


Abstract
Aim: To understand the role of iPS inductive genes in esophageal cancer, we examined the expression of Sex determining region Y-box 2 (SOX2), Octamer-binding transcription factor 3/4 (OCT3/4), Krueppel-like factor 4 (KLF4), c-Myelocytomatosis viral oncogene (c-MYC) and Tir Na Nog (NANOG) using an esophageal squamous cell carcinoma tissue micrroarray. Materials and Methods: The immunohistochemical expression levels of the five genes were compared to the clinicopathological data of the 81 patients with esophageal cancer. Results: There was no relationship between the expression of the five genes and TNM factors of the patients. High expression of NANOG was an independent favorable prognostic factor (p=0.041). Among the patients who received postoperative cisplatin-based chemotherapy, patients with NANOG-positive tumor had significantly better prognosis than those whose tumors were NANOG negative (p=0.024). On the other hand, those with c-MYC-positive expression tended to have a worse prognosis and were resistant to cisplatin-based chemotherapy. Conclusion: NANOG expression was found to be an independent prognostic factor for patient with esophageal cancer. Patients with NANOG-positive expression tumor may be good candidates for cisplatin-based treatment.
Abbreviations: Esophageal squamous cell carcinoma (ESCC), Induced pluripotent stem cells (iPS).
Induced pluripotent stem cells (iPS) are cells that have acquired pluripotency due to the introduction of genes such as Sex determining region Y-box 2 (SOX2), Octamer-binding transcription factor 3/4 (OCT3/4), Krueppel-like factor 4 (KLF4), c-Myelocytomatosis viral oncogenec (c-MYC) and Tir Na Nog (NANOG) and Lin-28 homolog (LIN28) (1, 2). Although these factors are necessary for the acquisition of pluripotency by stem cells, they have also been suggested to have oncogenic potential for normal cells (3). Aoi et al. reported that gastrointestinal cells had less potential for carcinogenesis than did fibroblasts (4). Thus, the role of iPS-inductive genes in normal epithelial cells, normal mesenchymal cells and cancer cells is unclear. Furthermore, the influence of these factors on the proliferation and metastatic potential of cancer is also unclear.
We previously suggested that NANOG stimulates the growth and metastasis of breast cancer cells, whereas KLF4 inhibits these processes (5). In this study, we evaluated the expression of iPS-inducing factors in human esophageal squamous cell carcinoma (SCC) specimens by immunohistochemistry using a tissue mocroarray, and analyzed the association of these factors with the prognosis of the patients.
Materials and Methods
Tissue microarray. We used an esophageal SCC tissue microarray. A total of 114 patients with esophageal SCC from 1990 to 2008 were included. The tumor areas were selected with matched Hematoxylin and Eosin (HE) -stained slides and marked directly on the donor block. Each cylindrical tissue sample was cored (0.6 mm diameter) from the selected region in the donor block and extruded directly into the recipient block. Multiple 4 μm sections were cut with a microtome and transferred to glass slides (Super frost Plus, Fisher Scientific GmbH, Schwerte, Germany).
Patients. Out of 114 patients with esophageal SCC, 10 underwent R1 resection, two died in hospital, 13 underwent preoperative chemoradiation, and eight underwent preoperative chemotherapy; these patients were excluded from this study. Data of the remaining 81 patients with esophageal SCC were analyzed in this study. All eligible patients underwent R0 resections and did not die in hospital. The median follow-up time was 40 months. There were 72 male and 9 female patients. The average age of the patients was 64.5 years. TNM stage (ver 6) of the patients were as follows: stage 1: 11; stage 2a: 14; stage 2b: 12; stage 3: 36; and stage 4: 8. All M1 cases were cases with distant lymph node metastases only and these were removed by surgery. Forty-six patients underwent postoperative cisplatin-based chemotherapy. Of these, 40 patients received cisplatin plus 5-fluorouracil (FP) regimen and the other six patients received cisplatin alone or a FP plus doxorubicin hydrochloride regimen. The Institutional Review Board at the University of Toyama approved this study (#20-57).
Characteristics of the patients according to the expression of each gene.
