


Abstract
Background: Oral metronomic chemotherapy is a therapeutic option which is particularly attractive due to its ease of administration and low toxic burden. Its mechanism of action probably involves antiangiogenetic effect rather than a classical antiproliferative effect like standard maximally tolerated dose-based regimens. Patients and Methods: A retrospective analysis of 61 patients with advanced breast carcinoma was carried out with the aim of reporting activity in terms of response rate, control of tumor-related symptoms, outcome, and toxicity. All patients had hormonal therapy-resistant metastatic disease and had previously received two lines of chemotherapy. The first cohort of 22 patients received oral cyclophosphamide at 50 mg/day without interruption until re-evaluation or progressive disease, while the second cohort of 39 patients had oral cyclophosphamide at the above dose plus oral low-dose methotrexate at 2.5 mg orally twice a week. Results: Overall, a partial response with a median duration of 6 months (range 4-9 months) according to the RECIST criteria was recorded in 18% of patients (95% confidence intervals, CI=8%-28%), and stable disease with a median duration of 5 months (range 3-8 months) was recorded in 35% of cases (95% CI=22%-49%) for a tumor growth control rate of 52%. Symptom control was achieved in 54% of cases. Toxicity was very mild and easily manageable. No cases of extra-hematological grade 3 toxicity were observed. Grade 3 non-febrile neutropenia were recorded in 3% of cases. Liver toxicity was represented by elevation of transaminases in 20 cases (33%), mainly in the cohort of patients receiving cyclophosphamide plus methotrexate. Conclusion: Although retrospectively recorded, the data presented in this study support the use of oral metronomic chemotherapy for patients with metastatic breast cancer. Significant clinical activity was seen in heavily pretreated patients without severe grade 3-4 side-effects. Further studies are warranted to optimise the treatment schedule and to select patients who may benefit from such an approach.
To date salvage therapy for advanced breast cancer (ABC) still represents a daily problem due to the improved median survival time and the frequent use of multiple lines of therapy. In this palliative clinical setting, the management of prolonged treatments represents another challenge since the major goals of any chemotherapeutic treatment include the best possible control of cancer-related symptoms, the prevention of serious cancer-related complications, and, hopefully, an increase in survival while maintaining the patients' quality of life (1). Despite these efforts, severe side-effects related to intravenous full-dose chemotherapy may outweigh its potential clinical benefits, negatively influencing quality of life, especially in patients receiving multiple line therapies.
Recently the administration of chemotherapy for prolonged periods of time at relatively low, non-toxic doses without long rest intervals – so called metronomic chemotherapy – has received considerable attention by many oncologists (2, 3). In fact, a metronomic approach has many potential advantages, such as the oral use of newer or old chemotherapeutic drugs, the relative ease of administration, the low rate of severe toxicity, the delivery of a dose-dense but not necessarily dose-intense treatment and the reduction in burden to both patients and their families. Moreover, a patient preference for oral treatment has been repeatedly reported in medical literature (4).
Experimental investigations have suggested that metronomic chemotherapy seems to work more via the inhibition of the proliferation of endothelial cells of the tumor vascular system rather than via the direct killing of proliferating neoplastic cells as classic antiproliferative treatment (2, 3, 5-9). Cyclophosphamide represents one of the older drugs used in oncology, mainly by intravenous route, even if it has been also successfully employed orally (10). Cyclophosphamide has generally been administered at a higher dose intensity when given orally compared with intravenous infusion (10, 11). Although oral administration presents the advantage of an easier and safer utilization with few side-effects, however, the administration of oral cyclophosphamide may raise challenges different from those related to conventional maximum-tolerated dose, intravenous chemotherapy. These include possible altered pharmacokinetic characteristics due to long-term drug exposure potentially resulting in acquired resistance, and an increased risk of unfavorable drug interactions especially when compounds that are metabolized by cytochrome P3A4 are co-administered with low dose metronomic chemotherapy (12). However, in some experimental trials oral cyclophosphamide has been safely employed in combination with low-dose oral methotrexate with significant results in terms of cancer palliation (13-15).
