


Abstract
Aim: To compare the overall survival (OS) in patients without recurrent hepatocellular carcinoma (HCC) after initial radiofrequency ablation (RFA) and in those with recurrence, treated with repeat-RFA. Patients and Methods: We compared OS between patients without recurrence (group A; n=150) and those with recurrence treated with repeat-RFA (group B; n=130). Results: One-, 3- and 5-year OS after initial RFA was 92.6%, 84.1% and 81.0%, respectively, in group A, and 99.0%, 84.1% and 61.8% in group B (p=0.296). There was no significant difference in OS between group A patients and patients with a single recurrent HCC (p=0.834). On multivariate analysis, serum albumin >3.5g/dl and first HCC recurrence, comprising of two or three nodules were significant predicting factors of poorer OS. Conclusion: Even if HCC recurs after initial RFA, survival comparable to that of patients without recurrence can be achieved in patients with a single recurrent tumor treated with repeat-RFA.
Hepatocellular carcinoma (HCC) ranks fifth among the most prevalent types of cancer worldwide and is the third most common cause of cancer-related death (1-4). Liver transplantation and surgical resection are considered curative therapies for HCC (2). When surgery is not possible, percutaneous ablation therapies, such as radiofrequency thermal ablation (RFA), or percutaneous ethanol injection (PEI), are usually considered as an alternative (1, 5).
HCC often recurs, even in patients who have undergone curative therapy, leading to high mortality rates (6). Recurrent HCC is due to micrometastases in the liver that are not detected before or during surgery, or to multicentric carcinogenesis in the underlying liver; in 68-96% of patients, HCC recurs at intrahepatic sites only (7). Hence, effective management of intrahepatic recurrent HCC is an important strategy in improving overall survival (OS) after curative treatment for HCC (8).
RFA is a minimally-invasive local treatment and an alternative to PEI that was introduced in Japan in 1999. It has been widely used as a curative treatment for HCC and has evolved into an important therapeutic tool (1-3, 9-12). RFA is less invasive and safer than surgical resection (13), and a region of ≤3 cm in diameter can be ablated with a single application. The technique is safe and effective for the treatment of small HCCs in patients who are unsuitable for surgical intervention due to insufficient hepatic reserve (1-3, 14). More recently, several investigators have used RFA to treat selected patients with resectable HCC, with favorable clinical outcomes, and the technique is gaining popularity in the treatment of resectable HCCs in many countries (14, 15). Recurrent HCCs that are confined to the liver may be amenable to appropriate additional therapies, leading to improved survival. RFA can be used whenever HCC recurs and is considered to be a reliable, effective and safe therapy for intra-hepatic recurrent HCC (16, 17). However, the impact of RFA treatment of recurrent HCC on survival has received little attention in previous studies, although the outcome of the initial treatment, the interval to the first recurrence of HCC, and OS have all been well-documented (16-20). The aim of the present study was to compare OS between patients with HCC who did not have any recurrence after initial RFA and in those for whom HCC recurred after initial RFA and who were treated with repeat-RFA.
Patients and Methods
Patients. We performed RFA for 395 treatment-naïve patients diagnosed with a solitary HCC in the Department of Gastroenterology and Hepatology at Osaka Red Cross Hospital, Japan between January 2004 and January 2012. Out of these patients, 27 who were lost to follow-up and 36 in whom ablation was incomplete or who had other malignancies that might affect their prognosis, were excluded from the study. Complete ablation by RFA was defined as no apparent residual tumor on dynamic computed-tomography (CT) performed within seven days after the procedure.
Our criteria for RFA therapy were as follows: (a) patient ineligible for surgical resection or liver transplantation; (b) patient refused surgery; (c) tumor size up to approximately 3 cm and tumor number up to three nodules; (d) absence of uncontrollable ascites; and (e) no extrahepatic metastases or vascular invasion. Whatever the type of recurrence, recurrent HCC in patients who met the above criteria was treated with RFA. PEI was performed for patients with intrahepatic recurrent HCC who were considered to be at risk or difficult to treat with RFA. For patients with recurrent tumors that would have been difficult to treat with either of these ablative therapies, hepatic resection was performed in those eligible for surgery; those not eligible for surgery or ablative therapies owing to liver function, tumor size, tumor location or tumor number underwent transcatheter arterial chemoembolization (TACE) (21). For patients with recurrent tumor who had extremely poor liver function or who refused therapy, no treatment was performed. Patients with extrahepatic recurrent HCC underwent TACE or received a systemic chemotherapy agent such as sorafenib (22).
