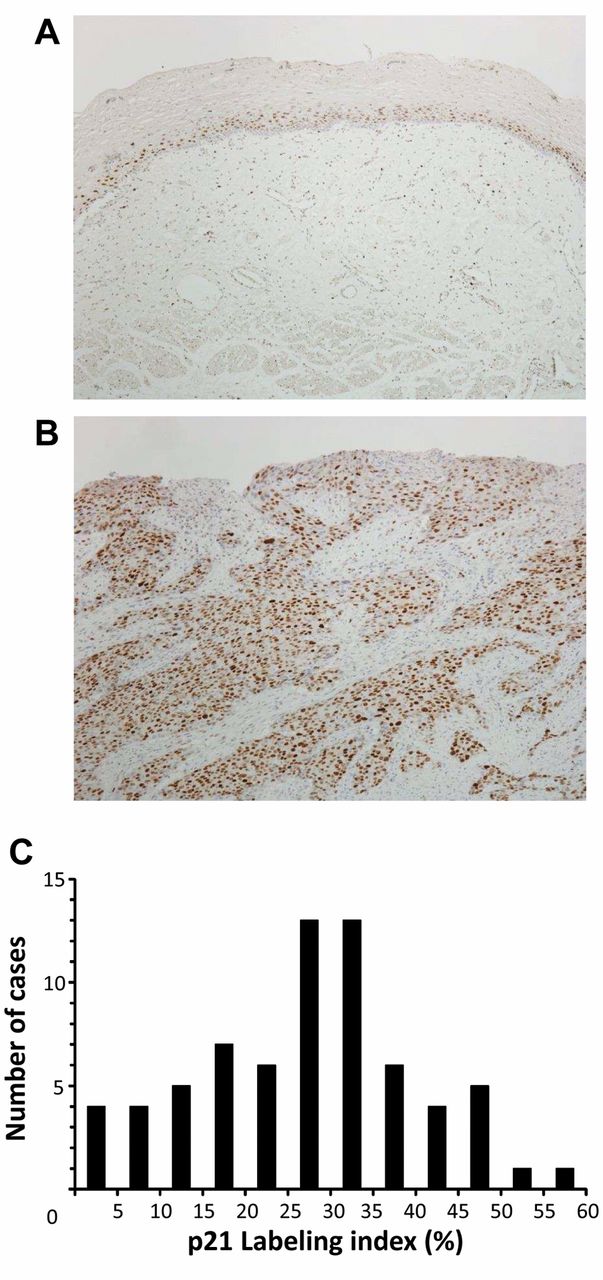
A: Immunohistochemical staining of non-cancerous esophageal epithelia with the p21 antibody. Magnification ×100. B: Immunohistochemical staining of primary human esophageal squamous cell carcinoma (ESCC) samples with the p21 antibody. Magnification, ×100. C: Histogram of the p21 labeling index in 69 human ESCC samples.
Results
An immunohistochemical investigation with the p21 antibody demonstrated p21 expression in the parabasal cell layer of normal esophageal mucosa (Figure 1A). p21-positive tumor cells were clearly identified by brown color nuclear staining (Figure 1B). The proportion of p21-positive tumor cells varied widely between the tumors (Figure 1C). The minimum p21 LI was 2.0%, and the maximum p21 LI was 57.0% (median=28.4%; mean±standard deviation (SD)=27.3%±13.0). Immunohistochemical analysis of CCND1 was performed to evaluate the association between p21 and CCND1 expression (Figure 2). An immunohistochemical investigation with the CCND1 antibody demonstrated that CCND1-positive tumor cells were clearly identified by brown color nuclear staining (Figure 2C and D). The proportion of CCND1-positive tumor cells varied widely between the tumors. The minimum CCND1 LI was 2.1%, and the maximum CCND1 LI was 82.8% (median=46.2%; mean±SD=43.3%±21.1). The data in the CCND1 histogram were similarly approximately normally distributed (data not shown). Although the staining patterns of p21 and CCND1 antibodies were different, as shown in Figure 2A-D, p21 LI was weakly positively correlated with CCND1 LI (R2=0.063, p=0.038) (Figure 2E).