In this article we report a retrospective analysis on the efficacy and safety of oral cyclophosphamide with and without oral methotrexate in a series of patients with ABC pre-treated with intravenous chemotherapy.
Patients and Methods
Study design. After communication with the Ethical Committee of participating institutions, this retrospective study included pretreated patients with ABC progression after several lines of hormonal treatment and chemotherapy. Data were retrospectively collected and only records with complete data were considered for the clinical analysis. The main study endpoints were to report activity in terms of response rate, time-to-progression (TTP) and safety of oral metronomic single-agent cyclophosphamide and its combination with methotrexate.
Selection criteria. Patients included in the study were required to have histologically confirmed ABC resistant to hormonal therapy and progressing after systemic chemotherapy, measurable disease according to the RECIST criteria (16); life-expectancy >3 months; Eastern Cooperative Oncology Group (ECOG) performance status ≤2; adequate bone marrow reserve defined as white blood cells ≥4,000/ml and platelets ≥100,000/ml, and adequate renal (serum creatinine ≤1.2 mg%, blood urea nitrogen <60 mg%) and hepatic (total serum bilirubin ≤1.5 mg%, transaminase values within two times the normal limit function; absence of cerebral or leptomeningeal involvement; no history of nephritic syndrome or arterial thromboembolic events; absence of severe uncontrolled cardiovascular or gastrointestinal diseases. Patients were excluded if their medical history was positive for cancer other than breast carcinoma, with the exception of non-melanotic skin tumors, or uncontrolled non-neoplastic diseases. Radiotherapy for advanced disease was allowed. Each patient gave a written informed consent to receive oral chemotherapy.
Disease staging and symptoms recording. Initial work-up included clinical and radiological evaluation of the metastatic target and non-target lesions, hematological plus renal and liver tests. Patients were staged with physical examination, serum chemistry tests, complete blood counts, chest x-rays, abdominal sonogram, computed tomography scan, bone scan. Other examinations were employed as needed. Patients were routinely interviewed for their main symptoms, which were graded according to a standard visual analogue scale ranging from 0 (none) to 10 (worst).
Treatment plan. Cyclophosphamide was used orally at the dose of 50 mg/day continuously for 22 patients (cohort 1), and in association with methotrexate at 2.5 mg orally twice weekly (Monday and Thursday). No antiemetic treatment was routinely given to patients. However, if clinically relevant nausea/vomiting occurred, the caring physician employed oral metoclopramide, dexamethasone or even an anti-HT3 drug depending on the severity of symptoms. Any prior hormonal therapy had to be stopped at least one week before the beginning of oral metronomic chemotherapy. Serum chemistry tests and blood counts were repeated every three weeks to monitor potential toxicity. Patients were seen by their treating physician every four weeks.
Evaluation of response and survival parameters evaluation. Patients were evaluated for objective response after three months of chemotherapy, unless an individual patient's clinical conditions suggested early re-evaluation. Objective responses were recorded according to the RECIST criteria and results were reported as best overall response (16). Briefly, complete response (CR) was defined as the complete disappearance of all measurable target lesions and also evaluable ones without the appearance of new lesions determined by two consecutive observations not less than four weeks apart; partial response (PR) was defined as at least a 30% decrease in the sum of the longest diameter of target lesions, taking as reference the baseline sum of the longest diameter with no progression of evaluable lesions; progressive disease (PD) was at least a 20% increase in the sum of the longest diameter of target lesions, taking as reference the smallest sum of the longest diameter recorded since the treatment started or the appearance of one or more new lesions; and stable disease (SD) as neither sufficient shrinkage to qualify for PR nor sufficient increase to qualify for PD with no progression of target lesions, using as reference the smallest sum of the longest diameter since the treatment started. The sum of CR and PR was defined as the overall response rate (ORR). The sum of ORR and SD was defined as the tumor growth control rate (TGCR). Results were also reported according to an intent-to-treat fashion. Therefore early deaths, patients with severe drop in performance status, those with clinically progressive disease before re-evaluation, and patients who dropped out due to severe toxicity were all considered as treatment failures, and were included in the treatment failure group. TTP was calculated from the date of starting oral treatment until the date when progression was documented. Survival was calculated from the screening date until death or the last follow-up date.
