


Abstract
Somatic mutations in PPP2R1A, which encodes a scaffolding subunit of serine/threonine protein phosphatase 2A (PP2A), have recently been described in different types of gynecological neoplasias. To extend this observation, we examined the frequency of PPP2R1A mutation in some major histological subtypes of type I and type II ovarian carcinoma. Mutational analysis of PPP2R1A (exons 5 and 6) was performed on 88 primary ovarian carcinomas, including mucinous, clear cell, high-grade serous, and high-grade endometrioid ovarian carcinoma. In addition, exons 9 and 20 of Phosphatidylinositol-4,5-bisphosphate 3-kinase (PIK3CA), exon 1 of v-Ki-ras2 Kirsten rat sarcoma viral oncogene homolog (KRAS), and exon 15 of v-raf murine sarcoma viral oncogene homolog B1 (BRAF) were sequenced and compared across the different histological subtypes. Finally, survival analysis was performed to determine any prognostic significance of these mutations. Mutations in PPP2R1A were rare: detected in 4.5% (1/22) of clear cell, 4.5% (1/22) of high-grade serous, and 6.7% (1/15) of high-grade endometrioid ovarian carcinoma. Interestingly, no PPP2R1A mutations were observed in mucinous ovarian carcinoma. A higher frequency of PIK3CA mutations (50%, 11/22) was found in clear cell carcinoma and a higher frequency of KRAS mutations (24.1%, 7/29) was observed in mucinous carcinoma. In addition, high-grade endometrioid ovarian carcinoma exhibited KRAS and PIK3CA mutations in 26.7% (4/15) and 20% (3/15) of cases, respectively. Survival analysis showed no significant association between mutational status and overall survival of patients. This study indicates that the PPP2R1A mutation occurs at a lower frequency compared to other gynecological malignancies, irrespective of the histological subtype.
Ovarian carcinoma is the most lethal gynecological malignancy (1), and its incidence has increased in the past decade. Depending on the epithelial component, ovarian carcinomas are histologically sub-classified into four major subtypes: serous, mucinous, endometrioid, and clear cell. They represent a heterogeneous group of cancers with distinct clinicopathological and molecular features (2).
To provide a conceptual framework for the study of the pathogenesis of ovarian cancer, a dualistic model was proposed that organizes the clinical, pathological, and molecular features of ovarian cancer by categorizing them into type I and type II tumors (3). Type I tumors include low-grade serous, low-grade endometrioid, clear cell, and mucinous carcinomas; these tumors develop in a stepwise fashion from well-established precursor lesions, such as borderline tumors and endometriosis. They typically present as large masses that are confined to one ovary, are indolent, and have a good prognosis. Type I tumors are relatively genetically-stable and typically display a variety of somatic mutations of v-Ki-ras2 Kirsten rat sarcoma viral oncogene homolog (KRAS), v-raf murine sarcoma viral oncogene homolog B1 (BRAF), phosphatase and tensin homolog (PTEN), Phosphatidylinositol-4,5-bisphosphate 3-kinase (PIK3CA), β catenin (CTNNB1) and the AT-rich interactive domain 1A (ARID1A), but very rarely of tumor protein p53 (TP53) (3-6). In contrast, type II tumors include high-grade serous carcinomas, high-grade endometrioid carcinoma, malignant mixed mesodermal tumors (carcinosarcomas), and undifferentiated carcinomas; these tumors are advanced at presentation in more than 75% of cases, they grow rapidly, and they are highly aggressive. Type II tumors, of which high-grade serous carcinoma is the prototypic type, are chromosomally highly unstable and harbor TP53 mutations in more than 95% of cases (7); in addition, they rarely display the mutations found in type I tumors.
Among the various histological subtypes of ovarian carcinoma, the mucinous tumors have been the least studied histological type, probably because of their relative rarity (2-10% of epithelial ovarian carcinomas) (8). However, these tumors have a poorer response to taxane- and platinum-based chemotherapy, resulting in poor survival outcomes compared with serous ovarian carcinomas (9). Therefore, understanding the mechanisms contributing to mucinous ovarian cancer development and progression, as well as novel therapeutic approaches, are urgently needed.