Immunohistochemical staining of primary human esophageal squamous cell carcinoma (ESCC) samples with the p21 and cyclin-D1 (CCND1) antibodies. A,B: p21 antibody, magnification: ×100. C,D: CCND1 antibody, magnification: ×100. E: Correlation analysis of the relationship between p21 and CCND1 labeling indices was performed by producing Fit Y by X plots. The p21 labeling indices was positively correlated with the CCND1 labeling index (R2=0.063, p=0.038).
Associations between the clinicopathological features of esophageal cancer and p21 labeling index.
Correlations between p21 LI and various clinicopathological parameters were analyzed. Regarding CCND1 LI, we divided the ESCC patients into two groups using a CCND1 LI cut-off value of 45%, which was near the median, the CCND1 LI <45% (n=34) and CCND1 LI ≥45% (n=35) groups. No significant correlation was found between p21 LI and clinicopathological features, age, gender, pT categories, pN categories, pStage, histological type of ESCC, lymphatic invasion, venous invasion, and CCND1 LI (<45%/ ≥45%) (Table I). We then divided the patients into two groups using a p21 LI cut-off value of 30%, which was near the median, the p21 LI <30% (n=39) and p21 LI ≥30% (n=30) groups, and compared their clinicopathological features. No significant correlation was found between p21 LI and other clinicopathological features (Table II). Furthermore, we assessed which factors of the 10 studied variables (age, gender, pT, pN category, pStage, histological type, lymphatic invasion, venous invasion, p21 LI, and CCND1 LI) influenced survival after curative resection of esophageal cancer. In univariate analysis of survival after esophagectomy, pT, pN, pStage, lymphatic invasion, venous invasion, and p21 LI were found to be significant prognostic factors (p=0.003, 0.004, 0.007, 0.013, 0.020 and 0.040, respectively) (Table III). The 5-year survival rate of patients with a p21 LI of ≥30% was 80.0%, which was significantly higher than that of patients with a p21 LI of <30% (55.5%) (Table III, Figure 3A). On the other hand, the 5-year survival rate of patients with a CCND1 LI of ≥45% was 69.9%, which was not significantly different from that of patients with a CCND1 LI of <45% (60.7%) (Table III, Figure 3B). When patients were divided into four groups using a p21 LI cut-off value of 30% and CCND1 LI cut-off value of 45%, the 5-year survival rate of patients was stratified depending on the p21/CCND1 expression status, and the one of patients with a p21 LI of <30% and CCND1 LI of ≥45% was the lowest (44.4%) (Figure 3C). Multivariate analysis with variables whose p-value were less than 0.15 in univariate analysis demonstrated that lymphatic invasion, venous invasion, and p21 LI were independent prognostic factors (p=0.046, 0.036 and 0.049, respectively) (Table IV). These findings suggest that p21 LI is an independent prognostic factor for patients with ESCC.
Associations between the clinicopathological features of esophageal cancer and p21 labeling index (cut-off value=30%).
Discussion
The p21 protein, which is encoded by the p21WAF1/CIP1 gene, is regulated by wild-type p53 (15, 16). The p21 gene acts as a major regulator of the G1 checkpoint of the cell cycle by binding to and inhibiting the activities of most cyclin/CDK complexes (8). Although several studies have investigated the relationship between p21 expression and ESCC, the prognostic significance of p21 in ESCC is still controversial (9-13). Some reports showed that p21 could be considered as a positive prognostic predictor for patients with ESCC (9, 10). However, other reports showed that p21 was as an adverse prognostic predictor for such patients (11-13). Although several reports investigated the combined immunohistochemical expression of p53 and p21 proteins (10, 11), no studies have analyzed the correlation between p21 and CCND1 expression in ESCC. Therefore, in the present study, we sought to investigate expression of the p21 protein in ESCC specimens by immunohistochemistry, define the prognostic significance of p21 expression, and analyze the correlation between p21 and CCND1 in ESCC.
