


Abstract
Background: Although high-dose chemotherapy (HDC) represents the standard of treatment for high-risk neuroblastoma (NBL), the most effective conditioning regimen still remains to be identified. Patients and Methods: Forty-one high-risk NBL entered into local protocol based on induction chemotherapy, surgery and HDC with either etoposide/thiotepa/cyclophophamide (ETC) or i.v. busulfan and L-PAM (Bu/L-PAM). Results: Thirty-seven patients underwent HDC; 29 with ETC and 8 with Bu/L-PAM. No toxic deaths were recorded. The 5-year progression-free survival (PFS) of patients given ETC was 21% (95% confidence interval CI (9-36%), while PFS for patients given Bu/L-PAM was 88% (95% CI=39-98%) (p<0.05). In multivariate analysis, treatment with the ETC regimen predicted progression/recurrence with a hazard ratio (HR) of 16.8 (p<0.05), as well as MYCN amplification which had an HR of 4.4 (p<0.05). Conclusion: Although the number of studied cases is limited, our data suggest that in high-risk NBL the combination of Bu/L-PAM is superior to the ETC regimen.
Children with high-risk neuroblastoma (NBL) have dismal outcome despite intensive multimodal treatment, with the 3-year event-free survival (EFS) being lower than 40% (1-6). The use of myeloablative cytotoxic therapy with autologous bone marrow transplantation (ABMT) and/or peripheral blood stem cell (PBSC) rescue represents a standard treatment for high-risk NBL patients. However, the best conditioning regimen, both in term, of survival and acute and late toxicities, has not been yet identified (1, 7). Different conditioning regimens have been proposed based mainly on carboplatin, etoposide, cyclophosphamide, melphalan (L-PAM) and busulfan, with or without total-body irradiation (TBI), as originally reported in the COG3891 study (2-5, 6-11). Currently, the Children Oncology Group (COG) standard regimen is carboplatin, etoposide and L-PAM (CEM) (7). The use of TBI in these young patients is controversial because of the long-term side-effects (12, 13); moreover, the benefit of a TBI-containing regimen has not been evaluated in a randomized study, while in a retrospective study the probability of survival was comparable to that obtained using high-dose chemotherapy alone (14). Some studies suggested that the busulfan-based conditioning regimen provides better results, in terms of survival (14-16). These studies were not prospectively randomized and selection bias may have influenced the results. One of the main objectives of the ongoing International Society Pediatric Oncology (SIOP) Europe Neuroblastoma Protocol is to compare, in a randomized way, 2 different conditioning regimens including busulfan and L-PAM (Bu/L-PAM) and CEM.
In 2001, we opened a single-institution pilot study for patients with newly-diagnosed high-risk NBL. The induction phase was based on four cycles including topotecan, cyclophosphamide, ifosfamide, carboplatin and etoposide. After a post-operative course, patients who achieved at least partial response received high-dose chemotherapy followed by radiotherapy on the primary tumor and cis-retinoic acid for one year (17). The conditioning regimen was based on etoposide, thiotepa and cyclophosphamide (ETC) in the first phase and on Bu/L-PAM in the second phase. In this study, we report the impact of these two different conditioning regimens on the patients' outcome.
Patients' characteristics.
Patients and Methods
Patients. Patients over one year of age, with either metastatic or localized MYCN-amplified tumor, were classified as having high-risk disease and were enrolled in the study from April 2001 to July 2009. The protocol was approved by the Institutional Review Board. Informed consent was obtained from patients' parents or their legal guardians. Patients' characteristics are summarized in Table I.
MYCN copy number was evaluated on tumor samples following current guidelines (18). Diagnosis, staging and response were performed according to the International Neuroblastoma Diagnosis and Staging Criteria (19).