Two recent studies have independently described the mutation profiles of a newly-discovered cancer-associated gene, protein phosphatase 2 regulatory protein 1A (PPP2R1A), in different subtypes of ovarian and endometrial carcinoma (10, 11). The rationale underlying these studies was derived from a recent report that applied exome sequence analysis to globally identify novel somatic mutations in ovarian clear cell carcinoma (5). PPP2R1A encodes the α isoform of a constant regulatory subunit, A, of protein phosphatase 2, one of the four major serine/threonine phosphatases (12). It consists of a heteromeric core enzyme composed of a catalytic subunit and a constant regulatory subunit, which associates with a variety of regulatory subunits. The constant regulatory subunit A serves as a scaffolding molecule to coordinate the assembly of the catalytic subunit, as well as a variable regulatory B subunit. Biologically, it participates in a variety of cellular functions, including cell-cycle regulation, mitosis, DNA damage repair, and response to hypoxia (13-15), and has been implicated in tumor suppression (16) and virus-associated neoplastic transformation (17).
The present study examined the somatic mutations of PPP2R1A in the four major histological types of ovarian carcinomas (serous, endometrioid, mucinous, and clear cell) in an effort to extend the previous observation of a high frequency of PPP2R1A mutation in mucinous carcinoma (11).
Materials and Methods
Tissue samples. Formalin-fixed, paraffin-embedded tissue samples of 88 ovarian carcinomas, including 22 high-grade serous, 29 mucinous, 15 high-grade endometrioid, and 22 clear cell, were evaluated. These samples were obtained from the Department of Obstetrics and Gynecology at the Shimane University Hospital and the Department of Obstetrics and Gynecology at Seirei Hamamatsu General Hospital. Diagnosis was based on conventional morphological examination of sections that underwent hematoxylin and eosin (H&E) staining, and tumors were classified according to the WHO classification. Tumor staging was performed according to the International Federation of Gynecology and Obstetrics (FIGO) classification (18). All patients were primarily treated with cytoreductive surgery and adjuvant platinum and taxane or irinotecan chemotherapy [Carboplatin AUC5 with paclitaxel at 175 mg/m2 or docetaxel at 70 mg/m2, or cisplatin at 60 mg/m2 with irinotecan at 180 mg/m2]. All patients received 6-12 courses of this combination regimen. Acquisition of tissue specimens and clinical information was approved by an Institutional Review Board (Shimane University and Seirei Hamamatsu General Hospital).
Mutational analysis of PPP2R1A, PIK3CA, KRAS, and BRAF. Genomic DNA was purified from all of the formalin-fixed, paraffin-embedded tissues using a Qiaquick PCR purification kit (Qiagen, Valencia, CA, USA). DNA purified from uterine tissue of the same patients was used as a normal control. Polymerase chain reaction (PCR) was then performed followed by nucleotide sequencing using an iCycler (Bio-Rad, Hercules, CA, USA). PCR amplification was performed using the following primer pairs which were designed to amplify the genomic DNA fragment of exon 5 of PPP2R1A flanking the arginine couplet at codons 182 and183: forward primer 5’-TACTTCCGGAACCTGTGCTC-3’ and reverse primer 5’-CCAGGAAGCAAAACTCACCT-3’. PCR primers used to amplify exon 6 of PPP2R1A were: forward primer 5’-GTTCCTGCCCATGAAAGAGA-3’, reverse primer 5’-TTATTGCTCAAACGCCCAAT-3’, and sequencing primer 5’-AATGGTTCCATCGGCCTAAT-3’.
Exons 9 and 20 of PIK3CA, exon 1 of KRAS, and exon 15 of BRAF were also sequenced, as these mutational hot spots, together, harbor nearly all known published mutations (5, 19, 20). The primers for PCR and sequencing were manufactured by GeneLink (Hawthorne, NY, USA); their sequences have been previously described (21). Sequences were analyzed using the Lasergene program, DNASTAR (Madison, WI, USA).
Statistical methods for clinical correlation. Overall survival was calculated from the date of diagnosis to the date of death or last follow-up. Data were plotted as Kaplan Meier curves, and statistical significance was determined by log-rank test. Data were censored when patients were lost to follow-up. Chi-square test or Fischer's exact test were used for comparisons of categorical data.
