


Abstract
We sought to determine if complete pathological necrosis (pathCR) predicts favorable oncological outcome in soft tissue sarcoma (STS) patients receiving pre-operative radiation monotherapy (RT). Patients and Methods: We evaluated 30 patients with primary STS treated with neoadjuvant RT followed by definitive resection, from 2000 to 2010 at our institution. We defined ≥95% tumor necrosis as pathCR. Results: There were 22 STS of the extremities (73%), 7 of the retroperitoneum (23%), and 1 (4%) of the trunk. The median pathological percentage of tumor necrosis was 35% (range 5-100%) with three tumors (10%) demonstrating pathCR. With a median follow-up of 40 months, the 5-year local recurrence-free survival (LRFS), distant recurrence-free survival (DRFS), and overall survival (OS) for the entire cohort were 100%, 61%±11%, and 69%±11%, respectively. Among patients with pathCR, 3-year DRFS was 100% compared to 63±11% in patients without pathCR (p=0.28). Conclusion: Following neoadjuvant RT for STS, pathCR is associated with a clinically but not statistically significant 37% improvement in 3-year DRFS.
External beam radiation therapy (RT) is an important component of the multi-modality treatment of patients with soft tissue sarcomas (STS). Oncological outcomes have been shown to be essentially equivalent when either pre- or post operative RT is administered, particularly for primary STS located on the extremities (1). Consequently, neoadjuvant RT has gained popularity among sarcoma centers because among its other potential advantages, response to therapy can be assessed using clinical, radiological, and pathological parameters (2, 3).
However, assessment of tumor response or treatment effectiveness remains poorly characterized, and novel imaging and molecular biomarkers remain a priority of clinical cancer research (4, 5). Currently one of the few reproducible markers which is available to clinicians is the degree of induced pathological necrosis in the surgical specimen. Studies in STS and other tumors have demonstrated that high levels of pathological tumor necrosis (pathCR) in surgical resection specimens are correlated with superior oncological outcomes including survival (6-13). However, these studies have been retrospective in nature, have analyzed varying thresholds of tumor necrosis (90% in osteosarcoma, 95% in STS, 99% in rectal cancer), and have employed heterogeneous pre-operative regimens, including multi-agent chemotherapy or chemoradiation (6-13). Consequently, the exact nature of the relationship of complete pathological necrosis to oncological outcome following neoadjuvant therapy remains equivocal, and the significance of pathCR in STS following RT monotherapy has not been well-established.
Therefore, we sought to determine the histological response rates of neoadjuvant RT monotherapy for patients with STS receiving treatment with curative intent to determine if pathCR was associated with overall survival (OS), distant recurrence-free survival (DRFS), and local recurrence-free survival (LRFS). We hypothesized that greater than 95% tumor necrosis at the time of surgical resection would predict favorable oncological outcomes.
Patients and Methods
We identified all patients greater than 18 years old, diagnosed between February 2000 and December 2010 at a single institution with localized intermediate- or high-grade primary STS who were treated with neoadjuvant external beam RT followed by resection with curative intent. All patients were prospectively entered and tracked in a computerized cancer center database. Patients with low-grade primary tumors and those who underwent combination preoperative chemoradiotherapy or investigational therapy were excluded.
A total of 30 patients met entry criteria. Neoadjuvant RT was administered in 2-Gy/day fractions over 25 sessions for a total dose of 50 Gy. Resection was performed 4 to 6 weeks after completion of RT to allow for the resolution of acute toxicities. After obtaining approval from the Institutional Review Board, data were collected on age, sex, tumor location, histological type, primary tumor size, tumor depth, margin status, extent of resection, and postoperative outcomes. These data were analyzed with respect to the percentage of pathological necrosis, LRFS, DRFS, and OS.
Age was determined from the date of diagnosis of the primary tumor. Tumor location was categorized as either upper extremity (upper at, or distal to the shoulder/axilla), lower extremity (at or distal to the buttocks/groin), retroperitoneal, or trunk. Histological grade was classified by a three-tiered system (grade I through III), while histological diagnosis was assigned by the published criteria of the World Health Organization Classification of Tumors of Soft Tissue and Bone (14). Tumor size was divided into three groups: ≤5 cm, 5-10 cm, and >10 cm. Depth was defined as being either superficial or deep to the enveloping fascia. Marginal status was defined as R2 for gross residual tumor following resection, R1 for microscopically-positive margins, and R0 for microscopically-negative margins. Major wound complications were defined based on standardized definitions (1).