Out of 176 patients with a first intrahepatic recurrence after initial RFA, 166 (94.3%) underwent additional therapy. RFA was the most commonly used modality (130/176; 73.9%), followed by TACE (20/176; 11.4%), PEI (8/176; 4.5%) and surgical resection (7/176; 4.0%). Out of six patients with extrahepatic recurrence after initial RFA, four (66.7%) underwent additional therapy; three underwent systemic chemotherapy and one underwent TACE. The patient who underwent TACE had recurrent HCC with invasion of the inferior vena cava. There were 150 patients without recurrent HCC after initial RFA (no recurrence, group A) and 130 patients were treated with repeat-RFA for a first recurrence (recurrence, group B). Thus, data from 280 patients were analyzed (Figure 1). We compared the OS of these two groups. We also categorized the group B patients into two subgroups: patients in whom the first HCC recurrence was a single tumor (group Ba; 83 patients) and those with recurrence comprising two or three nodules (group Bb; 47 patients). We compared the OS of these groups.
Before RFA, written informed consent was obtained from all patients. The study was a retrospective analysis of patients' records and all treatments were conducted in an open-label manner. The study protocol complied with all provisions of the Declaration of Helsinki.
HCC diagnosis. Hypervascular HCC was diagnosed using abdominal ultrasonography and dynamic CT (hyperattenuation during the arterial phase in all, or some of the tumors and hypoattenuation in the portal–venous phase). Arterial and portal phase dynamic CT images were obtained at approximately 30 s and 120 s, respectively, after the injection of contrast material. In all cases of hypovascular HCC, percutaneous tumor biopsy was performed according to the diagnostic criteria for HCC, proposed by the Japan Society of Hepatology (23). There were 256 hypervascular HCCs and 24 hypovascular HCCs. For all patients, abdominal angiography was performed before RFA. Before the initial RFA, we confirmed the presence of solitary HCC with no vascular invasion and no satellite nodules using CT during hepatic arteriography (CTHA) and arterial portography (CTAP) (24). CTHA and CTAP were performed again on all patients in whom HCC recurred.
Definition of recurrent HCC. We defined local tumor progression (LTP) as the presence on dynamic CT of a recurrent nodule adjacent to the area ablated by the initial RFA. Recurrence that occurred distant from the ablated area in the same segment, was defined as intrahepatic distant recurrence (IDR). Extrahepatic recurrence was determined using chest CT, whole abdominal CT and bone scintigraphy.
RFA procedure. The details of our RFA procedure have been previously described (25). Briefly, we primarily used a cool-tip needle (Radionics Corp., Burlington, MA, USA) to perform RFA. Using the intercostal or subcostal approach, a 17-gauge, 2 to 3 cm long cooled-tip electrode was inserted under real-time ultrasound guidance. The duration of a single RFA session was 12 min for the 3-cm electrode and 6 min for the 2-cm electrode. All procedures were performed under ultrasound guidance by one of five operators, all of whom had at least three years of experience of performing RFA. We used the artificial ascites technique to prevent collateral thermal injury when the anticipated RFA zone was in contact with a critical region, such as the hepatic flexure of the colon. We also used this technique to improve visibility when the index tumor was located in the hepatic dome area.
Follow-up. Follow-up after initial RFA comprised of periodic blood tests and monitoring of tumor markers, including alpha-fetoprotein and des-γ-carboxy prothrombin, which was measured using a chemiluminescent enzyme immunoassay (Lumipulse PIVKAII Eisai; Eisai, Tokyo, Japan). Dynamic CT and/or magnetic resonance imaging was conducted every 3-4 months after the initial RFA.