Treatment. The protocol included four courses of chemotherapy, as previously reported (17). Surgery was planned after the fourth course. HDC, followed by autologous stem cell rescue, was performed in all patients achieving at least partial response according to the Criteria of Brodeur et al. (19). Two different conditioning regimens were employed: the first conditioning regimen consisted of a combination of etoposide at 600 mg/m2, thiotepa at 750 mg/m2 and cyclophosphamide at 120 mg/kg (ETC regimen), while the second was based on i.v. busulfan at 0,8-1,2 mg/kg/dose for 16 consecutive doses over 4 days plus L-PAM at 140 mg/m2 in single-dose (Bu/L-PAM regimen). Until December 2007, the ETC conditioning was used, while children receiving transplants after January 2008 were given the Bu/L-PAM conditioning regimen.
As previously reported (17), the proposed induction regimen achieved a satisfactory response rate before consolidation. Nevertheless, the survival was dismal. The Bu/L-PAM regimen was introduced to improve the survival.
Hyperfractionated radiotherapy (21 Gy in two daily fractions 1.5-Gy, six hours apart, for 6 consecutive days/week) was delivered to the primary tumor bed (20). Subsequently, 13-cis-retinoic acid was administered orally for 12 months at a dosage of 160 mg/m2/day for 14 consecutive days and repeated every 28 days (2).
Evaluation of toxicity. Toxicity was evaluated according to the criteria of Bearman et al. (21). The Common Toxicity Criteria for Adverse Event (CTCAE) version 4 (22) was used to report the toxicities not considered in (21) (skin and tubular toxicities in this report).
Haematological toxicity. The median time from transplant to neutrophil and platelet recovery in days (range). ETC, etoposide/thiotepa/cyclophosphamide; Bu/L-PAM, busulfan/melphalan.
Statistical analysis. Overall survival (OS) was defined as the time interval between the date of diagnosis and the date of death from any cause or the date of last follow-up. Progression-free survival (PFS) was defined as the time interval between the date of diagnosis and the date of first relapse/progression, the date of death, whichever occurred first, or the date of last follow-up. The Kaplan–Meier method was used for the estimation of survival curves (23), while the log-rank test was used to compare differences between groups.
Multivariate analyses were performed using Cox proportional hazards regression model for PFS and OS. Variables that reached a p-value of 0.20 in univariate analysis were included in the initial model and variables were eliminated one at a time, in a stepwise fashion, to keep only variables that reached a p-value of 0.05 or less into the final models. All p-values were two-sided, with a type I error rate fixed at 0.05. Variables considered as potential prognostic factors for PFS and OS were age (considered as >2 years or <2 years), site of primary tumors, presence of metastasis, site of metastasis, MYCN status (MYCN amplified versus MYCN non-amplified or MYCN-gain), conditioning regimen (Bu/L-PAM versus ETC) and response at the end of induction. Analyses were performed using the Stata 9.0 statistical software package (StatCorp LP, TX, USA).
Results
Forty-one consecutive children, over one year of age, with either metastatic (38 patients) or localized MYCN-amplified tumor (three patients) were enrolled in the study.
At the end of induction and before HDC 40 patients were evaluable for response (one patient died after surgery due to acute renal failure): 5/40 (12.5%) patients presented progressive disease (PD), 14/40 (35%) were in partial response (PR) and 21/40 (52.5%) achieved either complete response (CR) or very good partial response (VGPR).
Thirty-seven patients underwent HDC; 29 underwent the ETC regimen and 8 the Bu/L-PAM. Out of five patients with PD, two patients underwent HDC as salvage treatment; in both cases the ETC regimen was given before transplantation. These cases were included in the analysis of the conditioning regimen toxicity.
The median time interval between the first course and HDC was 218 days (range=169-280 days): it was 215 days (range=177-280 days) for children given Bu/L-PAM and 218 days (range 169-280 days) for those treated with ETC. The median time to reach neutrophil and platelet recovery is shown in Table II. There was a statistically significant difference in the median time from transplantation to platelet recovery.
