


Abstract
Background/Aim: Serum amyloid A (SAA) has been identified as a potential biomarker for renal cell carcinoma. We examined its diagnostic value in patients of different tumor stages. Patients and Methods: In our study, 48 patients with localized and 67 patients with advanced renal tumors were included. 24 patients served as a control group. Interleukine 6 (IL-6), C-reactive protein (CRP) and SAA levels were measured preoperatively and at day 5 after nephrectomy. Results: The IL-6, CRP and SAA levels in patients with advanced tumors are significantly higher than those of patients with localized tumors. Advanced tumors were identified with a sensitivity of 78% (SAA), 69% (CRP) and 44% (IL-6). The specificity was 82%, 82% and 94% for SAA, CRP and IL-6, respectively. Conclusion: Our results indicate that advanced renal cancers are accompanied by increased levels of acute-phase proteins such as CRP and SAA. SAA is found to be more sensitive than CRP for the indication of advanced renal cancer.
Clinically relevant tumor markers for the diagnosis and the follow-up of renal cell carcinoma are not yet available. None of the parameters so far tested are suitable, to be used as a marker for renal cell carcinoma, due to their low specificity or sensitivity (1). Tumor markers for renal cell carcinoma are urgently needed. Most kidney tumors may cause no symptoms, but approximately 30% of those have already formed metastases at diagnosis, and 30% of the initially localized, curatively-treated renal cell carcinomas metastasize later.
New molecular biology techniques, such as Surface-enhanced laser desorption/ionization time-of-flight mass spectrometry (SELDI-TOF MS) have been used to identify specific protein patterns and potential biomarkers for renal cell carcinoma. A protein that was, in this way, detected, with high sensitivity, in the serum of patients with renal tumors, was serum amyloid A (SAA) (2). SAA is an acute phase protein, like C-reactive protein (CRP), and is produced in the hepatocytes of the liver after cytokine stimulation (3). SAA, however, responds more quickly and with a greater increase, than CRP, to the stimulation of inflammatory cytokines.
It is known that a correlation of cytokines and acute phase proteins with tumor stage, metastasis and prognosis exists in renal cell carcinoma (4-7). On this regardard, the intratumoral expression of interleukine 6 (IL-6) and CRP has been demonstrated (4, 8). This has been also reported for SAA (9). Among other things discussed is the fact, that measurable serum concentrations of these proteins can also be induced by inflammation caused by the tumor (5). The detection of SAA in the serum of patients with renal tumors, as an outstanding proteomic finding on the one hand, and its proposed ability to sensitively respond to an inflammatory stimulus, on the other hand, provide an opportunity to examine whether this protein has sufficient diagnostic validity for the identification of patients with advanced kidney cancer.
Patients and Methods
Patients. One hundred and thirty nine patients were enrolled in our study, for whom a nephrectomy was performed. A total of 115 of them had renal tumors: 48 tumors were small and localized (pT1, group 1); 67 patients had tumors of stage ≥pT2/positive lymph nodes/metastases (group 2). In the remaining 24 patients, nephrectomy was performed due to non-malignant renal disease or in the context of living kidney donation. These patients are summarized in the control group (group 0).
Sample preparation. Blood samples were collected using a standardized procedure. After a clotting time of at least 30 min, the blood samples were centrifuged (1600 ×g, 10 min) and the serum was immediately separated from the blood clot. In cases where the measurement of the parameters could not be immediately performed, after blood sampling, the samples were stored until analysis at −20°C. Repeated freezing and thawing cycles were avoided. The collection of blood samples was performed preoperatively and on the fifth day after surgery.
Distribution of tumor types in the patient groups.
Analytical methods. IL-6 (Immulite One; Siemens Healthcare Diagnostics GmbH, Eschborn, Germany) and CRP and SAA (BN II; Siemens Healthcare Diagnostics Products GmbH, Marburg, Germany) were measured according to the manufacturer's instructions (10, 11).
Statistics. The SPSS version 18.0 software (SPSS Inc., Chicago, IL, USA) was used to perform the following statistical tests: exploratory data analysis, Kolmogorov-Smirnov test for normal distribution, Mann–Whitney U-test for non-parametric random sampling, Pearson's correlation, coefficient and receiver operating characteristic (ROC) analysis. Test results of p<0.05 (two-sided) were considered to be significant.
It was investigated whether statistically significant differences existed between the patient groups. In addition, the sensitivity of each parameter for the indication of advanced tumor stage was calculated. The ability of the parameters to distinguish between the different patient groups was determined by the ROC analysis. The diagnostic accuracy of the parameters was also compared.