Pathological response was assessed using hematoxylin and eosin-stained slides by a single STS pathologist (D.B.) who was blinded to the oncological outcome. The percentage of histologically intact tumor and the percentage of necrotic tumor were scored per slide, and the mean percentage of tumor necrosis was calculated for the entire specimen, excluding non-neoplastic tissue. The median number of slides examined per patient was 10 (range, 8-18). Complete pathological necrosis was defined as greater than 95% tumor necrosis, as previously defined in the literature (6). We chose a more conservative definition due to the difficulty of adjudicating isolated tumor cells as being alive or dead within broad areas of necrosis.
The date of recurrent disease was defined either by biopsy or by radiographic detection of suspicious lesions when no biopsy was performed. Peritoneal recurrences of retroperitoneal sarcomas were considered local recurrences, whereas liver metastases were considered distant recurrences. Duration of follow-up included the interval from the date of diagnosis until the date of death or the date of last follow-up. The local recurrence-free interval was calculated from the date of resection. Patients who were free from recurrence or death were censored according to the date of their last follow-up.
Descriptive statistics were used to analyze frequency distributions. All continuous variables were plotted on a histogram to determine the distribution of data points and to assess for Gaussian distribution. Parametric continuous variables were expressed as the mean (±SD), while non-parametric continuous variables were expressed as median values with ranges. The Kaplan Meier approach was used to estimate survival curves (15). Survival differences were analyzed using the log-rank test. Significance was set at p<0.05. Statistical analyses were performed using SPSS version 17.0 (SPSS Inc, Chicago, IL, USA) and SAS version 9.1 (SAS Institute Inc., Cary, NC, USA).
Clinicopathologic characteristics of patients with soft tissue sarcoma undergoing preoperative radiotherapy and surgical resection with curative intent
Results
Patients' and tumor characteristics. Table I depicts the patient and tumor characteristics of the cohort. The median age was 64 (range 24-86) years, and 60% were women. There were 22 (73%) STS of the extremities, 7 (23%) of the retroperitoneum, and one (3%) of the trunk. The median tumor size was 8.5 (range 3-35) cm. The majority of tumors were high-grade (87%) and located deep to the enveloping fascia (97%). Malignant fibrous histiocytoma/pleomorphic sarcoma (37%), leiomyosarcoma (20%), and myxoid/round cell liposarcoma (20%) comprised the most common histological subtypes.
Outcomes among patients with soft tissue sarcoma undergoing preoperative radiotherapy and surgical resection with curative intent
The treatment and response outcomes are given in Table II. The majority of patients (70%) underwent limb-sparing resections for tumors of the extremities. The overall rate of R0 resection was 80%. There were seven patients (23%) who experienced major postoperative wound complications. Six patients required reoperation for wound debridement and secondary closure. One patient required readmission for wound care and antibiotics, but was managed conservatively.
Pathological necrosis. The median pathological percentage of tumor necrosis for all tumors following neoadjuvant RT was 35% (range 5-100%). Eight tumors (27%) demonstrated greater than 80% tumor necrosis, and three tumors (10%) demonstrated pathCR (≥95% necrosis). The three tumors demonstrating pathCR included an 11-cm high-grade undifferentiated pleomorphic sarcoma of the upper extremity, a 9-cm myxoid/round cell liposarcoma of the lower extremity, and a 7-cm extraskeletal myxoid chondrosarcoma of the upper extremity.
Oncological outcome. With a median follow-up of 40 months, the 5-year LRFS, DRFS, and OS for the entire cohort were 100%, 61%±11%, and 69%±11%, respectively (Figure 1). As shown in Table II, there were no local recurrences, and nine (30%) patients had distant recurrences. Among the nine patients with distant recurrences, six (67%) had STS of the extremities, two patients (22%) had a retroperitoneal STS, and one patient (11%) had a trunk sarcoma. Five out of the eight patients (62.5%) with distant recurrence died of their disease.

Kaplan Meier curve depicting 5-year local recurrence-free survival, overall survival, and distant recurrence-free survival for the entire cohort of soft tissue sarcoma patients treated with pre-operative radiotherapy followed by resection with curative intent.