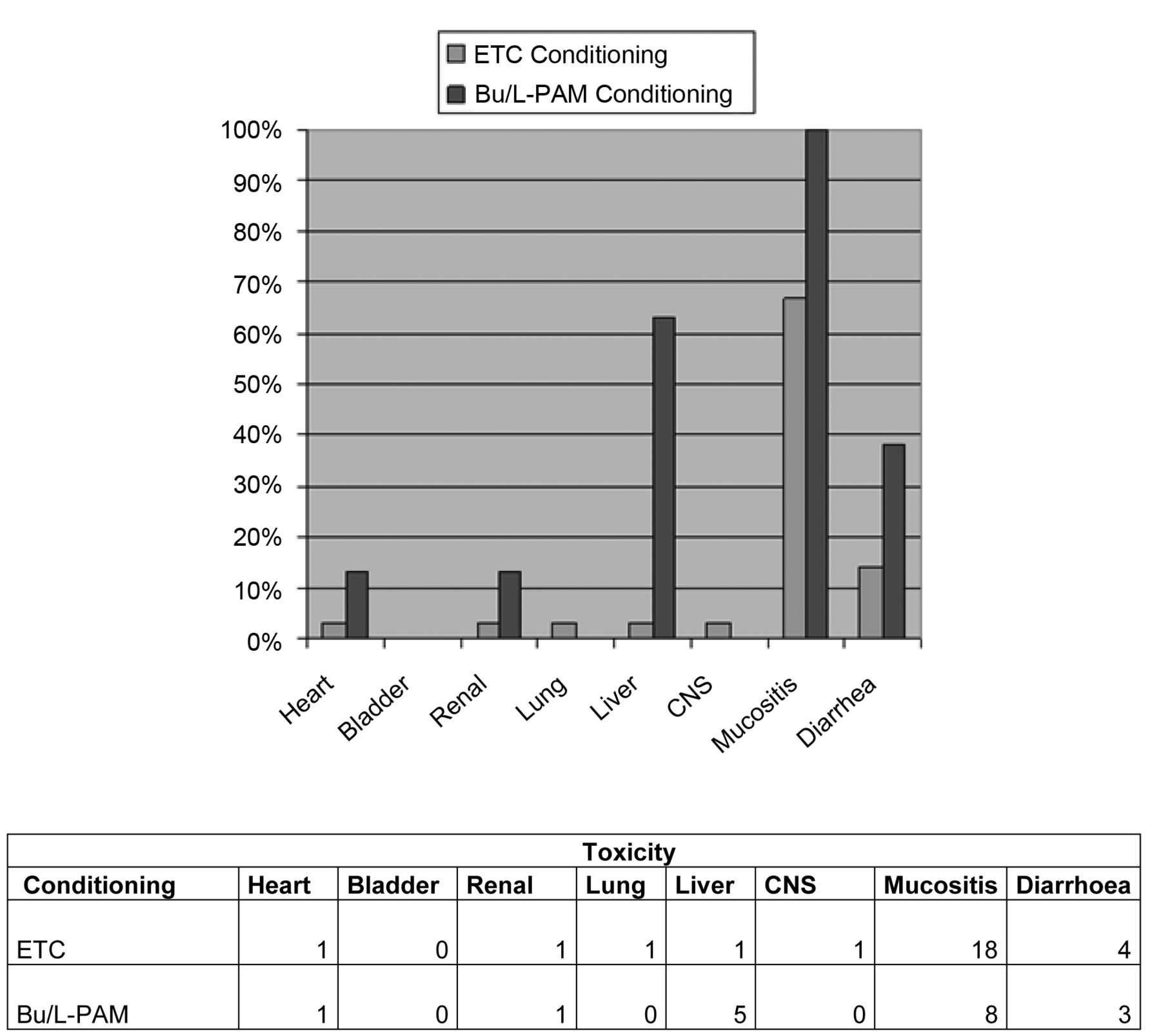
Toxicities of the two different conditioning regimens. The table shows the number of events and the figure the percentage, according to the two groups and the toxicities. ETC, Etoposide/thiotepa/cyclophosphamide; Bu/L-PAM, busulfan/melphalan; CR, complete response; CNS, central nervous system.