Results and Discussion
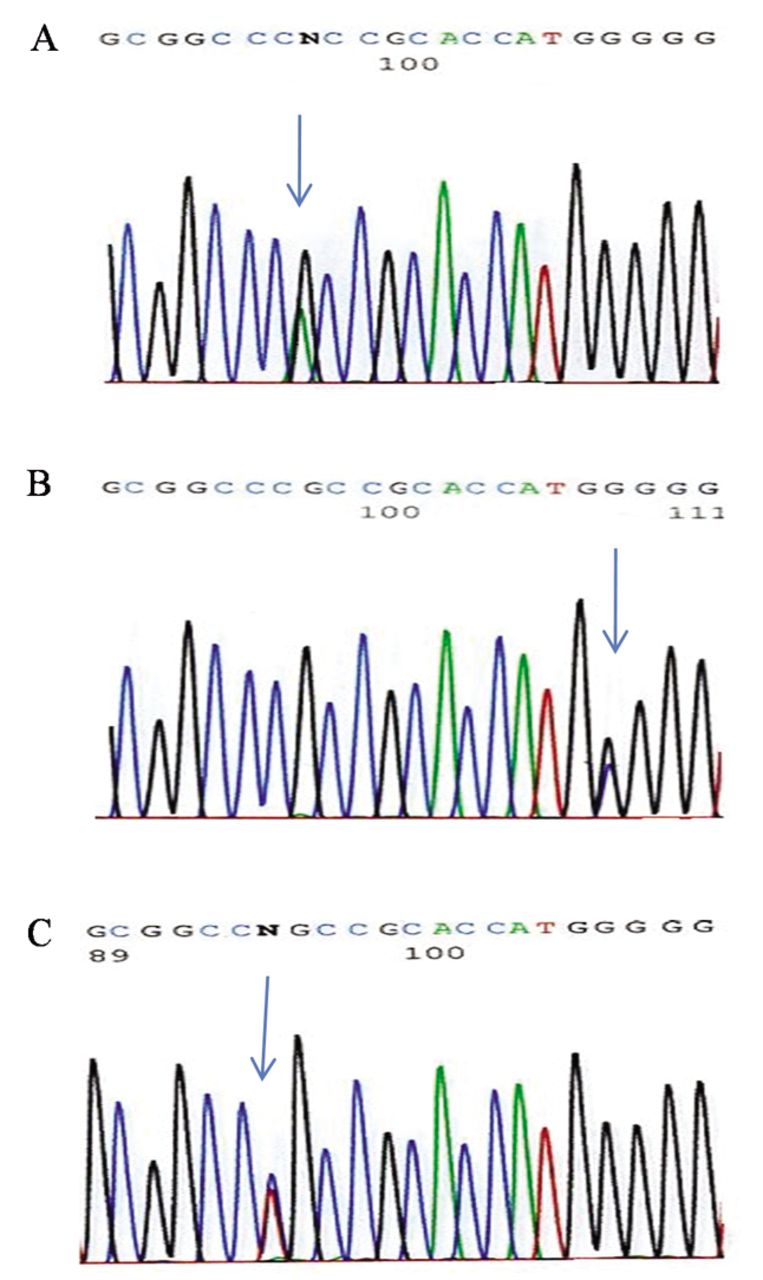
To characterize the spectrum and frequency of PPP2R1A mutations across the histological subtypes of ovarian carcinoma, 88 samples, including 29 mucinous, 22 clear cell, 22 high-grade serous, and 15 high-grade endometrioid ovarian tumor tissues were analyzed. Direct sequencing was performed for exons 5 and 6 because mutations on these two exons have been previously reported (11). PPP2R1A mutations were detected in one (4.5%) clear cell, one (4.5%) high-grade serous, and one (6.6%) high-grade endometrioid carcinoma. Out of these, two mutations involved the R183 hot spot and one mutation involved the P179 hot spot (Table I). These heterozygous missense mutations have also been identified in previous reports (11). Representative chromatograms of these three somatic alterations are shown in Figure 1. However, no PPP2R1A mutations were identified in mucinous carcinomas. Recently, PPP2R1A mutations in 2 out of 6 have been reported in ovarian mucinous carcinoma (11). We expected to make a similar observation in the 29 mucinous ovarian tumor tissues from Japanese women examined in this study. However, the present results demonstrated an absence of PPP2R1A mutations in mucinous subtype carcinomas, likely due to the difference in the total number of mucinous cases.