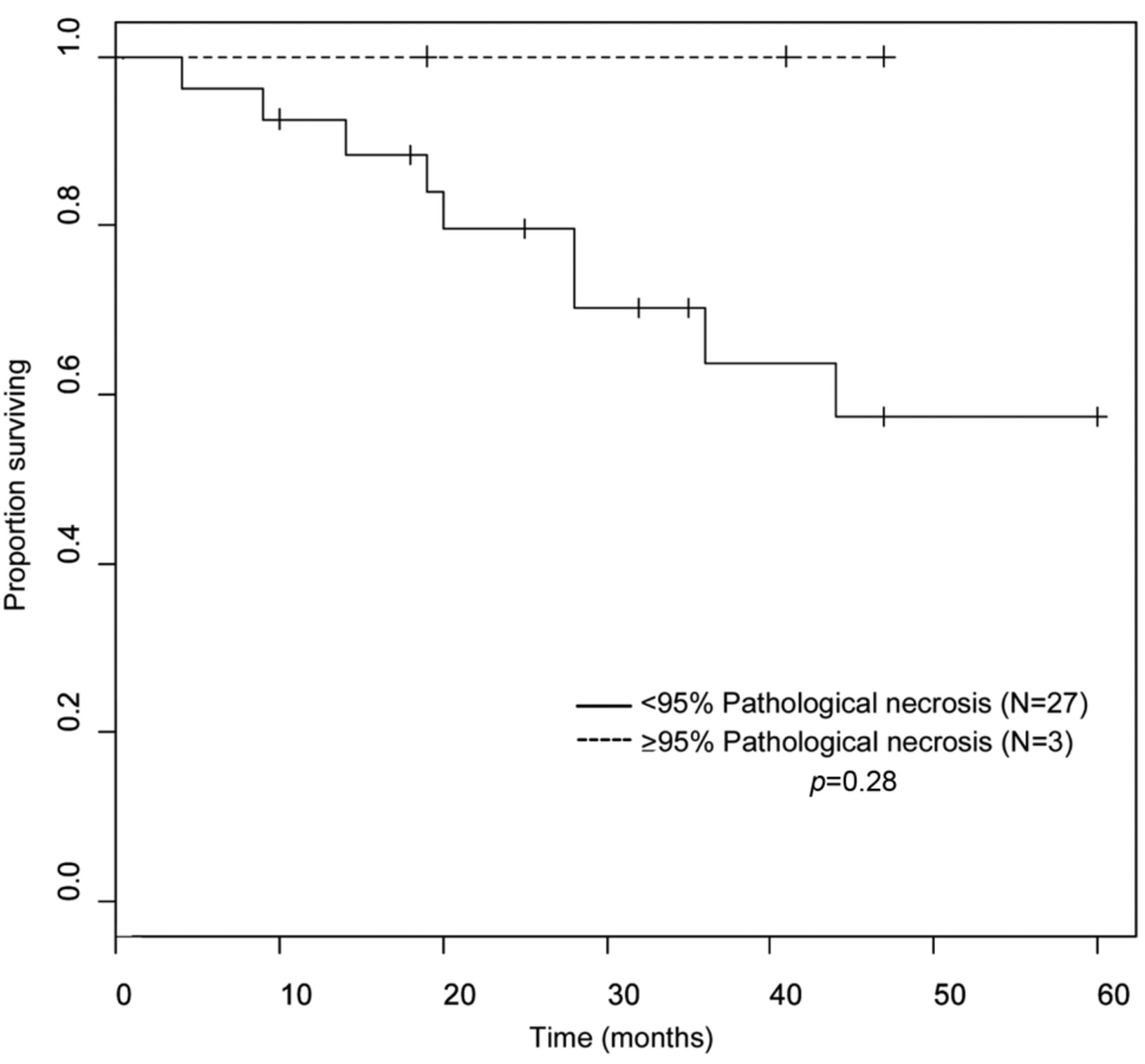
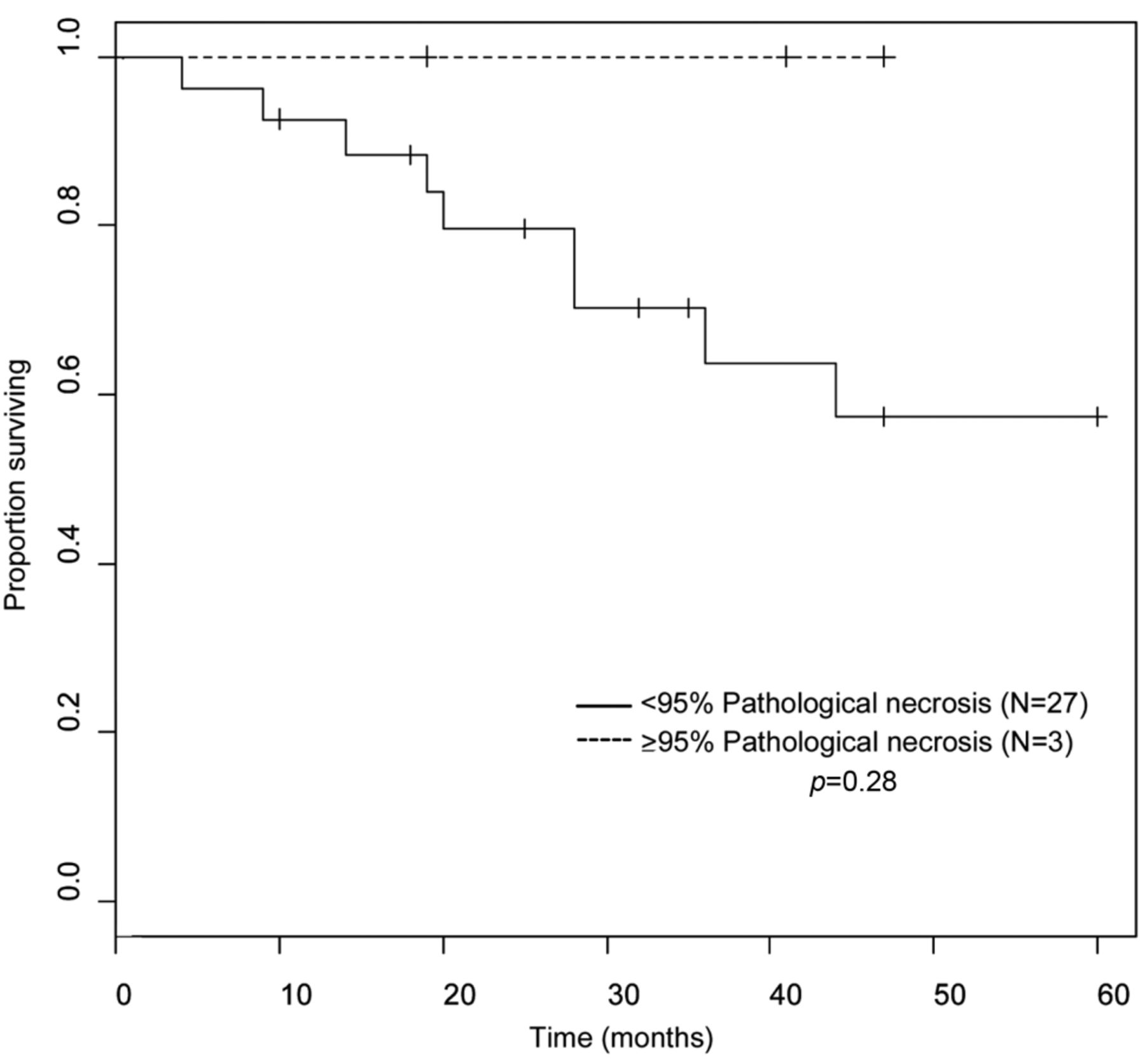
Kaplan Meier curve depicting distant recurrence-free survival grouped by presence or absence of near-complete pathologic necrosis in resected surgical specimen (≥95% tumor necrosis). Log-rank test p-value is shown.
Although there were only three patients (10%) who exhibited pathCR, there were no local recurrences, distant recurrences, or sarcoma deaths in this small subgroup. Conversely, all distant recurrences and deaths occurred among patients with less than pathCR. As depicted in Figure 2, patients with pathCR experienced a 3-year DRFS of 100% compared to 63±11% for patients without pathCR (p=0.28). Although this was not a statistically significant difference, patients without pathCR had a 37% reduction in 3-year DRFS.
Based on previous studies (7, 13) which considered a lower cut-off of pathological tumor necrosis to be associated with favorable oncological outcome (7, 13), we analyzed our data using >80% pathological tumor necrosis in the surgical specimen as the threshold for pathological response. Among the eight (27%) patients with >80% pathological tumor necrosis, DRFS was 27% higher than among the 22 patients with <80% pathological necrosis (88±12% compared to 61±12%, p=0.35). This was also not a statistically significant difference.
Discussion
Radiation therapy, as part of a multimodality treatment strategy, has been shown to reduce local recurrence rates in patients with localized STS of the extremities (3, 16). Local control has also been directly linked to survival in the treatment of retroperitoneal sarcomas, as local treatment failures contribute to patient death (17, 18).
However, there are currently no validated biomarkers which predict response to RT or correlate treatment response to RT with oncological outcome. The degree of treatment-induced pathological necrosis in the surgical specimen continues to be used as a short-term quantitative endpoint in STS (as in other tumors) despite limited data establishing a link between the extent of pathological necrosis and long term outcomes (9). For example, previous studies by Hew et al. and Willett et al. failed to establish a correlation between greater than 80% necrosis and DRFS in STS, when preoperative RT was administered as monotherapy (7, 13). Conversely, both MacDermed et al. and Eilber et al. demonstrated significant improvements in 5- and 10-year survival in patients with STS with greater than 90-95% pathological necrosis, but these results were obtained with combination of neoadjuvant chemoradiotherapy (6, 8).
