


Abstract
Background: No reliable prognostic predictor is known for patients undergoing sorafenib treatment for advanced hepatocellular carcinoma (HCC). Patients and Methods: In 81 patients receiving sorafenib treatment for advanced HCC, we evaluated the prognostic significance of an inflammation-based prognostic score, the Glasgow prognostic score [evidenced by an elevated C-reactive protein level (>1.0 mg/dl) and hypoalbuminemia (<3.5 g/dl)] and compared it with Child-Pugh grade, Barcelona Clinic Liver Cancer staging system, Japan Integrated Staging (JIS) score, and the performance status by Cox-proportional analysis. Results: Median overall survival after sorafenib administration was 11.3 months. On multivariate analysis, Glasgow prognostic score (0 vs. 1 and 2; p<0.001), JIS score (1 and 2 vs. 3 and 4; p=0.001), and performance status (0 vs. 1; p=0.001) were found to be independently associated with survival. Conclusion: The Glasgow prognostic score has significant prognostic value in patients undergoing sorafenib treatment for advanced HCC.
Performance status is predictive of survival following systemic chemotherapies in patients with gastrointestinal cancer (1) and hepatocellular carcinoma (HCC) (2). The assessment of performance status is, however, subjective (3), and there is a growing need for the development of objective and reproducible prognostic scores. The Glasgow prognostic score, which assesses the presence of a systemic inflammatory response as evidenced by elevated C-reactive protein levels and hypoalbuminemia, has reliable prognostic value in patients with advanced gastrointestinal cancer (4), and was reported to be more useful than performance status for patients with various types of cancer (5, 6). However, no study has evaluated the prognostic value of the Glasgow prognostic score in patients with HCC, except for one study on postoperative mortality (7).
In the current study, we aimed to evaluate the prognostic value of the Glasgow prognostic score and compare it with established scoring systems, including the Child-Pugh grade, Barcelona Clinic Liver Cancer (BCLC) staging system (8), Japan Integrated Staging (JIS) score (9), and performance status for predicting survival of patients receiving treatment with sorafenib, recently approved as first-line chemotherapy for advanced HCC (10).
Patients and Methods
Patients with advanced HCC, for whom locoregional treatment was contraindicated, and who were admitted to a single institute between June 2009 and July 2011, were included in the study. Patients received treatment with orally administered sorafenib until either of the following criteria for discontinuation of therapy was met: drug-related adverse reactions that required termination of medication, and disease progression. The Glasgow prognostic score was constructed as described previously (5); patients with both an elevated C-reactive protein level (>1.0 mg/dl) and hypoalbuminemia (<3.5 g/dl) were allocated a score of 2; patients with one or neither of these biochemical abnormalities were allocated a score of 1 or 0, respectively. The BCLC staging system (8) and the JIS score (9) have been defined in detail previously. These scores were evaluated as predictors of survival and radiologic progression by the Kaplan–Meier method; the log-rank test was used to analyze differences. Multivariate analysis was carried out by the Cox-proportional hazard model. The Institutional Review Board approved the study protocol.
Results
The characteristics of the enrolled patients (n=81) receiving sorafenib for HCC are presented in Table I. The median age was 75 years, and the majority had a background of hepatitis C infection. The median follow-up duration of patients was 19 months, and during the follow-up period, 43 patients did not survive the cancer. Median overall survival and median time to radiologic progression after administration of sorafenib were 11.3 months [95% confidence interval (CI) 9.6-13.1] and 3.2 months (95% CI 2.5-3.8), respectively.
Demographical and baseline characteristics of 81 patients. Data are given as n (%) or median (range).