Immunohistochemistry. Antibodies for the immunohistochemical staining were selected as follows. c-MYC (ab32; Abcam, Cambridge, UK), OCT4 (ab19857; Abcam), SOX2 (AB5603; Millipore, Billerica, MA, USA), KLF4 (SC-20691; Santa Cruz, CA, USA), NANOG (IHC-00205; Bethyl Laboratories, Inc. Montogomery, TX, USA).
Glass slides with the primary antibodies were incubated at an optimized titer and diluted using Universal Blocking Reagent (BioGenex, Fremont, CA, USA) for 60 min. After washing three times with phosphate buffered saline (PBS), the slides were incubated for 30 min with biotinylated secondary antibodies (Vector Laboratories, Burlingame, CA, USA) diluted to 1:250 by Universal Blocking Reagent, washed three times in PBS, and then incubated for 45 min with Avidin–Biotin Complex Method Reagent (Vectastain Elite ABC Kit; Vector Laboratories). The reaction products were then rinsed twice with PBS, placed in 0.05 M Tris–HCl buffer (pH 7.5) for 5 min, and then developed with liquid 3,3-diaminobenzidine (Dako, Glostrup, Denmark) for 3 min. After the development, the slides were washed twice with distilled water, lightly counterstained with Mayer's hematoxylin, dehydrated, cleared, and mounted with resinous mounting medium. All procedures were carried out at room temperature (5).
Immunohistochemical analysis. Two researchers analyzed the expression of each gene independently, and scored the intensity of expression as 0 (no expression), 1 (weak expression), 2 (moderate expression), or 3 (strong expression). They also scored the distribution of expression as 0 (none), 1 (1-50% of tumor cells), or 2 (51-100% of tumor cells). Expressions of genes were evaluated by the sum total of the staining intensity and distribution. On the basis of the total score, each patient was then classified into one of two groups, which were a low expression group (total score of 0-3) or a high expression group (total score of 4 or 5). Regarding the expression of NANOG, a score of 3 or more was defined as positive according to the distribution of the sum total score.

SOX2, OCT3/4. KLF4, c-MYC and NANOG expression in tissue microarray. All genes stained not only in the cytoplasm but also in the nuclei. Magnified areas shown on the right represent positive staining for each gene.
Statistical analysis. The chi-square test, Fisher's exact test and t-test were used to compare clinicopathological data. The overall survival (OS) rate and the cause-specific survival (CSS) rate after surgery were calculated for each group by the Kaplan–Meier method, and differences were assessed by the Log-rank test and Wilcoxon test. For evaluation of cluster analysis, the Wald method was used. A p-value less than 0.05 was assumed to indicate significance. All analyses were carried out with JMP 9.0 software (SAS Institute Inc, North Carolina, USA).
Results
Of 81 spots, 80 spots were evaluable for KLF4, SOX2 and c-MYC, 79 spots for OCT3/4, and 76 spots were evaluable for NANOG because some spots did not have enough cancer cells for evaluation or they peeled off during the staining procedure. As a result of immunohistochemical staining with antibodies to c-MYC, NANOG, and SOX2, nuclei were stained mainly and a low amount of cytoplasm was also stained. The nuclei and the cytoplasm were stained to the same degree on immunohistochemical staining with antibodies to KLF4 and OCT3/4 (Figure 1).
Tumors from 34 patients (44.7%) were positive for NANOG, 30 (37.5%) for KLF4, 42 (52.5%) for c-MYC, 22 (27.5%) for SOX2 and 24 (30.4%) for OCT3/4 (Table I). The expression of these five genes was not associated with the depth of tumor, lymph node metastasis or pathological stage.