Statistical analysis. Data were expressed as the mean±standard deviation. Differences between the two groups were analyzed using the unpaired t-test for continuous variables; categorical variables were analyzed using Fisher's exact test. Univariate and multivariate analyses were used. Time-to-recurrence was defined as the interval between the initial RFA and the first confirmed recurrence. For analysis of OS, follow-up ended at the time of death from any cause, after a census of the remaining patients at the last follow-up visit. Cumulative OS was calculated using the Kaplan–Meier method and tested using the log-rank test. The Cox proportional hazard model was used for multivariate analysis of factors that were considered significant on univariate analysis. p-Values of <0.05 were considered statistically significant.
Results
Clinical characteristics. The baseline clinical characteristics of the patients in groups A and B are shown in Table I. The mean tumor diameter at the initial RFA and the mean observation period from that date to the last follow-up were 1.87±0.66 cm and 2.6±1.9 years, respectively, for group A and 1.94±0.62 cm and 3.5±1.8 years for group B. There were significant differences between the two groups in the cause of liver disease (p=0.005) and the pre-treatment alanine aminotransferase level (p=0.015). For group B, the mean time from initial RFA to first recurrence of HCC was 1.6 years, and the mean maximal tumor diameter at first recurrence was 1.67±0.61 cm for group B, 1.66±0.62 cm for group Ba and 1.68±0.61 cm for group Bb.

Study profile. HCC, Hepatocellular carcinoma; RFA, radiofrequency ablation; TACE, transcatheter arterial chemoembolization; BSC, best supportive care; PEI, percutaneous ethanol injection.
Comparison of OS between groups A and B. One-, 3- and 5-year OS after initial RFA was 92.6%, 84.1% and 81.0%, respectively, for group A, and 99.0%, 84.1% and 61.8% for group B. There was no significant difference between the two groups (p=0.296) (Figure 2).
Comparison of OS between groups A, Ba and Bb. One-, 3- and 5-year OS after initial RFA was 100.0%, 89.0% and 69.3%, respectively, for group Ba, and 97.5%, 77.7% and 49.2% for group Bb. There was no significant difference in OS between group A and group Ba (p=0.834), but a significant difference between group A and group Bb (p=0.015) was observed. There was an overall significant difference between all three groups (p=0.029) (Figure 3).
Baseline characteristics between the group A and the group B patients.
Univariate and multivariate analysis of factors contributing to OS. On univariate analysis, cause of liver disease (p=0.026), serum albumin >3.5 g/dl (p<0.001), platelet count >10×104/mm3 (p=0.001) and recurrence of HCC (p=0.029) were significant factors contributing to poorer OS (Table II). On multivariate analysis of the four factors that were found to be significant in the univariate analysis, serum albumin >3.5 g/dl (p=0.001) and first HCC recurrence with two or three nodules (p=0.047), contributed significantly to OS. The hazard ratios and 95% confidence intervals for these factors are shown in Table III.
Patterns of HCC recurrence. HCC recurred as a single-nodule in 83 of the patients treated with repeat RFA after initial RFA. Among these patients, LTP-alone was found in seven and IDR-alone in 76. Forty-seven patients had a first recurrence comprising of two or three nodules. Among these, IDR with LTP was found in seven patients and IDR-alone was found in 40 patients.
Efficacy of repeat-RFA for recurrent HCC. In group B, RFA was incomplete for eight patients (6.2%); reasons included poor visibility of the targeted tumor, fear of potential toxicity, poor liver function, technical impossibility and physical burden. RFA was incomplete for one group Ba patient and seven group Bb patients.
Causes of death in groups A and B. Sixteen patients in group A (10.7%) died during the follow-up period; the causes of death were liver failure in nine and miscellaneous causes in seven. Forty-four patients in group B (33.8%) died during follow-up; the causes were progression of HCC in 22, liver failure in 14 and miscellaneous causes in eight.
Major adverse events related to initial RFA. Major adverse events related to the initial RFA, as defined by current guidelines (26) were: biloma (one patient); refractory ascites (one); intra-abdominal bleeding (two); pneumothorax (one); and liver abscess (one). All of these problems improved during the hospitalization in which the RFA was performed. There was no needle tract seeding or death related to complications of the initial RFA, and consequently the mortality was 0%.