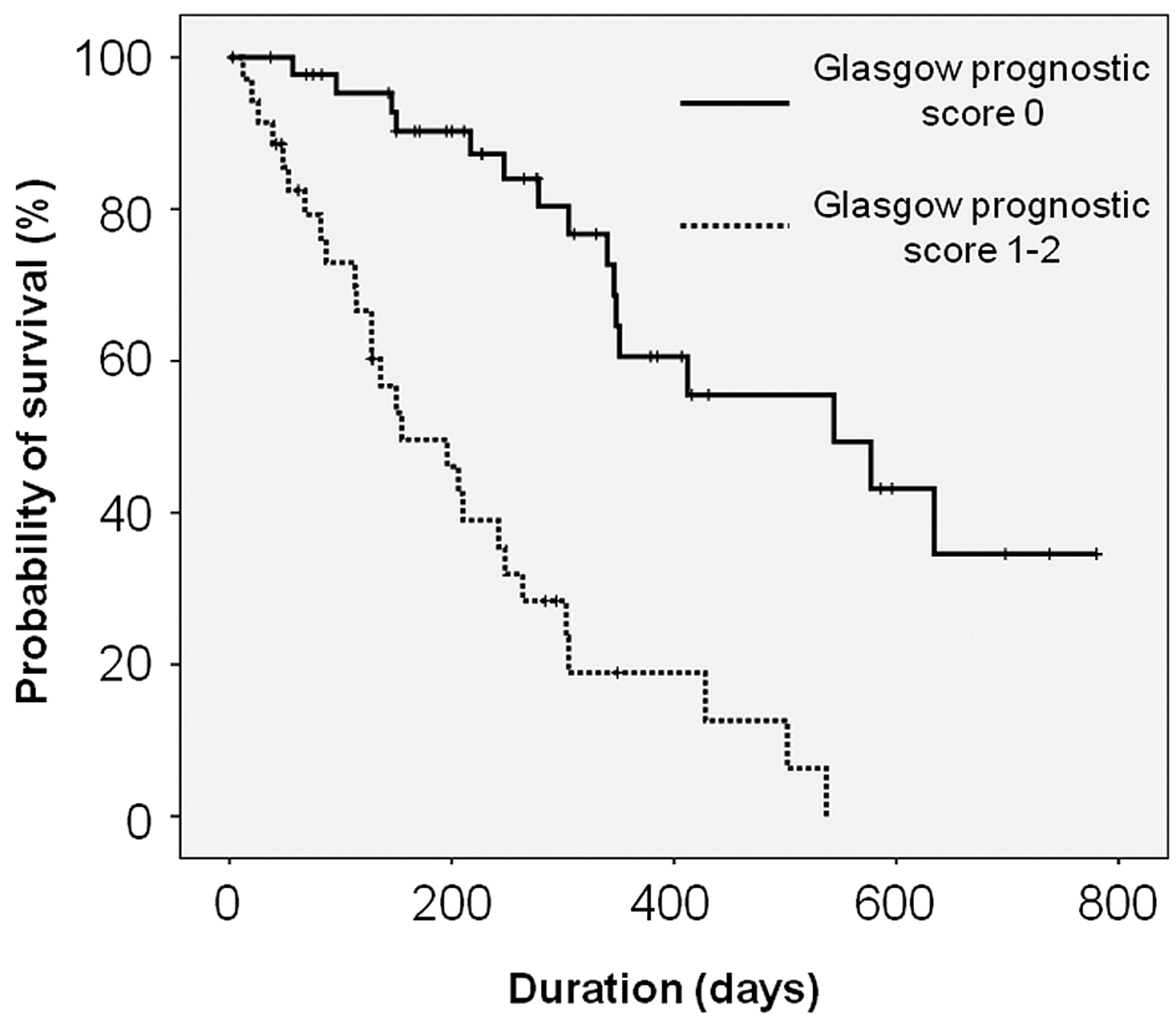
In univariate analysis, all the scores, including Child-Pugh grade, BCLC staging system, JIS score, Glasgow prognostic score, and ECOG performance status were found to be statistically significant indicators of survival (Child-Pugh grade: A vs. B, p=0.007; BCLC staging system: B vs. C, p<0.001; JIS score: 1 and 2 vs. 3 and 4, p<0.001; Glasgow prognostic score: 0 vs. 1 and 2, p<0.001; performance status: 0 vs. 1, p<0.001) (Table II, Figure 1). A multivariate analysis revealed that the following three scores were independently associated with survival: the JIS score [1 and 2 vs. 3 and 4; hazard ratio (HR) 10.042; 95% CI 2.638-38.228; p=0.001]; Glasgow prognostic score (0 vs. 1 and 2; HR 5.483; 95% CI 2.563-11.728; p<0.001); and ECOG performance status (0 vs. 1; HR 3.970; 95% CI 1.798-8.768; p=0.001) (Table II).