Pathological and molecular features of 31 ovarian carcinomas with mutations in PPP2R1A, KRAS, BRAF, or PIK3CA.
In addition to PPP2R1A mutations, the mutation frequencies of KRAS, BRAF, and PIK3CA were also determined in the same ovarian tumor tissue samples, as these genes are frequently mutated in ovarian tumors. It is also known that PP2A is implicated in regulation of signaling pathways, including the Mitogen-activated protein kinase (MAPK) and v-akt murine thymoma viral oncogene homolog-1 (AKT) pathways (22, 23). However, no mutually exclusive mutation patterns were observed between PPP2R1A and KRAS or between PPP2R1A and PIK3CA, which is similar to the results of a previous study (11). In the present study, no concurrent PPP2R1A and KRAS mutations were detected, whereas all the PPP2R1A-mutated cases harbored concurrent PIK3CA mutations. In contrast, of the 85 wild-type PPP2R1A cases, 13 (15%) had KRAS mutations and 15 (17%) had PIK3CA mutations. These results suggest that PPP2R1A mutations are not likely to participate in signaling pathways involving KRAS and PI3K. However, further studies are required to confirm potential cross-talk between these pathways.
The mutation frequencies of PPP2R1A, KRAS, BRAF, and PIK3CA among the different histological subtypes of analyzed ovarian carcinomas are shown in Figure 2. Sequence mutations of KRAS, BRAF, and PIK3CA were detected in 24.1%, 6.9%, and 10.3% of analyzed mucinous carcinoma cases, respectively. Some previous reports described an increasing frequency of KRAS mutations in this subtype (3, 4). The present results are also consistent with those reports. Among the genes analyzed, PIK3CA was the most frequently mutated in clear cell carcinoma; 11 out of 22 cases (50%), while the PPP2R1A mutation was observed in 4.5% of