Figure 1 reports the major toxicities according to the type of conditioning regimen. No toxic death was recorded after transplantation. Extra-hematological toxicity was mainly gastrointestinal. Using the citeria of Bearman et al., five patients presented grade 1 stomatitis, while 18 patients grade 2 and 3 patients grade 3 stomatitis, respectively. Diarrhea was recorded in seven patients: it was of grade 1/2 in four patients and of grade 3 in three others. Liver toxicity was reported in six patients: grade 1 in three patients and grade 2/3 in the other three patients; in five out of six cases, all treated with the Bu/L-PAM regimen- the liver impairment was due to reversible hepatic veno-occlusive disease. Only one patient (given the ETC conditioning) presented grade 3 lung toxicity, according to the criteria of Bearman et al. Sepsis was documented in four patients. One patient presented grade 1 tubular toxicity, based on the CTCAE, while grade 1/2 skin toxicity according to CTCAE was reported in three patients. Primary graft failures were reported in two patients, one for each conditioning regimen; in both patients the post-transplantation phase was complicated by sepsis and sepsis plus an hepatic veno-occlusive disease in the latter patient. Figure 1 presents toxicities according to the different conditioning groups.
Univariate analysis of factors predictive for outcome. All analyzed factors are presented with progression-free survival (PFS) and overall survival (OS), 95% (CI) and p-value. ETC, Etoposide/thiotepa/cyclophosphamide; Bu/L-PAM, busulfan/melphalan; CR, complete response; VGPR, very good partial response; PR, partial response; PD, progressive disease; SD, stable disease; Pts, patients.
Multivariate analysis of prognostic factors. Only statistically significant factors are reported. ETC, Etoposide/thiotepa/cyclophosphamide; Bu/L-PAM, busulfan/melphalan; HR, hazard ratio; CR, complete response; VGPR, very good partial response; PR, partial response; PD, progressive disease; SD, stable disease.
The median follow-up for the patient cohort was 41 months (range=6-120). Relapse occurred in 27 (77%) patients after a median time of 14 months (range=6-37 months) from diagnosis.
In univariate analysis (Table III), treatment with ETC conditioning regimen, a MYCN amplified status and no-response to the induction phase were statistically significant prognostic factors predicting worse survival and recurrence (p=<0.05). In detail, the 5-year PFS for the ETC conditioned group was 21% (95% CI=19-36%), while that of patients given Bu/L-PAM was 88% (95% CI=39-98%) (p=<0.05) (Figure 2). The 5-year PFS for patients in PD after the induction phase was 0, while the PFS was 52% (95% CI=28-72%) for patients in VGPR/CR and only 7% (95% CI=0-28%) in patients in PR (p=<0.001). The 5-year OS of patients with and without MYCN amplification was 26% (95% CI=5-53%) and 33% (95% CI =14-55%), respectively (p=<0.03).
In multivariate analysis, the treatment with ETC conditioning regimen was found to be a significant prognostic factor for recurrence/progression with hazard ratio (HR) of 12.7 (p=0.04), as well as the MYCN amplification which had HR of 4.5 (p=0.01). Major response at the end of the induction treatment was also associated with a favorable outcome (see also Table IV for details).

Progression-free survival (PFS). The Kaplan-Meier estimated curves for PFS of Bu/L-PAM patients versus ETC patients are presented.
Discussion
The use of HDC followed by PBSC rescue or ABMT for patients with high-risk NBL has been largely utilized over two decades. Since the results of the COG 3891 randomized trial were published (2), HDC has become a standard treatment after a multicycle induction and surgical removal of primary tumor. In a recent meta-analysis (24), it was reported that only three trials addressed the issue of the efficacy of autologous transplantation in a randomized way (2-4); despite this, the authors concluded that HDC with autologous hematopoietic stem cell rescue has to be considered standard post-induction treatment, able to improve the final outcome of patients with chemo-sensitive high-risk NBL.
