


Abstract
Purpose: The study aimed to evaluate the efficacy of concurrent chemoradiotherapy (CCRT) with platinum-based chemotherapy as a primary treatment for nasopharyngeal carcinoma (NPC) and to further compare the results of CCRT with these of neoadjuvant chemotherapy (NAC) followed by radiotherapy (RT). Patients and Methods: Before 1998, 21 patients with NPC received NAC followed by RT (NAC-RT). Between 1999 and 2008, a total of 25 NPC patients received CCRT. The CCRT group received a regimen including docetaxel (50 mg/m2, day1), cisplatin (CDDP, 60 mg/m2, day4) and continuous 5-fluorouracil (5-FU) infusion (600 mg/m2, day 1-5), the TPF regimen, or a regimen including CDDP (60 mg/m2, day4), continuous 5-FU infusion (600 mg/m2, day 1-5), methotrexate (MTX, 30 mg/m2, day 1) and leucovorin (LV, 20 mg/m2, day 1-5), PFML regimen. The CCRT group received 2 cycles of chemotherapy during definitive RT. The NAC group of patients received a PFML regimen. Results: The overall response rate after CCRT was 96%. The 3-year and 5-year disease-specific survival rates were 75.6% and 60.1%, respectively. In patients receiving NAC-RT, the 3-year and 5-year disease-specific survival rates were 84.1% and 67.3%, respectively. There was no difference observed in terms of survival rates between the group receiving CCRT and that receiving NAC-RT. Conclusion: CCRT with the TPF or PFML regimen was tolerable, and the NPC patients receiving this treatment showed excellent survival rates. In comparison to the group receiving NAC-RT, CCRT had no advantage in terms of the survival rate. In the future, the control of distant metastasis might play an important role in improving the survival rate of patients with advanced NPC receiving CCRT.
Nasopharyngeal carcinoma (NPC) is an extremely rare cancer in Japan. NPC is considered unresectable because of its unique anatomical location, and radiotherapy (RT) is the standard treatment modality. NPC is considered to be not only radiosensitive but also chemosensitive. On the basis of these characteristics, several randomized trials using RT plus chemotherapy for treating NPC have been conducted (1-8). The results of these trials showed that concurrent chemoradiotherapy (CCRT) either with or without maintenance chemotherapy is considered more effective than RT alone.
Currently, chemotherapy regimens that include cisplatin (CDDP) and 5-fluorouracil (5-FU) (PF) are considered to be the standard treatment for patients with squamous cell carcinoma of the head and neck (HNSCC). Since 1995, we have been developing a multiagent chemotherapy for locoregionally advanced HNSCC, this regimen consists of PF with methotrexate (MTX) and leucovorin (LV) (PFML) (9-11). PFML was initially used in the neoadjuvant chemotherapy (NAC) setting study. Since the end of 1998, PFML has been employed as chemotherapy in CCRT for a phase II trial (9). The results showed the improvement of locoregional control, survival and organ preservation rates of advanced HNSCC patients (9-11).
Recently, for advanced HNSCC, NAC with the docetaxel plus PF regimen (TPF) followed by RT has been proven to be more efficient than the PF regimen in terms of survival (12, 13). We have also examined the safety and efficiency of TPF in the NAC setting (14). Furthermore, patients treated by CCRT with the TPF regimen (15, 16) showed that this regimen results in a better survival rates for advanced HNSCC than NAC with TPF followed by definitive RT. The efficacy of CCRT with the PFML or TPF regimen was studied as a phase II trial (17, 18).
Before 1998, NAC with the PFML regimen followed by RT was administered to NPC patients in our department. Taking into consideration the reports of CCRT for NPC, we have been treating patients with CCRT with the PFML regimen since 1998. Furthermore, CCRT with the TPF regimen has been used since 2003.
The aim of the present study was to retrospectively evaluate the efficacy and toxicity of CCRT with the TPF or PFML regimens and further, to compare the results of CCRT to that of NAC followed by RT.
Patients and Methods
Patient population. Those patients who received CCRT with the TPF or PFML regimen at Yokohama City University Hospital between September 1998 and November 2008, for histologically proven, WHO classification (19), previously untreated nasopharyngeal squamous cell carcinomas were retrospectively reviewed. To be eligible, all the patients had to have an at least one dimensionally measurable lesion, with no distant metastasis and no concurrent malignancies.
For the purpose of the analysis of the CCRT survival benefit analysis, the patients treated by NAC with the PFML regimen followed by RT before 1998, were compared to the patients treated by CCRT. The survival rates and the patterns of relapse for each group were compared.