Toxicity evaluation. Evaluation of tolerance and side-effects was carried out according to National Cancer Institute Common Toxicity Criteria (NCI CTC) version 2.0 criteria (16) by clinical and laboratory investigations. Dose modifications were performed in a very flexible way depending on the type, severity and duration of side-effects. Treatment was withheld for one week in cases of a neutrophil count <1,000/ml and/or platelet count <75,000/ml. A 50% dose reduction in the total amount of drug administered in each cycle was prescribed after hematological recovery. In the case of a neutrophil count <1500 but >1,000/ml and/or platelet count <100,000 but >75,000/ml, therapy was administered with a 50% dose reduction in the total amount of drug administered in each cycle. Re-escalation of drug doses was attempted if close monitoring was possible. Oral therapy was withheld until recovery in case of grade 2 anorexia, nausea, vomiting, diarrhea, stomatitis, and dryness of the mouth, epigastric pain or increase in bilirubin or transaminases. The drug dose was reduced by 25% reduction of cyclophosphamide for the following week subsequently trying to increase drugs to full dosage if tolerated. Any other non-hematological grade 3 toxicity was managed by a 50% reduction of dosage for the subsequent administrations.
Statistics and dose-intensity. Objective tumor responses were reported as relative rates with 95% confidence intervals (95% CI). Differences in clinical data and response were analyzed by applying a Fisher's exact test to a contingency table. Rates were generally approximated to the nearest unit. TTP and overall survival (OS) were analyzed according to the Kaplan-Meier product-limit analysis employing the computer statistical software Prism (Graph Pad Incorporated, San Diego, CA, USA). Statistical analysis employed the log rank test reporting the p-value and hazard ratio (HR). Calculation of dose intensity was carried out according to Hryniuk (17) and the Wilcoxon rank sum test was employed for evaluation of differences in delivered dose intensity. Since patients received a fixed dose of oral cyclophosphamide independently of body weight and height, the planned dose intensity was theoretically calculated for a patient with a body surface area of 1.7 m2 and was found to be 220 mg/m2/week. Similarly methotrexate planned dose intensity was 3 mg/m2/week.
Results
Patient population. Table I depicts the main demographic and clinical characteristics of all enrolled patients and according to treatment employed. Overall, 61 patients with histologically confirmed, measurable ABC were considered eligible for the study out of 100 patients screened for complete data. Twenty-two patients received single-agent cyclophosphamide and 39 patients its combination with methotrexate. The median age was 68 years, ranging from 39 to 81 years and the median ECOG performance status was 1 (range 0-2). Only eight patients (13%) had a performance status of 2. Sites of disease included liver, lung, pleura, breast, soft-tissue and bone. Osseous, visceral and soft-tissue lesions each represented dominant disease in nearly one third of cases. All cases had multiple metastases. The main basal subjective symptoms included dyspnea, pain, cough, and fatigue.
Table II shows previous treatments received by patients. Briefly, 87% of patients had prior adjuvant medical treatment either hormonal or chemotherapy. Depending on menopausal status tamoxifen plus luteinizing hormone-releasing hormone analogue or an aromatase inhibitor (anastrazole or letrozole) were employed as adjuvant hormonal therapy. Adjuvant chemotherapy included: 5-fluorouracil (600 mg/m2), epirubicin (75 mg/m2), and cyclophosphamide (600 mg/m2; FEC); cyclophosphamide (600 mg/m2), methotrexate (40 mg/m2), and 5-fluorouracil (600 mg/m2; CMF); epirubicin (75 mg/m2) and cyclophosphamide (500 mg/m2; EC); or FEC followed by taxotere (75-100 mg/m2). The vast majority of patients were tumor positive for positive hormonal receptors and had previously received two hormonal therapy lines. Most cases (93%) had received two lines of chemotherapy before receiving oral chemotherapy. Fifty-four percent of patients had previously received an anthracycline-based regimen, 51% of patients a taxane-based treatment, 67% of cases vinorelbine, and 28% an oral therapy with capecitabine. All patients had PD at the beginning of oral treatment. No statistically significant differences in clinical data were found between the two cohorts of patients.