The most effective conditioning for preventing disease recurrence has not been clearly identified and over the years, different regimens were proposed by international and/or cooperative groups. They were based on HDC with or without TBI; the main chemotherapeutic agents were etoposide, cyclophosphamide and carboplatin, which are also widely used in the induction phase plus L-PAM, busulfan and more recently, thiotepa and topotecan (2-11, 13-15, 25, 26). During the past decade, the use of TBI was progressively abandoned considering the lack of data supporting superior efficacy over chemotherapy and its long term toxicity. The CEM regimen (without TBI and with an increased dosage of etoposide and carboplatin) represents the standard conditioning regimen for first transplant in COG study (8), while different conditioning regimens were proposed for tandem transplantation strategies (9, 10, 27). More recently, the use of metabolic radiotherapy with 131I MIBG-alone or associated with cytotoxic drugs, followed by PBSC, has gained interest (28).
Since 1998, European groups have shown that a busulfan-based conditioning regimen was associated with a better outcome (14, 15). Moreover, in 2008, Ladenstein et al. on behalf of the EBMT pediatric working group, confirmed the prognostic role of the Bu/L-PAM conditioning regimen in a retrospective analysis of more than 3500 patients affected by NBL (16). In the ongoing SIOP Europe Neuroblastoma Protocol started in 2001, the issue of the most effective conditioning is being addressed in a randomized study comparing the Bu/L-PAM combination versus the CEM conditioning regimen.
The aim of our study was to evaluate the impact on survival and disease progression/recurrence of two different conditioning regimens in children with high-risk NBL treated prospectively with the same induction protocol in a single institution. Moreover, for all children, the same tools, in particular MIBG scan were used for defining disease extension as well as the response to treatment.
We found that the Bu/L-PAM regimen was associated with a more favorable outcome; the 5-year PFS for patients treated with ETC was 21%, while PFS for patients given Bu/L-PAM was 88% (p=<0.05). In this series, the favorable prognostic role of Bu/L-PAM was confirmed in multivariate analysis together with well-known prognostic factors such as MYCN amplification and response to the induction phase (5, 7, 11, 14-16).
Both proposed conditioning regimens were safe, as no toxic death related to HDC was recorded. As expected, the occurrence of liver toxicity, mainly veno-occlusive disease, was higher in patients treated with Bu/L-PAM. The toxicity of the ETC regimen was more manageable with few cases of extra-hematological grade 2-3 toxicity and a more rapid platelet recovery. Nevertheless, considering the impact on survival, the toxicity of the Bu/L-PAM regimen seems acceptable. Moreover, the slower platelet recovery we observed in BU/L-PAM recipients, did not translate into a delayed radiotherapy treatment, which is, nowadays, recommended to start at least 60 days after a busulfan-based conditioning regimen.
In our series, as in other larger series, the MYCN status and quality of response before HDC represented major prognostic factors; in patients with amplified MYCN and/or in those who achieved only a PR after induction chemotherapy, new experimental approaches such as tandem autologous transplantation, after HDC-alone or combined with 131I-MIBG, or allogeneic transplantation are needed. In this setting, thiotepa could be considered as a valid agent, mainly in sequential HDC, taking into account its mild toxicity and also its pharmacokinetics. Indeed, thiotepa and its major metabolite, tepa, reaches concentrations in the cerebrospinal fluid which are roughly equivalent to simultaneous plasma concentrations (29); these characteristics could be of particular value in patients with NBL and CNS metastasis who often do not achieve CR/VGPR at the end of the induction phase.
Our data clearly have limitations due to the small cohort of patients. Nevertheless, our experience suggests that a conditioning regimen based on the Bu/L-PAM combination is superior to that of the ETC regimen, with manageable toxicity and no toxic deaths.
Acknowledgements
The Authors thank Prof. Franco Locatelli for the critical review of the manuscript.
Footnotes
-
Conflicts of Interest
The Authors have no conflicts of interest to disclose.
- Received September 21, 2012.
- Revision received October 21, 2012.
- Accepted October 23, 2012.
- Copyright© 2012 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}