Treatment schedule. As in our phase I study of the TPF regimen (15), docetaxel (50 mg/m2) was administered intravenously for 1 h on day 1. More than 1 h after completion of the intravenous docetaxel, 5-FU (600 mg/m2/day) was administered by continuous intravenous infusion with 3.5 L of normal saline per day on days 1-5. CDDP (60 mg/m2) was administered intravenously on day 4. The PFML regimen consisted of a combination of 4 drugs: CDDP (60 mg/m2, day 4), 5-FU (600 mg/m2/day, days 1-5), MTX (30 mg/m2, day 1) and LV (20 mg/m2/day, days 1-5) (9-11).Two cycles of each regimen were administered every 4 weeks during RT.
NAC with the PFML regimen consisted of CDDP (60 mg/m2, day 4), 5-FU (800 mg/m2/day, days 1-5), MTX (30 mg/m2, day 1) and LV (20 mg/m2/day, days 1-5). The RT was schedualed to begin 21 days after chemotherapy.
In both of the CCRT group and the NAC group, RT was performed 5 days a week with a single daily fraction of 1.8 or 2.0 Gray (Gy) using 6 MV X-ray linear accelerators.
Toxicity assessment. Toxicity was assessed once per cycle according to the Common Terminology Criteria for Adverse Events version 3.0 (CTCAE v3.0). Before initiating the second treatment cycle, resolution of side-effects (e.g., myelosuppression, mucositis, fever (>38.0°C)) and other disorders was required.
Statistical analysis. Disease specific survival (DSS) times were calculated as the time from the conclusion of RT until death. Progression-free survival (PFS) times were calculated as the time from the conclusion of RT until the date of progression or the date of last follow-up for any other reasons. DSS and PFS curves were calculated using the Kaplan-Meier method. Differences in survival were examined according to log-rank criteria. Differences were considered statistically significant at p < 0.05.
Patients' characteristics.
Results
CCRT group. Twenty-five patients received CCRT with TPF or PFML chemotherapy. The patients' characteristics and staging are listed in Table I.
Six patients received TPF chemotherapy and 19 received PFML chemotherapy. Twenty-one patients (84.0%) completed the scheduled CCRT (4 TPF cases and 17 PFML cases). The second course was discontinued in 4 cases because of chronic neutropenia in 2 patients and renal toxicity in 2 patients. The median dose of radiation was 67.4 Gy (range, 61.2-75.0).
Responses and survival. In the patients receiving CCRT with either TPF or PFML, the overall response rate (RR) in the primary tumors was 96% (20 complete response (CR) and 4 partial response (PR)) and 95.5% (20 CR and 1 PR) in the neck lymph- node involved cases. The RR in the stage I/II group was 100% (7 CR and 1 PR) and 94.1% (13 CR and 3 PR) in the stage III/IV group.
The RR in the TPF group was 83.3% (5 CR and 1 no change (NC)) and 100% (15 CR and 4 PR) in the PFML group. Only 1 patient (T4aN1M0), who was treated with TPF showed NC in the primary and neck lymph- node sites.

Kaplan-Meier survival curves in months for patients given CCRT (TPF or PFML). (a) Disease -specific survival rate. The 3-year, and 5-year DSS rates were 75.6% and 60.1%, respectively (b) Progression-free survival rate. Both the 3-year and 5-year PFS rates were 52.4%.
After a median follow-up of 51.7 months (range, 9.7-114.7 months), 14 patients were still alive with no evidence of disease (NED). One patient was alive after neck dissection for neck lymph- node relapse. Three patients were alive after relapse. Seven patients died as a result of tumor relapse.
In the patients with stage I/II, six patients had NED and two patients died from relapse. In the patients with stage III/IV, eight patients had NED, four were alive after relapse and five patients died from tumor progression or relapse.
For all 25 patients, the 3-year, and 5-year DSS rates were 75.6% and 60.1%, respectively, and both the 3-year and 5-year PFS rates were 52.4% (Figure 1). In the TPF group, the rates of both 3-year and 5-year DSS were 75.0% and in the PFML group, the 3-year and 5-year DSS rates were 77.1% and 56.2%, respectively (Figure 2).
In the stage I/II group, both the 3-year and 5-year DSS rates were 75.0%, and both the 3-year and 5-year PFS rates were 72.9%. In the stage III/IV group, the rates of 3-year and 5-year DSS were 77.0% and 49.5%, respectively, and both the 3-year and 5-year PFS rates were 40.0%.