Patients' demographic and clinical characteristics.
Previous treatments.
Objective response and symptoms control. Table III shows the results in terms of objective response and survival data. No CR was observed. Overall, 11 patients had a PR (18%; 95% CI=8%-28%) and 21 patients showed SD (34%; 95% CI=22%-49%), for a TGCR of 52% (95% CI=41%-67%). The remaining 39 patients experienced progressive disease. The median duration of PR and SD were 6 months (range 4-9 months) and 5 months (range 3-8 months) respectively. As presented in Table III, the PR rate was higher in the cohort of patients treated with the combined therapy (20%; 95% CI=7%-37%) as compared to the one recorded in patients treated with single-agent cyclophosphamide (14%; 95% CI=0-28%). This difference was not statistically significant (p=0.45). The SD rate was 31% (95% CI=16%-46%) and 41% (95% CI=20%-62%), and TGCR was 51% (95%CI 35%-67%) and 55% (95%CI 34%-76%) in the cohort treated with the combination therapy and in the one treated with single-agent cyclophosphamide respectively. These differences were not statistically significant. The variability of objective responses is shown in Figures 1 and 2. The PR rate observed was significantly lower for patients with liver metastases (n=26) when compared with patients (n=35) with other sites of disease (3.8% versus 28.6%; p=0.0173, Fisher's exact test). Moreover patients with nodal disease (n=31) had a significantly higher ORR than patients (n=30) without nodal disease (29% versus 6.7%; p=0.0426, Fisher's exact test). No other correlation existed between the type of response and other sites of disease. Overall, 54% of patients who completed the interviews reported an improvement in basal symptoms.
Objective responses and survival parameters.
TTP and survival outcomes. Overall, the median TTP was estimated to be 4.2 months (range 2-11 months) and the 6-month progression-free rate was estimated to be 14% (95% CI=5%-23%). The median OS time was estimated to be 13.8 months (range 4.0-26+ months) and the survival rate at 2.0 years was estimated to be 20.0% (95% CI=10%-30%). The differences in survival parameters between the two cohorts of patients were not statistically significant. In the whole series the presence of liver metastasis was significantly associated with worse PFS (HR=1.33; log-rank p=0.042) and OS (HR=1.91; log-rank p=0.045). At the last data update, six patients were alive but all with progressed disease, but with one who is disease-responsive after 26 months of oral ciclophosphamide plus methotrexate administration. One patient died of stroke without cancer progression, and other one of disease-unrelated bone fracture, and the remaining patients died of cancer progression.
Toxicity data and dose-intensity. The median duration of oral treatment was 4.2 months. At the time of this report, all patients but one, have discontinued treatment because of progression of disease. Toxicity data are available for all patients. As shown in Table IV severe toxicities related to oral chemotherapy, i.e. ≥grade 3-4 side-effects were extremely infrequent. Transient and non-febrile grade 3 leukopenia was recorded in two cases (3%), grade 1-2 thrombocytopenia was observed in seven (12%) and one patient had grade 3 platelet decrease (2%). Fifteen patients (25%) complained of moderate grade 1-2 nausea, which was easily controlled with the use of oral metoclopramide in most cases but 3 cases required the addition of oral dexamethasone. Mild epigastric pain was reported in four patients (7%). Four patients (7%) presented signs of mild urinary bladder inflammation without bacterial growth, which was treated with hydration by mouth and short-term anti-inflammatory drugs. Liver toxicity was represented by elevation of transaminases in 20 cases (33%), mainly in the cohort of patients receiving the combination therapy. Accordingly to the theoretical planned dose intensity, the median, actually delivered dose intensity of oral cyclophosphamide and methotrexate was 96% and 90% of the planned dose intensity, respectively. The main reasons for reduction in dose intensity were liver and hematological toxicity.