Major adverse events related to repeat-RFA for recurrent HCC. Major adverse events related to repeat-RFA for recurrent HCC were: biloma (one patient); refractory ascites (one); intra-abdominal bleeding (one); hemothorax (one); and hemobilia (one). All of these problems improved during the hospitalization in which the repeat RFA was performed. There was no needle tract seeding or death related to complications of repeat-RFA, and consequently the mortality was 0%.
Discussion
In most patients with HCC, successful RFA for HCC is followed by recurrence (6). However, recurrent HCCs are often confined to the liver for a long period of time and this offers opportunities for radical elimination of HCC. Although RFA is effective for the treatment of HCC, to our knowledge, its repeatability in the management of recurrent HCCs and the impact of this approach on survival had not been fully-evaluated until the present study.

Cumulative overall survival (OS) in group A (n=150) and group B (n=130). One-, 3- and 5-year OS after initial radiofrequency ablation was 92.6%, 84.1% and 81.0%, respectively, in group A, and 99.0%, 84.1% and 61.8% in group B. There was no significant difference between the two groups (p=0.296).
Univariate analysis contributing to overall survival after initial radiofrequency ablation.
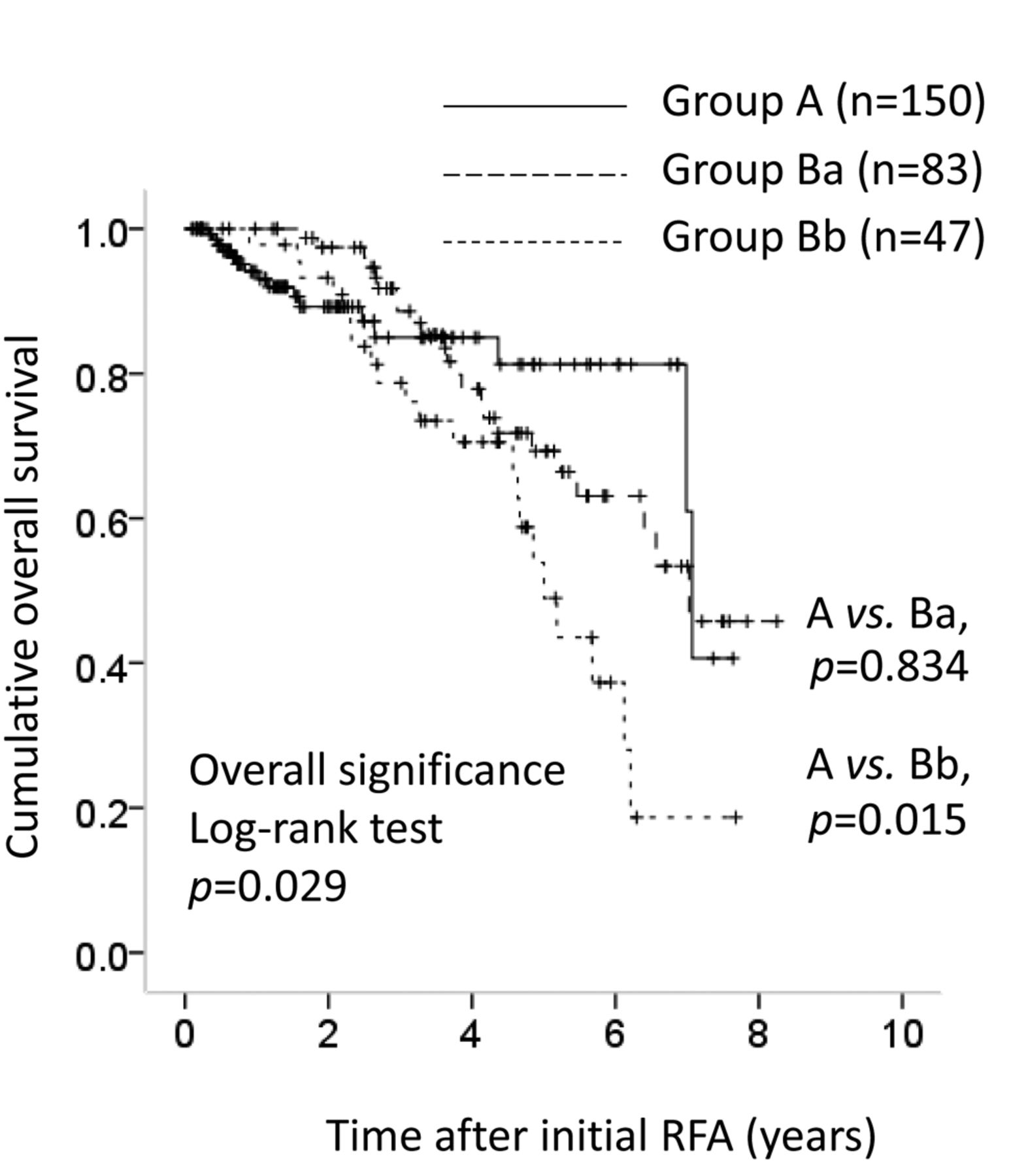
Cumulative overall survival (OS) in group A (n=150), group Ba (single first hepatocellular carcinoma (HCC) recurrence treated with repeat-radiofrequency ablation (RFA) after initial RFA; n=83) and group Bb (first HCC recurrence of two or three nodules treated with repea-RFA after initial RFA; n=47). One-, 3- and 5-year OS after initial RFA was 92.6%, 84.1% and 81.0%, respectively, in group A, 100.0%, 89.0% and 69.3% in group Ba, and 97.5%, 77.7% and 49.2% in group Bb. There was no significant difference in OS between group A and group Ba (p=0.834), but there was a significant difference between group A and group Bb (p=0.015). There was an overall significant difference between these three groups (p=0.029).
Multivariate analysis contributing to overall survival after initial radiofrequency ablation.
In this study, there was no significant difference between groups A and Ba in terms of OS, although a significant difference was observed between group A and group Bb. On multivariate analysis, first recurrence of HCC as a single-tumor was not significant in terms of OS, but a first recurrence comprising two or three nodules was a significant adverse prognostic factor. Preventing