


Abstract
Despite great improvements in the management of metastatic clear cell renal carcinoma, complete responses with antiangiogenic therapies are infrequent and complete pathological responses remain anecdotal. We report the complete pathological response of a solitary bone metastasis from a clear cell renal carcinoma after sequential treatment with sunitinib and radiotherapy. In February 2009, a female patient was diagnosed with clear cell renal carcinoma of the left kidney, bearing only one metastatic site localized in the proximal extremity of the left tibia. Radical nephrectomy was performed at first. Thereafter, sunitinib was administered at standard dose level for four weeks followed by two weeks free at each cycle. The patient underwent palliative radiotherapy between the fifth and the sixth cycle. Due to stable status, a radical surgery of the left knee was then performed and pathological analysis concluded a complete response. This case highlights potential synergy between sunitinib and radiation therapy in clear cell renal carcinoma.
Antiangiogenic targeted therapies have demonstrated significant survival improvement in metastatic clear cell renal cell carcinoma (RCC) compared to interferon (1-5). Sunitinib and other tyrosine kinase inhibitors (TKIs), such as pazopanib, axitinib and sorafenib, lead to an overall response rate from 10 to 47% as assessed with RECIST criteria (1, 3-9). Nevertheless, complete responses are infrequent with these new therapeutic agents; near 3% even if RECIST criteria are not always predictive of TKI efficacy. Mammalian Target of Rapamycin (m-TOR) inhibitors, such as temsirolimus, as first-line therapy, or everolimus as second- or third-line therapy, have demonstrated few objective responses but an interesting tumor stabilization rate (2, 10). According to RECIST criteria, some data suggested that primary renal tumors did not respond as well as their corresponding metastatic locations, with objective responses ranging from 0 to 23% (11-15).
Standard radiation therapy alone cannot induce a complete response in a metastatic site due to the intrinsic resistance of RCC and toxicity-limiting doses used. A possible sensitizing effect of sunitinib to radiation has been mentioned in several studies (16, 17). A synergic association between radiotherapy and sorafenib or mTOR inhibitors was also suggested (18, 19).
Here, we report a case of complete pathological response in a solitary bone metastasis after sequential therapy with sunitinib followed by radiation therapy, highlighting a potential synergy between these two treatments. Informed consent was obtained from the patient.
Case Report
A 60-year-old woman was admitted to our center (La Conception Hospital, Marseilles, France) in February 2009 for investigation of pain of the left knee, existing since December 2008. She had a history of hypercholesterolemia equilibrated under Atorvastatine at 20 mg once a day, and was known to have iodine allergy.
A computed tomography (CT) scan and magnetic resonance imaging (MRI) of the left knee were performed. MRI showed an osteolytic lesion of the left tibial plateau (33×25×27 mm) with T1 hypersignal and enhancement after gadolinium contrast agent injection (Figure 1a and 2a). The patient underwent a bone biopsy in March 2009. The pathological analysis concluded the mass was a bone metastasis from clear cell renal carcinoma.