clear cell carcinoma cases. These results are also similar to those of previous studies (4, 8, 10). In high-grade serous carcinoma, which is the most frequent type of ovarian carcinoma, mutations of the analyzed genes were observed at a lower frequency (PPP2R1A, 4.5%; KRAS, 9.1%; BRAF, 0%; PIK3CA, 4.5%) in this tumor type. This result supports the molecular features of the dualistic model that has been proposed for ovarian cancer (8).
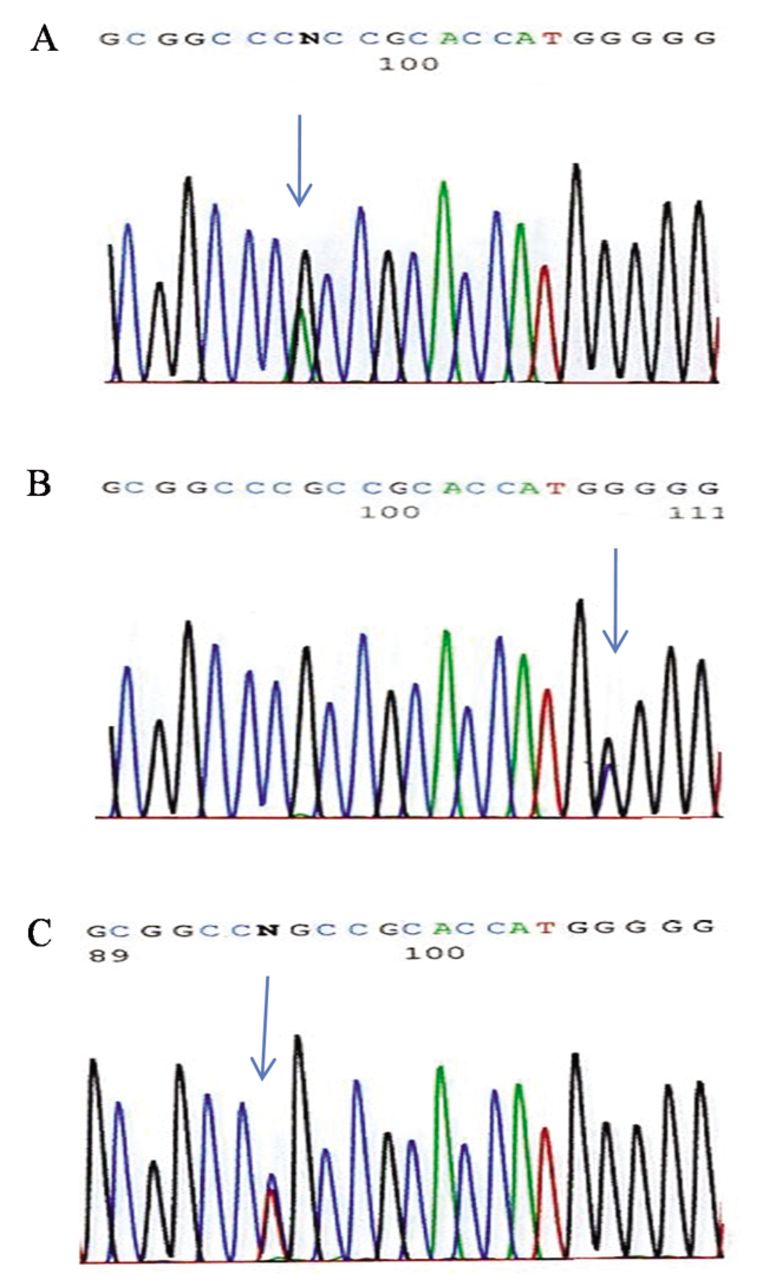
Somatic mutations in serine/threonine-protein phosphatase 2A regulatory subunit A α isoform (PPP2R1A). Arrows indicate nucleotides with sequence mutations. (A) Chromatogram of the sequences demonstrates a mutation in a high-grade ovarian serous carcinoma (547G>A, R183W), (B) a mutation in a high-grade ovarian endometrioid carcinoma (536G>C, P179R), and (C) a mutation in an ovarian clear cell carcinoma (548C>T, R183Q).
In this study, we also included high-grade endometrioid carcinoma, which is thought to be a variant of high-grade serous carcinoma by some pathologists, because of the difficulty in distinguishing high-grade endometrioid carcinoma from high-grade serous carcinoma (8). Mutations in PPP2R1A, KRAS, BRAF, and PIK3CA were identified in 1 (6.7%), 4 (26.7%), 0 (0%), and 3 (20.0%) of 15 high-grade endometrioid tumor cases, respectively. KRAS and PIK3CA exibited relatively high mutation frequencies, which can be explained by the fact that some high-grade endometrioid carcinomas (type II) can display molecular changes found in the low-grade endometrioid carcinomas (type I), suggesting that some low-grade endometrioid carcinomas may progress to high-grade carcinomas. In contrast, the mutation frequency found in high-grade endometrioid tumors may be due to the low number of cases analyzed.