Aberrant expression of p21, detected by immunohistochemical staining, in which both decreases and increases in p21 expression were associated with poor prognosis, has been shown in ESCC (9-13). Liu et al. showed that p21 could serve as a positive prognostic predictor for patients with stage III ESCC (9). Natsugoe et al. showed that examination of p21-positive expression in the p53-dependent pathway helps to estimate the favorable prognosis of patients with advanced ESCC (10). However, several studies obtained contrasting results. The view that p21 acted as a tumor suppressor was complicated by p21 being overexpressed in various types of human cancers (17, 18). Taghavi et al. also showed that p21 overexpression was associated with poorer clinical outcomes in patients with ESCC (11). Goan et al. reported that p21 overexpression correlated with chromosomal instability and served as an adverse prognostic predictor for patients with ESCC (12). Sarbia et al. demonstrated a significant correlation between strong p21 expression and poor prognosis (13). In the present study, our results showed that the 5-year survival rate of patients with a p21 LI of ≥30% was significantly higher than that of patients with a p21 LI of <30%, and that a low p21 LI was an independent poor prognostic factor. These results clearly support the former reports.

Survival curve of patients after curative resection for esophageal squamous cell carcinoma (ESCC) according to the p21, and cyclin-D1 (CCND1) labeling indices (LI). A: Patients were classified into two groups: p21 LI <30% (n=39) and p21 LI ≥30% (n=30). B: Patients were classified into two groups: CCND1 LI <45% (n=34) and CCND1 LI ≥45% (n=35). C: Patients were classified into four groups: p21 LI <30%/CCND1 LI <45% (n=23), p21 LI ≥30%/CCND1 LI <45% (n=11), p21 LI <30%/CCND1 LI ≥45% (n=16), and p21 LI ≥30%/CCND1 LI ≥45% (n=19). *p<0.05: log-rank test.
Five-year survival rate of patients with esophageal cancer according to various clinicopathological parameters.
Several studies have demonstrated that CCND1 is an independent prognostic factor in esophageal cancer. The Research Committee on Malignancy of Esophageal Cancer, Japanese Society for Esophageal Diseases performed immunohistochemical analysis of CCND1 expression in 416 patients with ESCC and reported that increased expression was a significant prognostic factor (19). Fukuchi et al. showed that patients with high CCND1 expression had a significantly more favorable prognosis than patients with low CCND1 expression (20). In the present study, the 5-year survival rate of patients with a CCND1 LI of ≥45% was 69.9%, which was not significantly different from that of patients with a CCND1 LI of <45% (60.7%). However, when patients were analyzed according to p21 expression levels, the 5-year survival rate of patients with high CCND1 expression was slightly worse than those with low CCND1 expression (Figure 3C), which suggests that our results support the findings of previous reports in spite of the limitation of a small sample size. No reports have investigated the correlation between p21 and CCND1 expression in ESCC as far as we are aware of; therefore, our study indicates that analyzing the combined immunohistochemical expression of these proteins may be useful for predicting the outcomes of patients with ESCC.
Prognostic factors of esophageal cancer according to multivariate analysis.
In our study, no significant correlation was found between p21 expression and clinicopathological parameters in terms of age, gender, pT categories, pN categories, pStage, histological type of SCC, lymphatic invasion, and venous invasion. Although these results may not be persuasive because of the limitation of a small sample size, several studies on ESCC have also shown no significant correlation between p21 expression and different clinicopathological parameters among patients with ESCC (9-12). The p21 LI cut-off values used in previous reports ranged from 10% (10) to 50% (11, 13). In the present study, the median, mean±SD, and range of p21 LI in ESCC were 28.4%, 27.3%±13.0%, and 2.0%-57.0%, respectively. We used 30% as the cut-off value and found that p21 LI was an independent prognostic factor for ESCC. Although additional, more extensive prospective studies are needed to further clarify the possible prognostic significance of p21 LI for patients with esophageal cancer, the present study suggests a potential p21 LI cut-off value for patients with ESCC, and revealed that this cut-off value has prognostic significance.
In conclusion, the present study demonstrated that p21 LI was correlated with the CCND1 LI in patients with ESCC. Furthermore, we showed that p21 LI can be used as an independent prognostic factor for patients with ESCC by selecting a suitable cut-off value.
Acknowledgements
This work was supported by Grants-in-Aid for Young Scientists (B) (22791295, 23791557, 24791440) and a Grant-in-Aid for Scientific Research (C) (22591464, 24591957) from the Japan Society for the Promotion of Science.
Footnotes
-
↵* These Authors contributed equally to this study.
-
Conflicts of Interest
The Authors declare that they have no conflict of interests.
- Received July 26, 2013.
- Revision received September 11, 2013.
- Accepted September 13, 2013.
- Copyright© 2013 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.