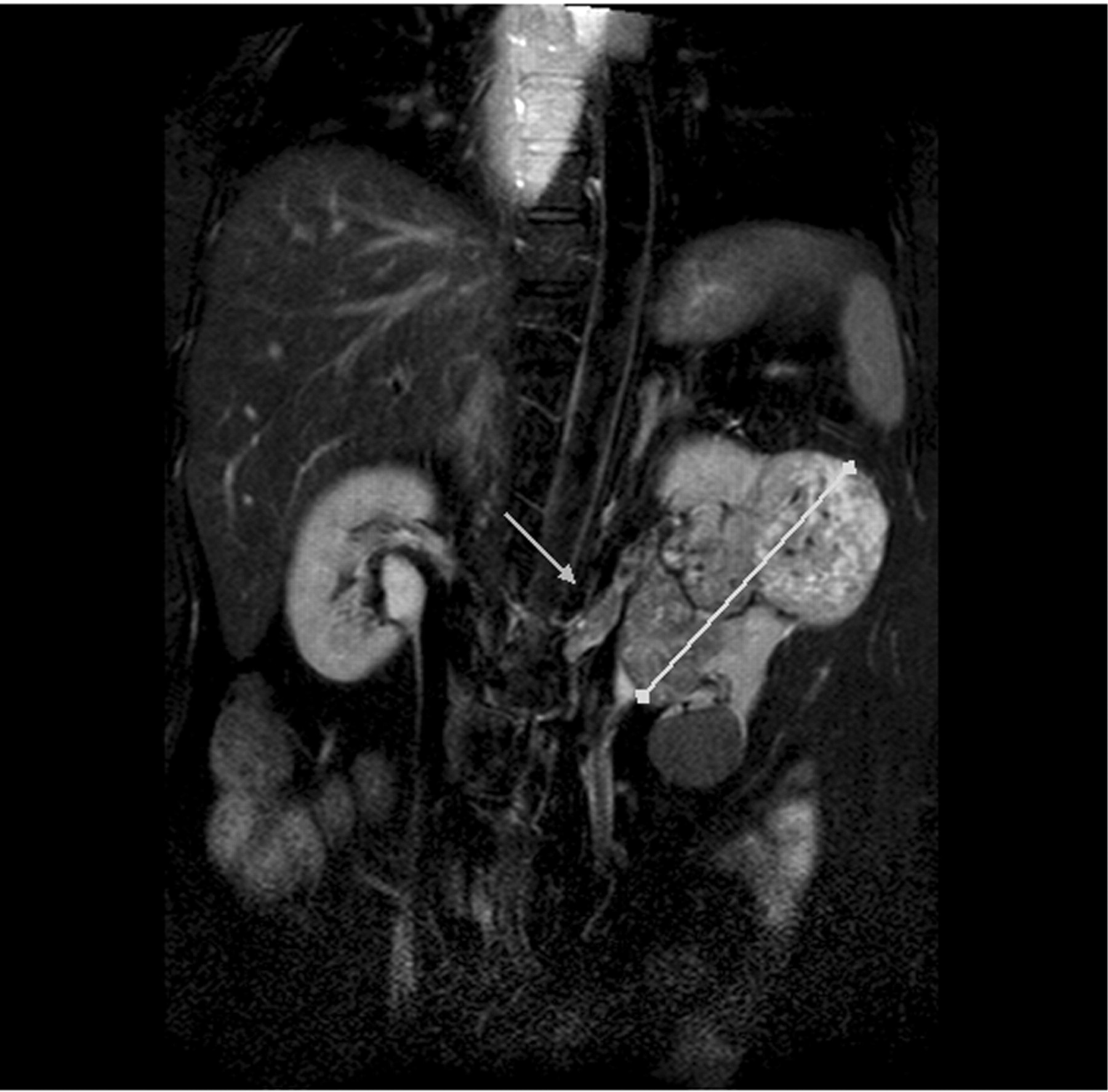
A staging evaluation was then performed consisting of abdominal MRI, CT scan of the brain, chest, abdomen and pelvis, and bone scan. The evaluation showed a primary tumor (60×60 mm) of the left kidney with extension to the renal vein and inferior vena cava (Figure 3). No other distant lesion was identified by CT scan, MRI or bone scan, except the bone metastasis localized in the proximal extremity of left tibia.
The patient underwent left radical nephrectomy and thrombectomy in April 2009. Pathological analysis confirmed a Fuhrman grade 3 clear cell renal carcinoma, staged pT3bpN0 according to TNM 2002 classification (20).
According to Memorial Sloan-Kettering Cancer Center (MSKCC) criteria (21), the patient belonged to intermediate prognosis group (Table I) and sunitinib was administered at the standard dose level of 50 mg daily for four weeks every six weeks in May 2009. After two cycles, the dose was reduced to 37.5 mg daily for four weeks followed by two weeks free, due to gastrointestinal toxicities. The patient received 15 cycles including two early aborted cycles due to grade III digestive side-effects (diarrhea and vomiting). Moreover, an anti-osteoclastic treatment was added consisting of zoledronate administered intravenously monthly. Disease in the patient was restaged every three cycles by CT scan of chest, abdomen and pelvis and every six cycles by bone scan. During treatment, no new lesion was detected and every evaluation concluded in stable disease.