recurrence of HCC is essential in improving survival (27). However, our results suggest that even if HCC recurs after initial RFA, a favorable clinical outcome can be achieved by repeat-RFA for patients with a single recurrent tumor. In group Ba, RFA of the first recurrence of HCC was incomplete in only one patient (1.2%), and this may be associated with the favorable clinical outcome of this approach. Achieving a sufficient margin of ablation seems to be essential not only for treatment-naïve patients with HCC, but also for those with recurrent HCCs (17, 25).
Serum albumin >3.5 g/dl was the strongest predictive factor linked to OS in our multivariate analysis. The serum albumin levels reflect liver function, and in our cohort liver function strongly influenced OS, as previously reported (18, 19). In general, a considerable proportion of patients with HCC have concurrent liver cirrhosis, and patients with liver cirrhosis have lower serum albumin levels and can develop protein-energy malnutrition (PEM) due to increased catabolism (28). PEM is associated with poor clinical outcome (29), but branched chain amino acid treatment may improve this (30).
RFA is a safe procedure. Serious complications related to RFA were observed in some patients in our study, but all improved during the hospitalization in which the RFA was conducted. Repeat-RFA may also be considered safe, although operators should be always aware of RFA-related complications and their potential morbidity and mortality.
There are several limitations to the present study. Firstly, this was a retrospective single-center study. Secondly, patients in whom ablation was incomplete after the initial RFA and those who were lost to follow-up were excluded, leading to bias. Thirdly, the mean observation periods for group A and group B were not balanced for survival analysis. Hence, a prospective study is be needed. However, our results demonstrate that even if HCC recurs after initial RFA, the survival of patients with a single nodule treated by repeat-RFA can be comparable to that of those in whom HCC does not recur. In conclusion, repea-RFA for recurrent HCC can be useful in optimizing clinical outcome in selected patients.
Acknowledgements
The Authors thank Haruko Takada for data collection.
Footnotes
-
Conflicts of Interest
The Authors declare that they have no conflicts of interest.
- Received July 25, 2012.
- Revision received September 24, 2012.
- Accepted September 26, 2012.
- Copyright© 2012 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}