Child-Pugh grade, Glasgow prognostic score, ECOG performance status, and JIS score were found to be statistically significant indicators of radiologic progression in univariate analysis (Child-Pugh grade: A vs. B, p=0.001; Glasgow prognostic score: 0 vs. 1 and 2, p=0.004; performance status: 0 vs. 1, p=0.026; JIS score: 1 and 2 vs. 3 and 4, p=0.036) (Table III, Figure 2). However, in multivariate analysis, no indicators were found to be independently associated with radiologic progression (Table III).
Discussion
In this study, we found that the Glasgow prognostic score has significant prognostic value for patients undergoing sorafenib treatment for advanced HCC, independently of the JIS score and performance status.
Sorafenib has been reported to improve outcome for patients with advanced-stage HCC, and has therefore been established as a first-line treatment for these patients (8, 10). However, certain recent studies have reported surrogate markers for determining the treatment efficacy and prognosis in patients after sorafenib treatment for HCC. These studies investigated the early response of tumor markers (11) and radiological tumor response as evaluated by the response evaluation criteria in solid tumors (RECIST) (12), although these markers are not known at the commencement of the sorafenib treatment. The Glasgow prognostic score is a reliable prognostic marker following systemic chemotherapy in patients with cancer (4-6). The systemic inflammatory response predicts the progressive nutritional decline of patients (13) and is associated with increased toxicity in patients receiving chemotherapy (14). Recent reports indicated that the Glasgow prognostic score was more useful than performance status in patients with gastroesophageal cancer (6) and non-gatrointestinal cancer (5).
Univariate and multivariate analyses of survival.
Univariate and multivariate analyses of radiologic progression.
However, few reports have evaluated the prognostic value of the score for patients with HCC (7). Because of underling liver dysfunction, Ishizuka et al. proposed a modified Glasgow prognostic score in which the cutoff value for C-reactive protein is reduced from the original 1.0 mg/dl to 0.3 mg/dl for patients with HCC (7). Reduced liver dysfunction weakens the reaction of hepatocytes to interleukins induced by the host-versus-tumor interaction, including up-regulation of C-reactive protein synthesis in the liver (15, 16). The results of multivariate analysis in the current study, however, indicated that both the original and the modified Glasgow prognostic scores provided significant prognostic value, independently of JIS score and the performance status (data not shown).

Overall survival of the patients according to Glasgow prognostic score (score 0 vs. 1 and 2, p<0.001).
Univariate analysis in the current study indicated that both the BCLC staging system and JIS score had significant prognostic value for patients under sorafenib treatment. These scoring systems, encompassing both tumor burden and liver function, were revealed to have potential predictive value for survival of patients with advanced HCC, although no reliable systemic chemotherapies that improve survival had been considered when these scoring systems were first implemented (8, 9). Interestingly, multivariate analysis in this study indicated that the Glasgow prognostic score functioned independently in the prognostic prediction of the JIS score, which considered both tumor burden and liver function.
The Glasgow prognostic score is, from another viewpoint, one of the clinical markers indicative of cancer-related cachexia, including lean body mass, resting energy expenditure, and performance status (17). Thus, in patients with cancer-related cachexia, a systemic inflammation-based scoring system provides a prognostic value which is independent of the tumor stage (18) and is superior to the one of performance status (5). Patients with advanced-stage HCC often experience cancer-related cachexia, and the Glasgow prognostic score might thus add useful prognostic value for such patients.
To our knowledge, this is the first report evaluating the prognostic values of various scoring systems for patients receiving sorafenib treatment for advanced HCC. We conclude that the Glasgow prognostic score has great potential clinical utility, exceeding the one of the JIS score and performance status, because this scoring system consists of two simple, objective, and reproducible parameters. However, the current study was retrospective and comprised a relatively small number of patients. We have also not clarified any interaction between the systemic inflammatory reaction and response to sorafenib. Thus, this interaction should be evaluated thoroughly in further studies. Nevertheless, our study contributes to the current drive to identify biomarkers that may aid the selection of appropriate patients for various systemic chemotherapies in order to improve the outcome of advanced HCC.

Radiologic progression of the patients according to Glasgow prognostic score (score 0 vs. 1 and 2, p=0.004).
Footnotes
-
This article is freely accessible online.
- Received November 17, 2011.
- Revision received December 18, 2011.
- Accepted December 21, 2011.
- Copyright© 2012 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}