Due to persisting pain of the left knee despite adapted analgesic treatment, radiotherapy to the bone metastasis was decided in January 2010. A total dose of 35 Gy was delivered in 10 fractions during the two weeks free of sunitinib (between the sixth and seventh cycle) without any skin, or soft tissue toxicity. After completing radiation therapy, pain and impotence decreased. CT scan of brain, chest, abdomen and pelvis, bone scan and MRI of the left knee were performed in February and June 2010. They only showed the persistence of the left knee metastatic localization. From March 2009 to November 2010, the size of the lesion increased from 33 mm to 44 mm by MRI evaluation but a large central necrosis had developed, with persistence of peripheral enhancement (Figure 2b).
Radical surgery of the bone metastatic site was decided in February 2011. Sunitinib was stopped after the 15th cycle, 32 days before the surgery; a resection of the proximal extremity of the left tibia was then performed with clear margins (Figure 4). The pathological analysis found no residual tumor cells and concluded there was a complete pathological response of the metastatic site. Clinical and radiological follow-up was decided and sunitinib was definitively stopped.
Ten months after surgery, the patient was still free of disease, as assessed by bone scan and CT scan of chest, abdomen and pelvis.
Discussion
To our knowledge, this is the first description of a complete pathological response for a bone metastatic site after sequential therapy with sunitinib followed by radiotherapy for a metastasis of clear cell renal carcinoma. The metastatic nature of the bone lesion was pathologically documented before systemic treatment initiation and staging evaluation concluded there was a solitary metastasis. The patient is actually free of recurrence but a longer follow-up is needed.
Complete pathological remission has been previously described for primary renal clear cell carcinoma after sunitinib followed by nephrectomy (22). In 2009, Robert et al. presented the first case of complete histologic response of a primary renal clear cell carcinoma after six months of sunitinib (22). Recently, Vaz et al. (23) reported a complete pathological response of a retroperitoneal metastasis from a clear cell renal carcinoma after sunitinib therapy. Nevertheless, at 12 months' follow-up, the patient experienced disease relapse and sunitinib was reintroduced.
Interestingly, our case highlights the potential synergy between radiation therapy and antiangiogenic therapies. Here, the radiation dose was not standard with an hypofractionated scheme (3.5 Gy per fraction) instead of a standard fraction of 2 Gy per fraction. Radiation therapy was delivered during the two weeks free of treatment and systemic treatment with sunitinib was not delayed.
It remains unclear whether sunitinib alone, radiation therapy, or both induced the complete response in our patient. Taussky and Soulieres suggested a synergistic action between radiation therapy and sunitinib for metastases from renal cell carcinoma; a single dose of 8 Gy of external beam radiation was delivered to a metastatic mass by the authors (17). Staehler et al. reported the efficacy of radiotherapy combined with sunitinib for clear cell renal carcinoma metastases in 22 patients, without limiting toxicity (16).
In our case, radiotherapy was delivered to the proximal extremity of the left tibia and no toxicity was observed. Nevertheless, toxicities could be greater for deep metastatic lesions near critical organs such as the bowel, spinal cord and brain. Consequently, with the same strategy as we used, side-effects should be closely monitored for other localizations.
These observations underlined the potential of combining modern techniques of radiation therapy with an antiangiogenic drug for patients with stable or responsive metastatic disease.
As suggested by several studies, surgery is probably one of the most important aspects of a multimodal strategy in patients with few metastases when a curative attempt is made and possible. Data from retrospective series showed higher survival rates with such an aggressive management (24-26). Nowadays, even if a sequential or concomitant treatment with sunitinib and radiotherapy is used, surgery should be thereafter proposed whenever possible. Firstly, it is the only way to treat metastatic sites in selected patients, and secondly, it could be used to assess the rate of complete pathological responses in patient treated with sunitinib followed by radiotherapy.