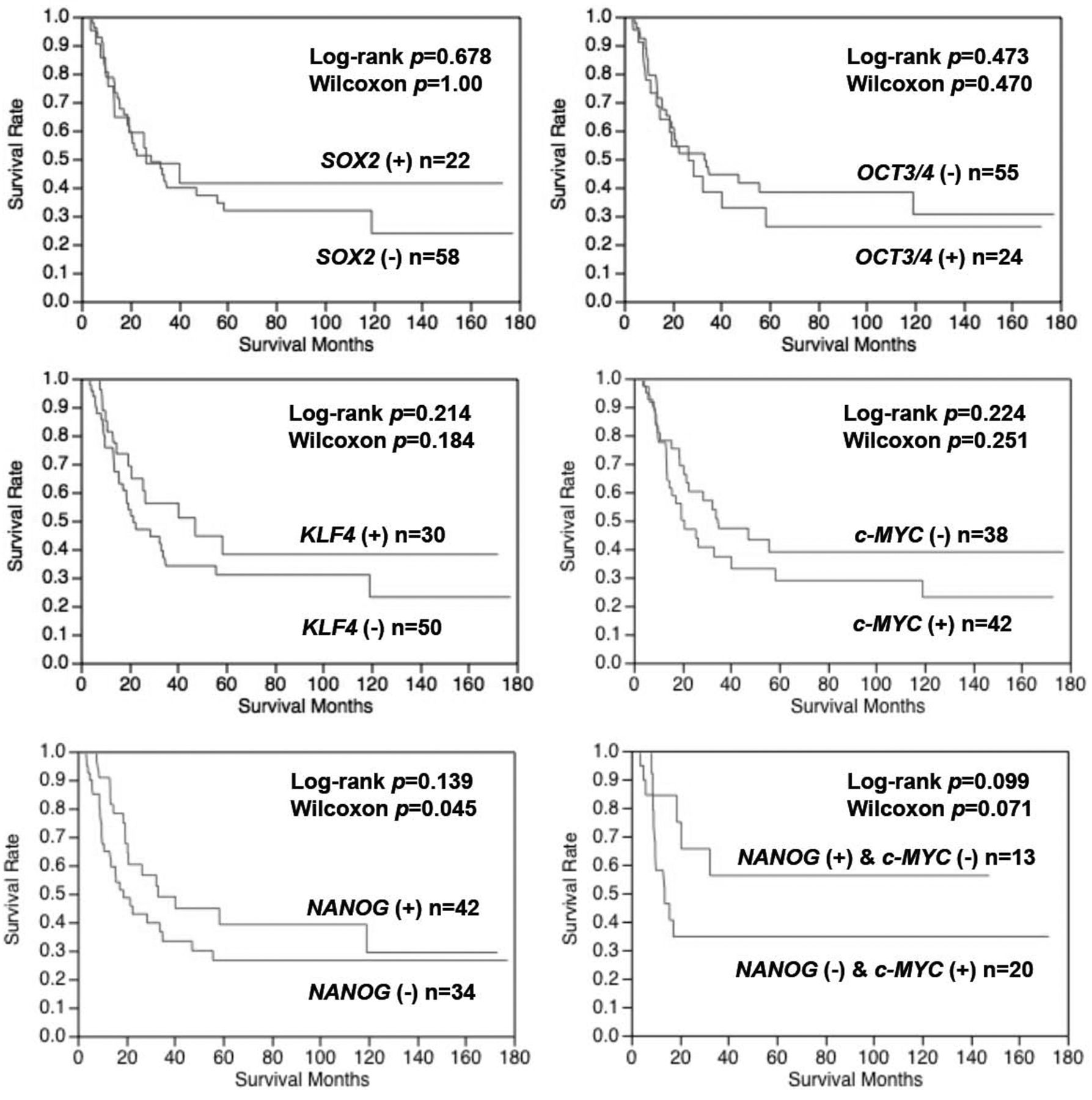
KLF4 expression was associated with histological types; however, other genes were not. Although the overall prognosis of the patients was not associated with these five genes, the cause-specific prognosis of the patients with tumor with high expression of NANOG was significantly better than that of those with low expression of NANOG (p=0.043) (Figure 2). Furthermore, NANOG expression was an independent prognostic factor regarding cause-specific prognosis (risk ratio=0.5, p=0.031) (Table II). Patients with c-MYC-positive tumor tended to have a worse prognosis than those with c-MYC-negative tumors, however c-MYC was not an independent prognostic factor for the patients (Table II). Combination analysis of NANOG and c-MYC revealed that the prognosis of the patients with NANOG positive and c-MYC negative tumors were better than that of those with NANOG-negative and c-MYC-positive tumors, however, there was no statistical significance (Figure 2).