Results
Table I shows the patients' characteristics. The majority of the studied cancer patients (77%) had clear cell renal carcinoma; 58% of patients with non-malignant renal diseases had an oncocytoma. Other non-malignant diseases were cystic kidney, cirrhosis of the kidney and malformed kidney.
The preoperative values of IL-6, CRP and SAA in patients with advanced renal cell carcinoma (group 2) were statistically significantly higher than those of patients with small and localized tumors (group 1), as well as compared to those of the control group (group 0). Between the control group and the patients of group 1, no significant differences were observed (Figure 1). All three parameters exhibited similar behavior. SAA, however, had the highest increases in concentration, up to 120-fold the normal value. In contrast, the maximum concentration of CRP was only 40-fold above the normal value, and that of IL-6 only 15-fold above the normal value.
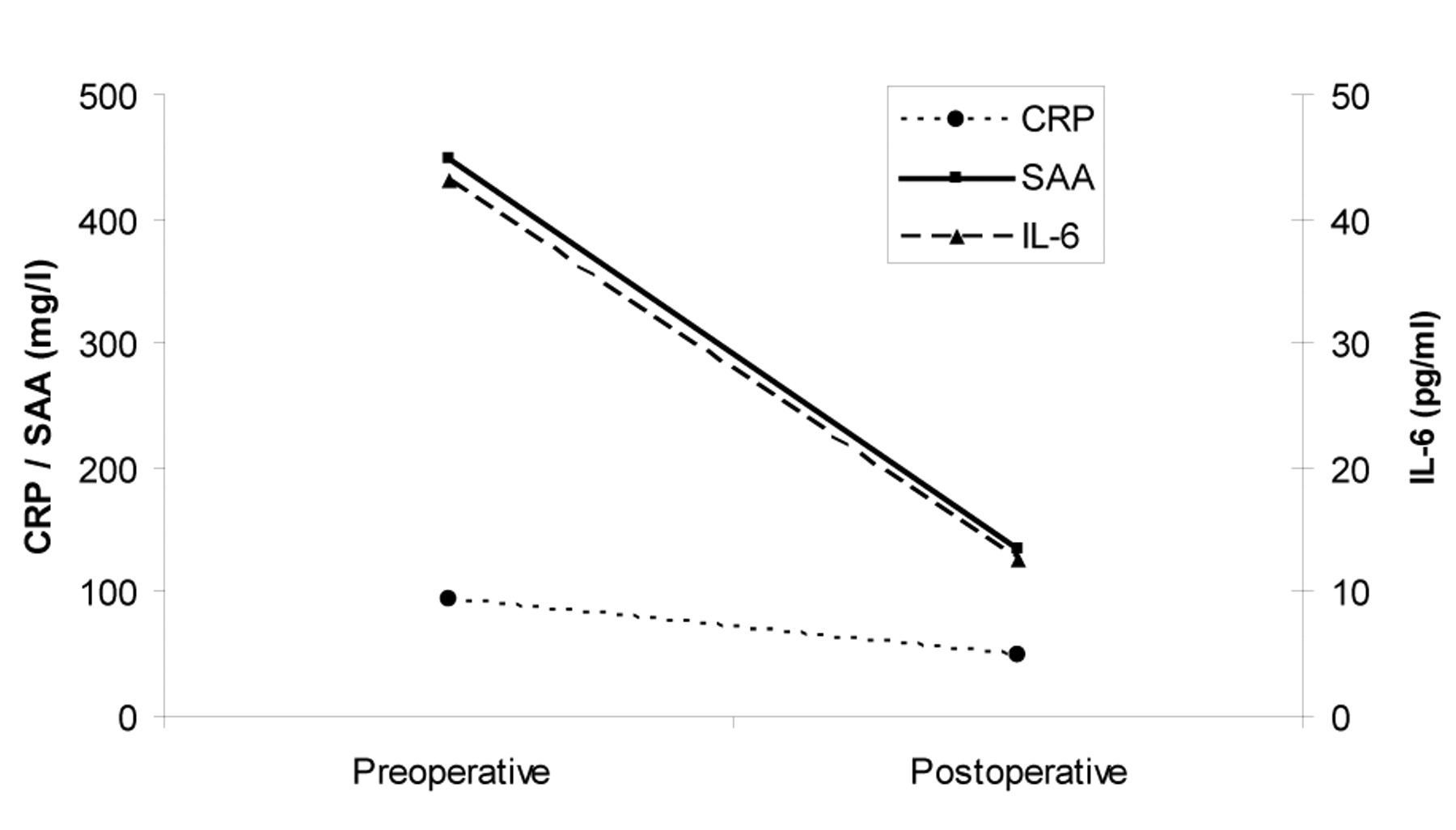
With a sensitivity of 78%, SAA can accurately distinguishe between most advanced tumors of the kidney, with the same specificity as CRP (Table II). The results of the ROC analysis are listed in Table III. It is clear that the correct distinction between group 0 and group 1 by IL-6, CRP or SAA, is not possible, but these molecules can easily distinguish between the control group and patients with advanced cancer. IL-6, CRP and SAA correlate with tumor stage; the Pearson's correlation coefficients are: 0.338, 0.429 and 0.357, respectively (p≤0.00). In 15 patients with very high preoperative SAA values, the SAA concentration dropped below the baseline within five days after the surgery (Figure 2). In a similar manner, but not as pronouncingly, the CRP and IL-6 concentrations decreased after surgery (SAA by 3.9-fold, CRP by 1.9-fold and IL-6 by 3.9-fold).