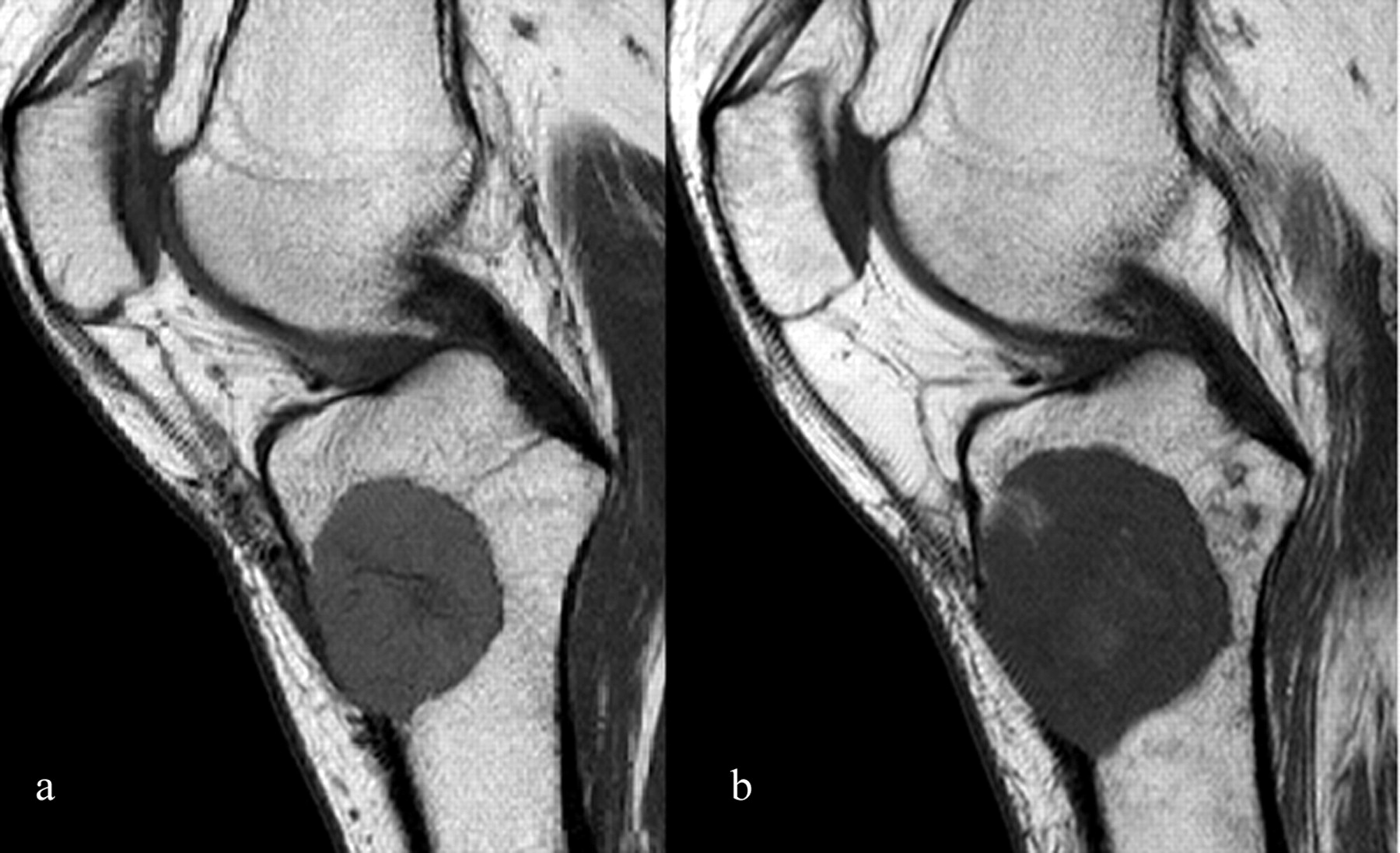
Magnetic resonance imaging (T1) of the left knee before (a) and after (b) sunitinib and radiotherapy.