Cause-specific survival curves of the patients regarding expression of SOX2, OCT3/4. KLF4, c-MYC and NANOG. The prognosis of the patients with a high expression of NANOG was significantly better than that of those with a low expression of NANOG (p=0.043, generalized Wilcoxon test).
With regard to chemosensitivity, patients with NANOG-positive tumors had significantly better prognosis than those with NANOG-negative tumors among the patients who underwent postoperative cisplatin-based chemotherapy (Figure 3A). Patients with c-MYC-positive tumors also tended to have a worse prognosis than those with c-MYC-negative tumors (Figure 3B). On the other hand, among the patients without postoperative chemotherapy, the prognosis of the patients did not differ between those with NANOG positive and those with NANOG negative tumors (Figure 3C), nor between those with c-MYC-positive and c-MYC-negative tumors. (Figure 3D). The background of the patients with postoperative chemotherapy did not differ depending on NANOG or c-MYC expression (Table III).
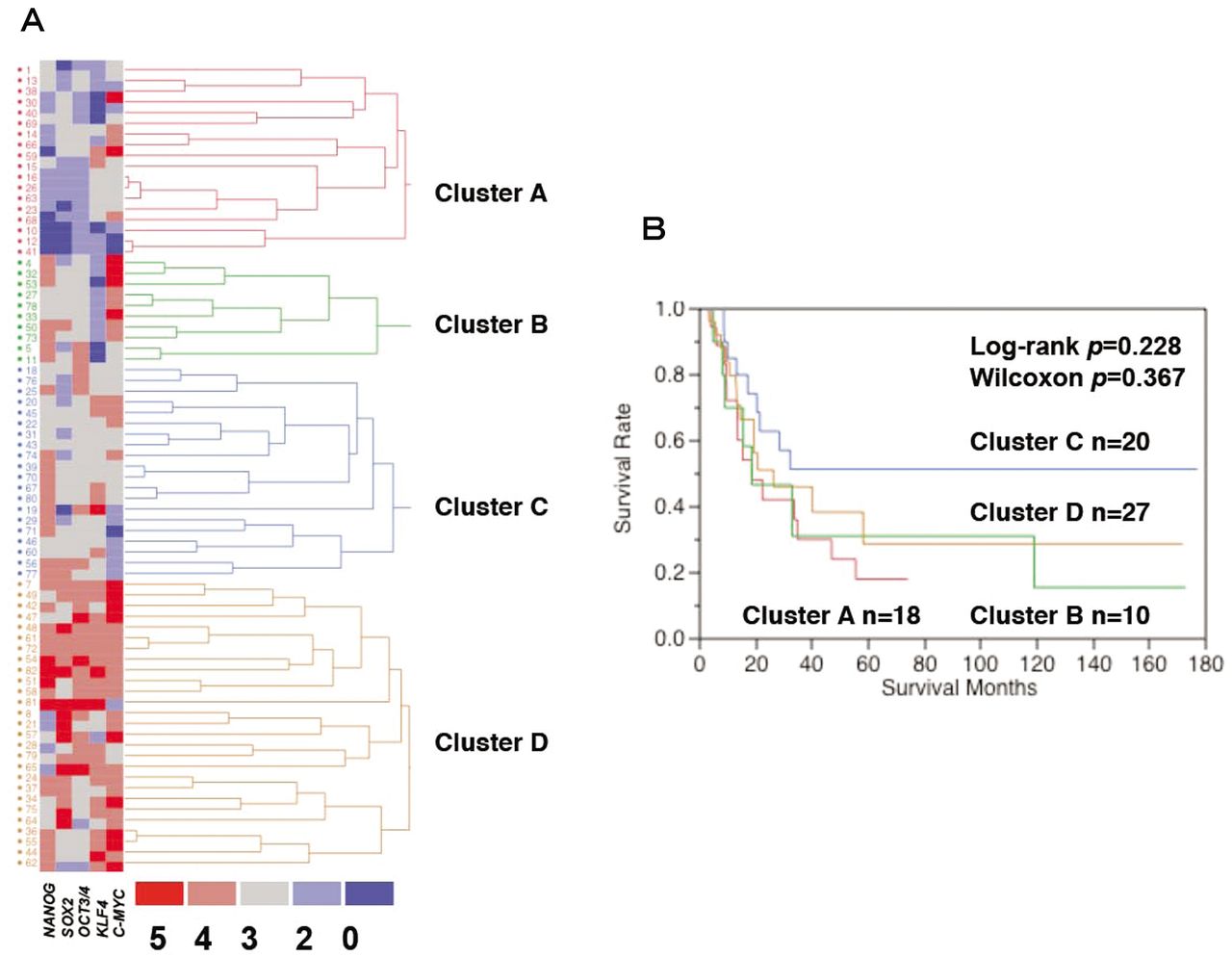
In clustering analysis, 75 cases had complete sets of all genetic data and were evaluable for analysis. Clustering analysis with absolute levels of expression of each gene resulted in four clusters (A, B, C and D) (Figure 4A). The patients in cluster C, which represents those with positive expression of NANOG low expression of c-MYC, and moderate expression of KLF4, SOX2, and OCT3/4, had a better prognosis than patients in other clusters (Figure 4B).