Discussion
Oral chemotherapy is an attractive option for both patients and medical oncologists because of its great ease of administration and convenience compared to intravenous chemotherapy (18-20). Liu et al. (4) reported that nearly 90% of cancer patients treated outside a clinical trial setting expressed a preference for oral chemotherapy, provided that the efficacy and toxicity of these agents were comparable to those of their intravenous counterparts. From a patient's perspective, oral agents would make a significant contribution to their quality of life. In fact, patients receiving oral chemotherapy at home have been found to have a better quality of life than those receiving treatment in the hospital (18-20). Moreover patients at home have been found to be more active, to require less analgesia, and to experience fewer psychosocial or gastrointestinal side-effects.
Cyclophosphamide and methotrexate were among the first chemotherapeutic agents available in oral formulations for the management of ABC and other neoplastic diseases (21, 22). Since then, other oral cytotoxic agents have been developed, including the fluoropyrimidine capecitabine and the vinca alkaloid vinorelbine, which are widely employed for the management of ABC patients (23, 24). These drugs have also been employed in all oral combinations according to the possible antiangiogenic activity of metronomic scheduling (13, 14, 25-27).
In this article we report our experience with low-dose, continuous chemotherapy with daily cyclophosphamide with and without twice weekly oral methotrexate in a series of 61 patients with ABC resistant to hormonal therapy and chemotherapy. A cohort of 22 patients was treated with single-agent cyclophosphamide and a second larger cohort (n=39) with the combination of cyclophosphamide plus methotrexate according to a schedule previously described by investigators at the European Institute of Oncology in Milan, Italy (13). The intermittent schedule of methotrexate was successfully designed in order to reduce expected liver toxicity. The clinical interest in metronomic scheduling of chemotherapy is further strengthened by the recent publication of phase II trials on metronomic chemotherapy plus other anti-angiogenic agents, such as thalidomide, and bevacizumab (14,27-29).
Side-effects experienced accordingly to therapy received.
In our retrospective series oral single-agent cyclophosphamide and the combination of cyclophosphamide and methotrexate resulted fairly active and very well tolerated, since severe grade 3-4 toxicities were only occasionally reported in a minority of cases. Occasional grade 3 toxicity, mainly leukopenia and thrombocytopenia, were observed more frequently in the cohort of patients treated with the combination than in that receiving cyclophosphamide alone. The addition of low-dose, twice-weekly methotrexate to daily cyclophosphamide resulted in a slight increase in liver toxicity, mainly represented by mild and transitory transaminase increases, which however were generally easily managed with dose reduction, with or without temporary dose interruption. In our experience, tri-weekly monitoring of serum chemistry tests and blood counts is strongly advisable to accurately monitor possible side-effects.

Waterfall plot of objective responses in the cohort of patients treated with oral single-agent cyclophosphamide accordingly to individual changes in the size of target lesions at baseline.