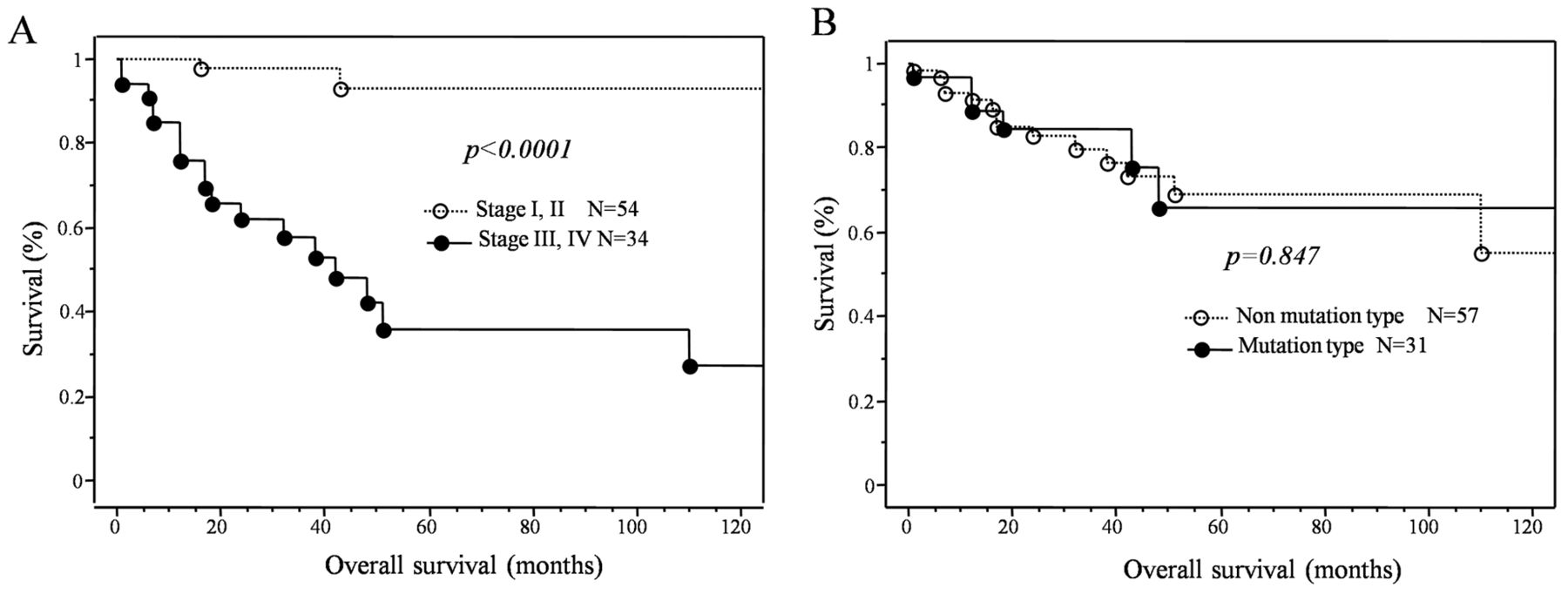
Finally, in an effort to determine prognostic significance of these mutations, the mutation status of the tumors was correlated with overall survival. The Kaplan-Meier estimates of overall survival are shown in Figure 3. No significant relationship was found between the mutation status of ovarian carcinomas and overall survival (p=0.847). In addition, no correlation was observed between type I and type II ovarian cancer and overall survival (p=0.571). However, a significant correlation was found between FIGO stage and overall survival (p<0.0001).

Summary of serine/threonine-protein phosphatase 2A regulatory subunit A α isoform (PPP2R1A), v-Ki-ras2 Kirsten rat sarcoma viral oncogene homolog (KRAS), phosphatidylinositol-4,5-bisphosphate 3-kinase (PIK3CA) and v-raf murine sarcoma viral oncogene homolog B1 (BRAF) mutations analyzed in type I and type II ovarian carcinomas. The frequency of individual mutations in ovarian carcinomas including mucinous carcinoma, clear cell carcinoma, high-grade serous carcinoma, and high-grade endometrioid carcinoma is shown in the bar chart.

Kaplan-Meier survival curve on 88 patients with ovarian carcinoma. A: International Federation of Gynaecology and Obstetrics (FIGO) stage significantly correlates with overall survival. B: The two types of ovarian carcinoma had a statistically non-significant effect on overall survival of patients.
The results of the present study confirmed that PPP2R1A mutation occurs at a low frequency in ovarian carcinoma. Unexpectedly, no PPP2R1A mutations were observed in mucinous ovarian carcinoma. However, out of the three mutations, one occurred in type I tumors and the other two were observed in type II ovarian tumors, which to our knowledge is a novel finding. Although these data indicate that the PPP2R1A mutation indeed occur in ovarian carcinoma, they may not contribute to carcinogenesis of ovarian carcinoma, irrespective of histological subtype.
Acknowledgements
This study was supported by grants from the Ministry of Education, Culture, Sports, Science and Technology in Japan, Suzuken Memorial Foundation and Takeda Science Foundation.
Footnotes
-
Conflicts of Interest
The Authors declare that there are no conflicts of interest.
- Received October 29, 2012.
- Revision received November 20, 2012.
- Accepted November 21, 2012.
- Copyright© 2013 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}