Discussion
iPS were induced from the somatic cells of mice and human fibroblasts by Takahashi and Yamanaka (1). Among the iPS-inducing factors (OCT3/4, SOX2, KLF4, c-MYC, NANOG, and Lin28), NANOG is known to control the differentiation of embryonic stem (ES) cells, and it also has a role in maintaining self-repopulating ability (1).

A and B: Survival curves of the patients who received postoperative cisplatin based chemotherapy according to tumor expression of NANOG and c-MYC. Patients with NANOG-positive tumors had a significantly better prognosis than those with NANOG-negative tumors. C and D: Survival curves of the patients who did not receive postoperative cisplatin-based chemotherapy according to tumor expression of NANOG and c-MYC. The prognosis of the patients did not differ between the patients with NANOG-positive and NANOG-negative expression.
Cox multivariate analysis of the patient data.
Recently, Du et al. reported that the occurrence of NANOG expression was positively correlated with the TNM stages and the histopathological differentiation of esophageal SCC tumors (p<0.01) (6). However, they did not mention the outcome of the patients. Contrary to this report, our results did not show any association between the TNM stage and histopathological differentiation. Our results also suggest that positive expression of NANOG is associated with a favorable prognosis of patients with esophageal cancer. Furthermore, NANOG expression was an independent prognostic factor for patients with esophageal cancer.
The background of the patients treated with and without postoperative cisplatin-based chemotherapy.
With regard to chemosensitivity, Du et al. also reported that NANOG siRNA enhanced the sensitivity to cisplatin chemotherapy in esophageal cancer in an in vitro study (6). Contrary to this report, our results clearly suggest that among the patients who underwent postoperative cisplatin-based chemotherapy, the prognosis of these with the NANOG-positive tumors was better than that of those with NANOG-negative tumors. Miyoshi et al. reported that the transcription factors OCT3/4, SOX2, KLF4, and c-MYC significantly induced up-regulation of NANOG mRNA in four cancer cell lines (7). They also suggested that retroviral-mediated introduction of iPS confers higher sensitivity to chemotherapeutic agents and differentiation-inducing treatment. Taken together, these data indicate that NANOG may be a good predictive marker for efficacy of cisplatin-based chemotherapy in esophageal cancer.
c-MYC gene is an important member of the MYC gene family, and can translocate and regulate a variety of substances, enable unlimited cell proliferation, and immortalize cells, and is involved in tumor development. Wang et al. suggested that positive c-MYC expression was significantly correlated with invasion depth and lymph node metastasis in esophageal SCC (8). They also suggested that the patients with positive expression of c-MYC had a significantly poorer prognosis than those without expression. Yang et al. reported that down-regulation of c-MYC effectively overcame AURORA-A-induced resistance to cisplatin in esophageal cancer cells (9). Although we did not find any significant difference, our results also suggest that c-MYC expression might have prognostic impact in esophageal SCC and c-MYC expression might be a predictor of resistance to cisplatin-based chemotherapy.