The significance of pathological necrosis following RT monotherapy and its relationship to oncological outcome is important since multimodal regimens combining RT and novel chemotherapy and/or biological agents are the subject of ongoing investigational studies (2). Given the substantial toxicities of these regimens (19, 20), it will be vital to assess the unique risks and benefits of individual treatment modalities in improving outcomes with a reproducible and validated surrogate endpoint of response.
In our series, we observed a median of 35% tumor necrosis among all patients with STS undergoing neoadjuvant RT monotherapy, and only 10% of patients demonstrated pathCR. Although these rates are lower than those achieved by other studies (29-58%), these differences are likely related to the use of combined chemoradiotherapy by other investigators (6, 8). Some of the studies also employed differences in the technique of RT administration which may have contributed to differences in the degree of pathological necrosis (7, 13). As opposed to the 2 Gy fractions delivered over 25 weeks in our study, both Ryan et al. and MacDermed et al. used a continuous course of hypofractionated (3.5 Gy/day) radiation delivered over 5-10 days (8,11). Willett et al. was able to achieve greater necrosis with twice daily fractionation of RT (13). Thus, fractionation of RT may contribute to the extent of necrosis. In addition, in the series by Eilber et al., the high rates of pathCR appear to have been restricted to patients who received neoadjuvant ifosfamide in addition to RT (6). The rate of pathCR for their entire cohort was only 14%, which is comparable to ours.
Furthermore, it is unclear if these higher pathCR rates with chemoradiotherapy actually translate into improved oncological outcomes (9). For example, 100% pathCR after chemoradiation for gastric or rectal cancer does not translate into reduced risk of distant or regional metastasis (9), possibly due to heterogeneity in the response of local tumor cells and distant micrometastases to chemotherapy. Moreover, combined chemoradiotherapy for STS may not impact on micrometastatic disease since outcomes among patients receiving combined neoadjuvant chemoradiotherapy versus RT monotherapy remain comparable (21). Consequently, given the substantial potential toxicity of intensive chemotherapy, neoadjuvant/adjuvant chemotherapy for STS remains controversial (22).
Our data demonstrate a 37% improvement in 3-year DRFS in patients with pathCR compared to those without pathCR. With a median follow-up of 40 months, we observed no local or distant recurrences among the patients with pathCR, a time period during which the majority of STS recurrences are known to occur (23). Although these would appear to be clinically significant differences in outcome, the rarity of pathCR in our cohort undermines the statistical power of our study. Furthermore, despite the clinically significant differences between the pathCR and non-pathCR cohorts, it remains possible that pathCR after RT monotherapy is not associated with improved long-term oncological outcomes since RT is a local treatment modality and does not address undetectable micrometastatic disease, which theoretically governs DRFS and OS in STS.
In summary, our data demonstrate that pathCR is a rare event in patients undergoing pre-operative RT monotherapy for STS. When it occurs, it is associated with a clinically but not statistically significant improvement in oncological outcome. Our results suggest that pathCR remains a potentially meaningful marker for long-term outcome among patients with STS receiving neoadjuvant RT monotherapy. However, while awaiting the development of novel markers of response to local and systemic therapies for STS, further studies are required to confirm or refute the validity of this important surrogate endpoint as a marker of oncological outcome in STS
Acknowledgements
Statistical support was made possible by grant number UL1 RR024146 from the National Center for Research Resources (NCRR), a component of the National Institutes of Health (NIH), and NIH Roadmap for Medical Research. This article's contents are solely the responsibility of the Authors and do not necessarily represent the official view of NCRR or NIH. Information on Re-engineering the Clinical Research Enterprise can be obtained from http://nihroadmap.nih.gov/clinicalresearch/overview-translational.asp.
- Received May 23, 2012.
- Revision received June 30, 2012.
- Accepted July 2, 2012.
- Copyright© 2012 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Intratumoral talimogene laherparepvec injection with concurrent preoperative radiation in patients with locally advanced soft-tissue sarcoma of the trunk and extremities: phase IB/II trial
- Serum C-reactive Protein and Neutrophil/Lymphocyte Ratio After Neoadjuvant Radiotherapy in Soft Tissue Sarcoma
- First-in-Human Study Testing a New Radioenhancer Using Nanoparticles (NBTXR3) Activated by Radiation Therapy in Patients with Locally Advanced Soft Tissue Sarcomas
- Tail of Superficial Myxofibrosarcoma and Undifferentiated Pleomorphic Sarcoma After Preoperative Radiotherapy