Box and whisker plots of interleukine 6 (IL-6), C-reactive protein (CRP), and serum amyloid A (SAA) concentrations prior to surgery. Group 0: 24 living kidney donors and patients with non-malignant renal disease; Group 1: 48 patients with small and localized tumors; Group 2: 67 patients with advanced tumors.
Discussion
Our results show that IL-6, CRP and SAA can be elevated in patients with renal tumors, and that their serum levels correlate with the tumor stage. Likewise, it is clear that these parameters are not suitable for the diagnosis of localized renal tumors. With the help of the studied parameters, a discrimination is not possible between the control group and the group of patients with localized malignancy (group 1). However, patients with a tumor stage ≥pT2/positive lymph nodes/metastases have significantly higher IL-6, CRP and SAA serum levels in comparison to the other two groups. Here, SAA has the best diagnostic accuracy (see Table II). Thus, our results are in accordance with data found in the literature (12). However, SAA, like IL-6 and CRP, is not a tumor-specific parameter. All three parameters are involved in inflammatory processes (e.g. induced by infection or trauma). In addition, increased IL-6, CRP and SAA values in the serum of patients with various metastatic tumors, such as of breast, colon, stomach, lung, ovarian and pancreatic cancer were described (13–18). It seems certain that these values have prognostic significance. Their relevance as prognostic markers for renal cancer has been reported several times (6, 7, 12, 19-21). More recent studies have focused primarily on SAA (22-24). There are three reasons for this. Firstly, the SAA protein was detected by Matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF-MS) analysis, with high intensity, in the serum of patients with renal cell carcinoma (2, 25-26). Secondly, the intratumoral expression of SAA was demonstrated (9), and thirdly, SAA is very sensitive to inflammatory stimuli. One might assume that SAA changes in serum correlate with the course of the disease and with the success of treatment. However, only a few publications on the subject exist. Vermaat et al. (27) report that the measurement of SAA during treatment did not establish SAA as an early marker for response. Our data showed that SAA responds, in some cases, very sensitively to the removal of the tumor. As expected, SAA values rise (as well as those of IL-6 and CRP) after nephrectomy as a result of surgical trauma in the context of the induced acute-phase reaction (data not shown). After a short time (on day 5 after surgery), serum concentrations far below the initial concentrations were measured (Figure 2). SAA responded most pronouncedly (see above). This may indicate that the measured concentration of SAA comes from two sources. The tumor itself could be a source. Another source of the elevated SAA levels in the serum could be the acute-phase reaction which is caused by cytokines of the tumor. Using SAA, it might be possible to monitor patients with regard to the occurrence of metastasis or recurrence of the tumor. For that purpose, however, further prospective studies are required.
Sensitivity regarding the detection of advanced renal tumors (correct assignment to group 2) and specificity regarding the detection of advanced renal tumors (correct assignment to group 0 and 1).
Receiver operating characteristic (ROC) analysis.

Concentrations of interleukine 6 (IL-6), C-reactive protein (CRP), and serum amyloid A (SAA) before and five days after surgery (arithmetical mean of 15 patients).
Conclusion
Advanced renal tumors are more common than small, localized tumors, with an accompanying increase of the cytokine IL-6 and of the acute-phase proteins CRP and SAA. Compared with IL-6 and CRP, SAA is more sensitive at indicating an advanced stage of cancer. However, localized tumors of the kidney cannot be detected in this way.
- Received March 7, 2012.
- Revision received April 5, 2012.
- Accepted April 9, 2012.
- Copyright© 2012 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}