Toxicity. There were no deaths resulting from the treatment. Table II presents the toxicities. Mucositis was the most common grade 3 and 4 toxicity observed; 10 patients had Grade 2 (40%) and 14 had Grade 3 (56%). The second most common grade 3 and 4 toxicity was leukopenia associated with CCRT, grade 3 and 4 occurred in 40% (10/25) of the patients. Furthermore, Grade 3 and Grade 4 neutropenia was observed in 36% (9/25) of the patients.
Comparison with the group receiving NAC followed by RT: Before 1998, 21 patients received NAC with PFML chemotherapy followed by RT (NAC-RT), and their characteristics and staging are described in Table I. There were no significant differences between the CCRT group and the NAC-RT group in gender, age, histopathological classification, stage and median radiation dose.

Kaplan-Meier survival curves for patients given CCRT with TPF or PFML. In the TPF group, the 5-year DSS rate was 75.0% and in the PFML group, the 5-year DSS rate was 56.2%.
Toxicities during concurrent chemoradiotherapy.
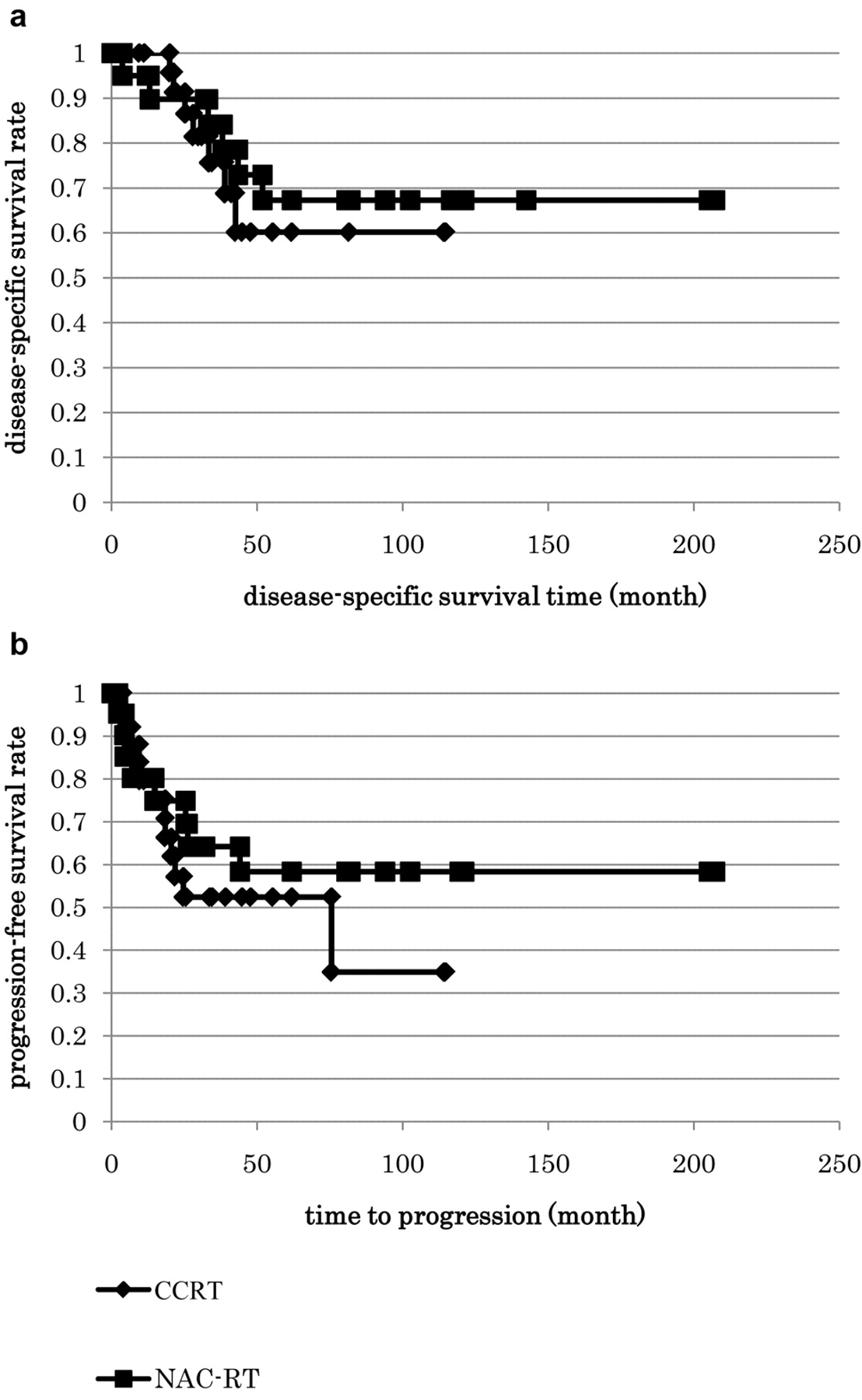
In the NAC-RT group, the 3-year and 5-year DSS were 84.1% and 67.3%, and the 3-year and 5-year PFS were 64.1% and 58.3%, respectively. There were no significant differences in DSS and PFS between the CCRT group and the NAC-RT group (Figure 3).