SOX2 is a high-mobility group box embryonic stem cell transcription factor that is expressed in the developing foregut and normal gastric epithelium and is down-regulated in intestinal metaplasia of the stomach and esophagus. Mendelson et al. reported that in a normal esophagus, OCT3/4-positive cells are located in the basal layer, representing a pool of progenitor cells (10). Thus both SOX2 and OCT3/4 are thought to be essential for proliferation in esophageal epithelia. Long and Harnick suggested that SOX2 is preferentially expressed in sSCC of the esophagus and anal canal compared to adenocarcinomas from these sites (11). Bass et al. performed fluorescence in situ hybridization (FISH) on tissue microarrays from 63 independent primary esophageal SCC samples and noted amplifications (3q26.33) in seven out of 63 cases, confirming the presence of recurrent amplifications in primary tumors (12). They found that SOX2 was a main target gene in 3q26.33 and suggested that Sox2-driven tumors show expression of markers for both squamous differentiation and pluripotency. Gen et al. reported that up-regulated expression of SOX2 was associated with poor differentiation of esophageal SCC (13). These studies suggest that SOX2 may have crucial role in carcinogenesis of SCC.

Clustering analysis and the prognosis of the patients using absolute expression levels of five genes. Cluster C represents the patients with a relatively high expression of NANOG, moderate expression of SOX2, OCT3/4 and KLF4, and low expression of c-MYC (A). Although there was no significant difference among the four groups, cluster C had better prognosis than other clusters (B).
With regard to the prognostic impact of SOX2 and OCT3/4, in a series of 162 consecutive patients with esophageal SCC, Wang et al. showed that 17.9% and 22.8% of the tumors highly expressed OCT3/4 and SOX2 proteins, respectively. They also suggested that the expression of these two factors was significantly associated with higher histological grade and poorer clinical survival (14). However, our data did not show any association between clinicopathological factors of the patients and survival. In lung cancer, Wilbertz et al. suggested that SOX2 gene amplification and protein overexpression are associated with a better outcome in squamous cell lung cancer (15). Thus, the prognostic impact of SOX2 in SCC is still controversial.
KLF4, a member of the KLF family of transcription factors, plays a key role in proliferation, differentiation, and carcinogenesis in a number of gastrointestinal tissues. KLF4 has distinct functions in esophageal carcinogenesis in mouse models (16). Ectopic expression of KLF4 inhibits survival and invasion (17, 18). Although our results did not show a significant impact on prognosis, KLF4 might have favorable prognostic impact on the patients with esophageal SCC. Furthermore, our results suggest that KLF4 was associated with histological type. Thus KLF4 might be related to carcinogenesis of esophageal SCC.
Clustering analysis revealed that patients in the cluster with NANOG-positive, c-MYC-negative and moderate expression of other iPS genes had better survival compared to those of the other clusters. Thus, in esophageal cancer, NANOG and c-MYC may have a higher prognostic impact than SOX2, OCT3/4 and KLF4.
Finally, it has been well known that due to tumor heterogeneity, a single section from a tumor is not always representative of all the characteristics of the tumor. Although our tissue microarray used one section from the tumor, a careful selection by a skillful pathologist may reduce such a weakness. Thus, we believe that our study may introduce helpful information to understanding the esophageal SCC.
In conclusion, the expression of various iPS inductive factors (c-MYC, KLF4, OCT3/4, SOX2 and NANOG) was detected in esophageal cancer specimens. NANOG expression was associated with favorable prognosis in patients with esophageal cancer, whereas c-MYC expression might indicate a worse prognosis in patients with esophageal cancer. Furthermore, NANOG may be a marker of cisplatin sensitivity and c-MYC a marker of cisplatin resistance.
Acknowledgements
The present study was supported by a research grant from the Japanese Ministry of Education, Culture, Sports, Science and Technology (MEXT/JSPS KAKENHI Grant Number B:23390320), and a research grant from the Japan Society for the Promotion of Science (JSPS) (Funding Program for World-Leading Innovative R&D on Science and Technology (FIRST Program). The authors declare that they have no conflicts of interest.
- Received October 11, 2012.
- Revision received October 30, 2012.
- Accepted October 31, 2012.
- Copyright© 2012 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}
{kind=link}