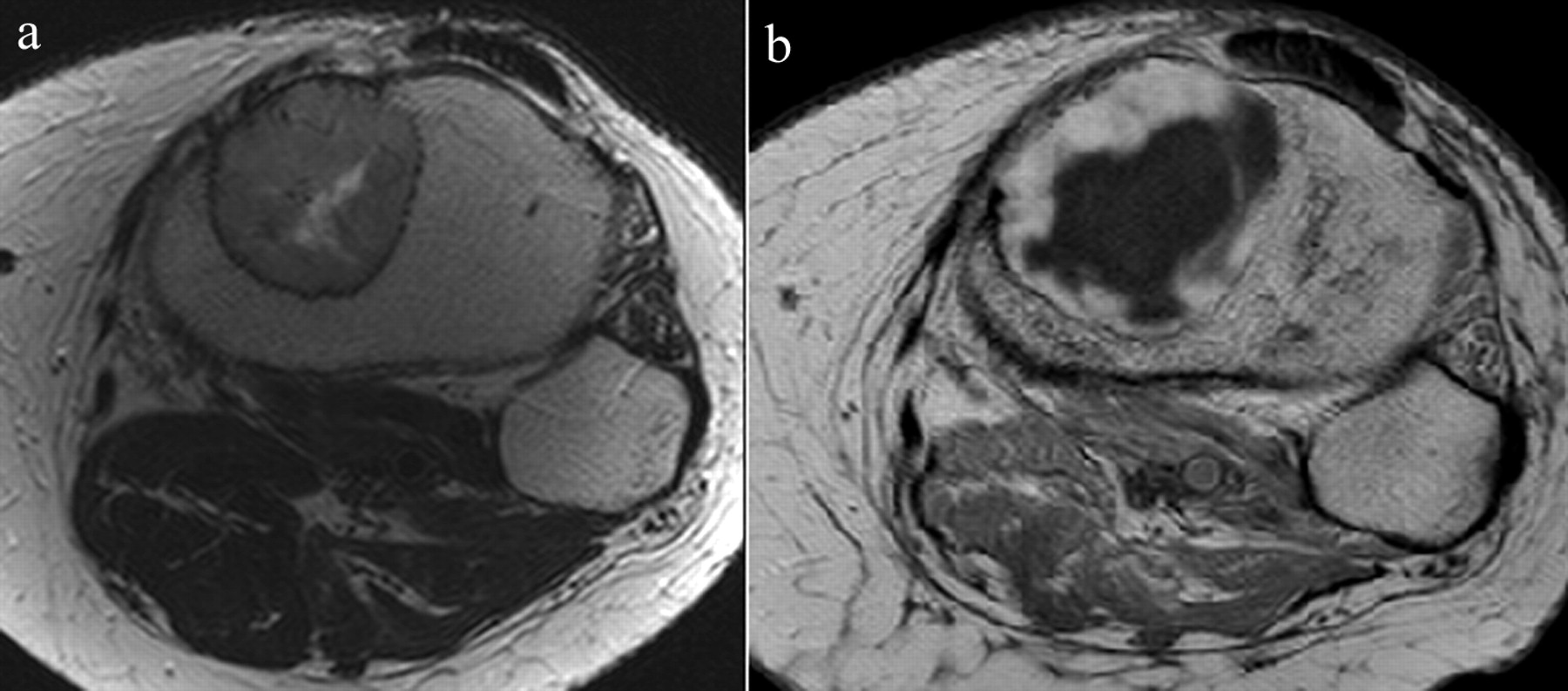
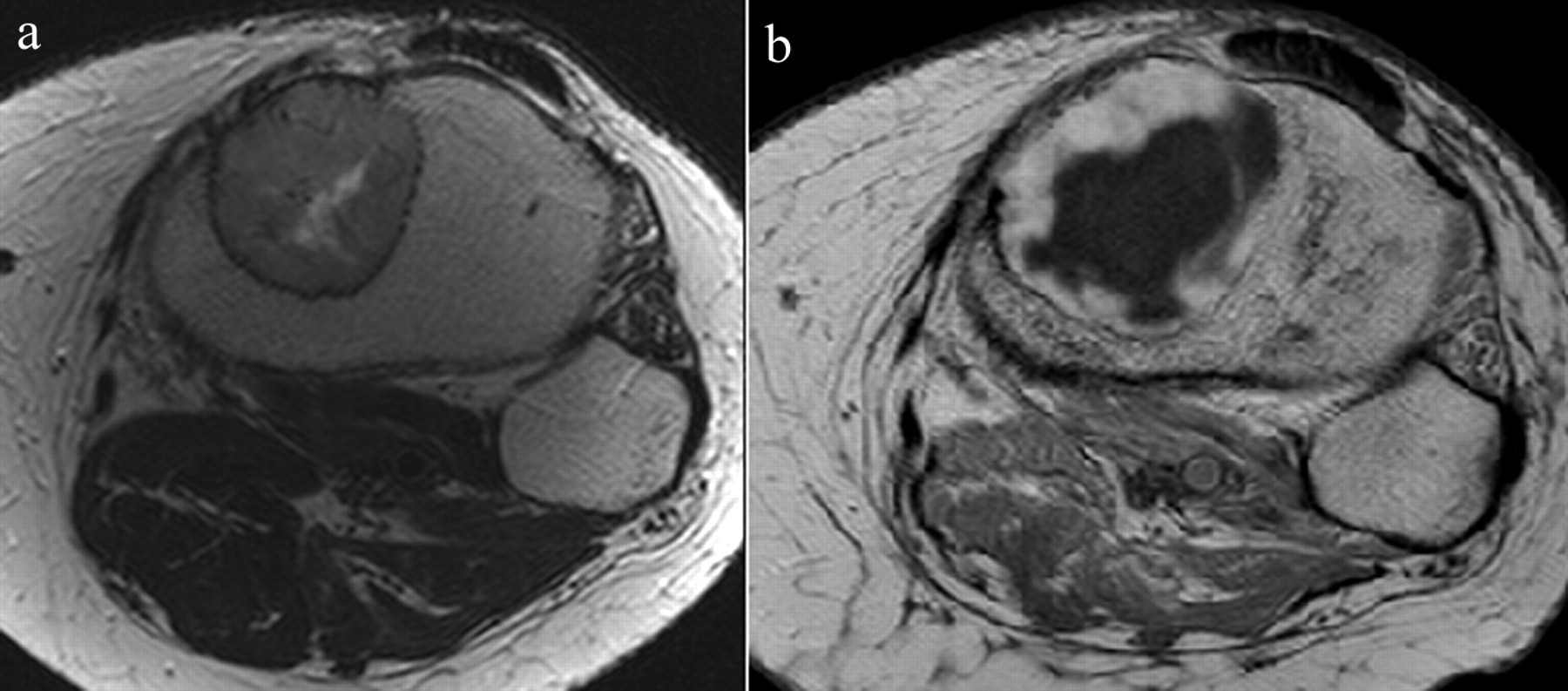
Axial gadolinium-enhanced T1-weighted magnetic resonance image of the left knee showing global enhancement before sunitinib and radiotherapy (a) and central necrosis with persistent enhancement after treatment (b).
Patient characteristics.

Abdominal magnetic resonance imaging (T2 Fat-Sat), showing a primary tumor of the left kidney, with left renal vein invasion (arrow).
Another interesting aspect is the discordance between response as assessed by MRI and CT scan and the pathological response. The size of the bone lesion was stable in our case, with a trend towards increase before radical surgery. Development of necrosis was probably associated with sunitinib activity. Despite RECIST criteria not being adapted to evaluate the response for bone metastatic localization, our observation highlights the issues of criteria using size to evaluate the responsiveness of cancer treated with antiangiogenic therapy. Moreover in our case, after sunitinib and radiotherapy, MRI evaluation of the secondary bone lesion suggested the persistence of viable tumor cells linked to the persistence of peripheral enhancement after gadolinium contrast agent injection. In contrast, pathological analysis confirmed the absence of residual tumor cells.
The limitations of results from a case report are known and we do not suggest that combining radiotherapy and sunitinib should be extensively proposed to patients treated for metastatic clear cell renal carcinoma. However, it could be an interesting strategy for patients presented with a few but unresectable metastases, and stable or responsive disease under antiangiogenic therapy. This kind of strategy deserves further study.

Standard X-rays of left knee after radical surgery of the solitary bone metastasis localized in the proximal extremity of the left tibia.
- Received November 29, 2011.
- Revision received December 19, 2011.
- Accepted December 21, 2011.
- Copyright© 2012 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Related Articles
Cited By...
- No citing articles found.