With regard to the stage I/II patients, the 5-year DSS was 72.9% in the CCRT group and 40% in the NAC-RT group (Figure 4A). Regarding the stage III/IV patients, the 5-year DSS was 49.5% in the CCRT group and 77.8% in the NAC-RT group (Figure 4B).
With regard to the cause of death in the two groups, locoregional failure rates were lower in the CCRT group (12%, 3/25) than in the NAC-RT group (19%, 4/21). In contrast, the number of patients who died of distant metastasis was slightly higher in the CCRT group (16%, 4/25) compared to the NAC-RT group (9.5%, 2/21).

Kaplan-Meier survival curves in months for patients given CCRT in comparison with NAC followed by RT.
Discussion
Combination treatments of RT with chemotherapy are classified as NAC followed by RT, CCRT, RT followed by adjuvant chemotherapy and alternating chemoradiotherapy. In 1998, Al-Sarraf et al. reported the superiority of CCRT followed by adjuvant chemotherapy over RT alone (1) with a significant advantage in 3-year overall survival for the patients treated with CCRT (76% vs. 46%, p<0.001). In addition, a decrease in both locoregional failure and distant metastasis was observed in the patients treated with CCRT. Moreover, some studies of NAC followed by RT or RT followed by adjuvant chemotherapy have been reported. However, the survival benefit of CCRT compared to RT alone has not been established (2-4).

Kaplan-Meier disease-specific survival curves in months for patients given CCRT in comparison with NAC followed by RT. (a) patients with Stage I/II (b) patients with stage III/IV.
In the present report, in the patients who received CCRT with the TPF or PFML regimen, the 5-year DSS and PFS were 60.1% and 52.4%, respectively. In comparison with former reports, these survival rates were encouraging. In particular, the TPF group showed a 5-year DSS was 75.0 %. But in contrast to our expectation, the survival rate improvement of CCRT in comparison to NAC followed by RT was not established. In particular, there was no survival rate advantage in advanced cases. In terms of outcome, the CCRT group showed less locoregional failure than the NAC-RT group (12% vs. 19%). Locoregional control seems to be improved by CCRT. In contrast, distant metastasis occurred more often in the CCRT group than in the NAC-RT group (16% vs. 9.5%). These results suggested that it is important to determine way to reduce the incidence of distant metastases in the patients with advanced stage receiving CCRT.
Recently, the use of NAC in head and neck cancer has been reevaluated in several reports (12, 13). For NPC, Hui et al. reported better 3-year overall survival and progression-free survival rates with NAC including docetaxel and cisplatin followed by CCRT (94.1%, 88.2%) than with CCRT alone (67.7%, 59.5%) (20). Bae et al. reported the efficacy and safety of NAC with TPF regimen followed by CCRT (21). Furthermore, Park et al. reported that in locally advanced NPC patients, CCRT followed by adjuvant chemotherapy with bleomycin, epirubicin and CDDP was effective and tolerable (22). On the basis of these previous studies and the results of present study, additional chemotherapy before or after CCRT for the purpose of controlling micrometastsis and decreasing distant metastasis may be important for survival rate improvement in patients with advanced NPC.
Conclusion
In comparison to the group receiving NAC-RT, CCRT had no advantage in terms of survival rates. In future, the control of distant metastasis by additional adjuvant chemotherapy before or after the initial treatment might play an important role in improving the survival rate of patients with advanced NPC receiving CCRT.
Footnotes
-
Conflict of Interest Notification
We have no conflict of interest.
- Received November 18, 2011.
- Revision received December 27, 2011.
- Accepted December 22, 2011.
- Copyright© 2012 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}
{kind=link}