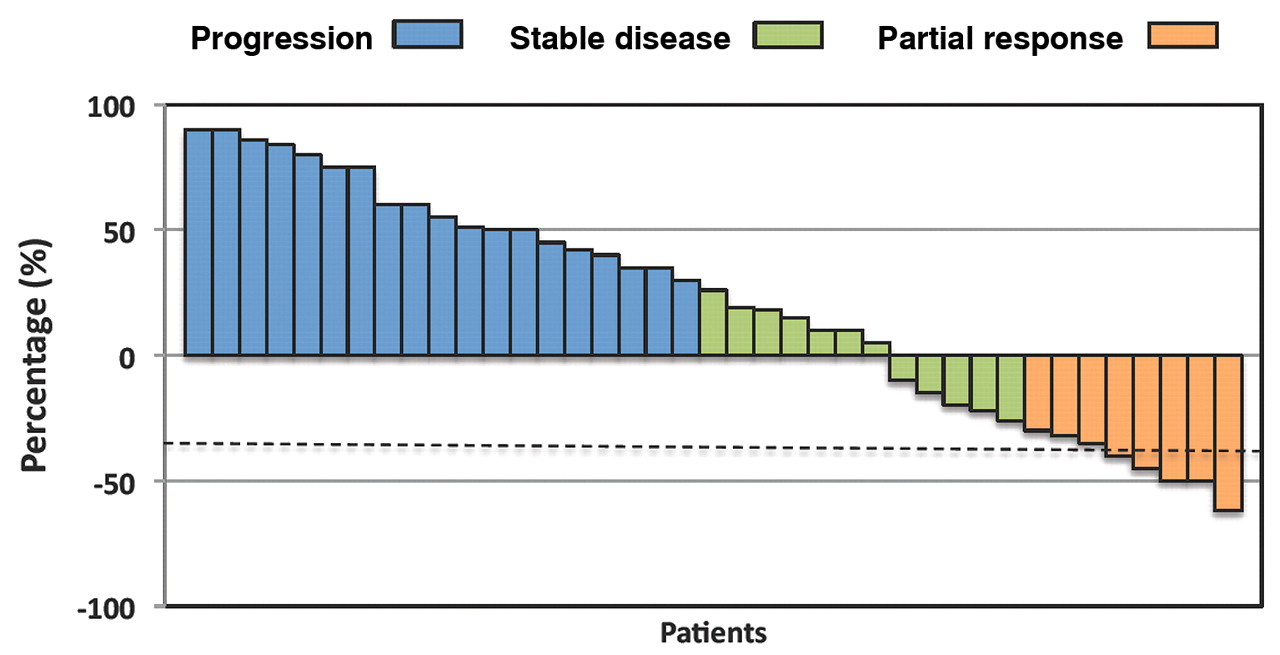
Waterfall plot of objective responses in the cohort of patients treated with oral cyclophosphamide plus methotrexate accordingly to individual changes in the size of target lesions at baseline.
Overall a PR was recorded in 18% of patients and SD in 34% of cases, for a TGCR of 52%. Therefore almost one half of patients experienced absence of cancer progression, SD being a reasonable clinical endpoint in such a clinical setting. The PR rate was somewhat higher in the cohort of patients treated with the combination as compared to that treated with cyclophosphamide alone (20% versus 14%), but this difference was not statistically significant (p=0.45). Moreover, the TGCRs were almost superimposable in the two cohorts. Patients without liver metastases and with nodal disease showed the highest response rate. The median TTP and OS were not significantly different between the two cohorts of patients. The presence of liver metastases was associated with a worse outcome both in terms of objective response and survival parameters, while the presence of soft tissue disease was associated to a better outcome. These data suggest that the prescription of oral metronomic chemotherapy may be more appropriate for patients without visceral dominant disease. Overall, our data confirm the activity and safety of oral metronomic chemotherapy, with cyclophosphamide with or without methotrexate, being response rate and survival parameters in the range reported in medical literature by other authors (13, 14, 27-29).
In conclusion the above-reported data suggest that oral metronomic cyclophosphamide may be useful in the palliative treatment of patients with ABC, pending careful selection of cases. Patients without dramatic visceral progression, patients of advanced age, those with dominant soft tissue and/or bone disease and with hormone receptor positive disease, are probably the best candidates for oral metronomic chemotherapy. Further studies are required to optimize oral treatment of ABC and better select patients likely to benefit from this therapeutic approach.
Acknowledgements
This work was supported by the GSTU Foundation, Palermo for data management and editorial fees.
Footnotes
-
Author's Contribution
VG conceived the study, managed data, carried out statistical analysis, and coordinated the study; HB collected and managed required data; MRV collected required data and participated in writing the paper. All Authors read and approved the manuscript.
-
Competing Interests
The Authors declare they have no competing interests.
- Received November 26, 2011.
- Revision received December 17, 2011.
- Accepted December 21, 2011.
- Copyright© 2012 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.