


Abstract
Background: We have previously reported that macrophage migration-inhibitory factor (MIF) is associated with an unfavorable prognosis in hypopharyngeal carcinoma. Here, we quantified MIF expression in oral cavity carcinomas and looked for possible correlations with clinical outcome. Materials and Methods: MIF expression was assessed by immunohistochemistry in a cohort of 154 oral cavity carcinomas and was compared to eight specimens of tumor-free epithelia, 32 cases of low-grade dysplasia and 137 cases of high-grade dysplasia. Results: Marked increases in MIF-immunostaining intensity and MIF-positive tissue areas were seen in carcinomas as compared to dysplasia (p<10−6). MIF expression showed no correlation with recurrence, but was significantly higher (p=0.01) when a second primary tumor occurred. In addition, HPV(+) malignancies exhibited lower MIF expression. Conclusion: Our study revealed an association between tissue MIF levels and tumor progression in oral cavity carcinomas. Of note, high-level MIF expression was found in patients developing a second tumor during the follow-up period.
The incidence of head and neck cancer, as well as its rather dismal prognosis, call for the identification of new biomarkers for disease progression, with the hope of designing innovative therapeutic strategies (1). Therefore, we have focused on immunomodulatory effectors potentially contributing to tumor progression. Their presence can indeed correlate with clinical parameters and contribute to differential diagnosis. In this context, promising results have been obtained with galectins, a class of endogenous lectins triggering adhesion/growth regulation activity by binding to distinct glycoconjugates, e.g. ganglioside GM1 on T-regulatory cells, and cross-linking them (2, 3). Some galectins have been shown to be associated with unfavorable prognosis (4-10), and galectin fingerprinting has refinements in diagnosis (11, 12). Based on the emerging paradigm that immunomodulators possess pro-tumoral potential, we have also examined the presence of macrophage migration inhibitory factor (MIF). The latter is a pleiotropic pro-inflammatory mediator expressed by various cell types, such as endothelial and epithelial cells, macrophages and lymphocytes (13). The MIF protein is best known for its pro-inflammatory activity which counterbalances the anti-inflammatory action of glucocorticoids (14). MIF has been described to interact with sarcolectin and other proteins, triggering a wide spectrum of responses (15-17).
MIF signaling notably depends on interaction with the cytokine receptor CD74/CD44. MIF binding to its cognate receptor triggers the Mitogen-activated protein kinase (MAPK)/Extracellular signal-regulated kinase (ERK) signaling cascade, leading to an activation of cyclin D1 transcription and Cyclin-dependent kinase (CDK)-mediated phosphorylation of the Retinoblastoma (Rb) protein, resulting in stimulation of cell proliferation (18; for a review, see 17). Together with a positive impact on Cys-X-Cys (CXC) chemokine expression, MIF/CD74 co-localization accompanies increased vascularity in non-small cell lung cancer (19). MIF induces expression of matrix metalloproteinase-9 (MMP-9), a matrix-degrading enzyme in colorectal carcinomas and enhances tumor cell invasiveness (20). Also of importance is the fact that MIF favors angiogenesis by stimulating the production of angiogenic factors such as Interleukin-8 (IL-8) and Vascular Endothelial Growth Factor (VEGF) in breast and esophageal cancer (21, 22). These results led us to examine MIF in hypopharyngeal squamous cell carcinomas. In a previous study, we reported evidence pointing to a relationship between MIF expression and tumor progression (23). Likewise, others have demonstrated a promigratory activity of MIF in a cell model of head and neck cancer (24).
In order to examine whether MIF may also be relevant to oral cavity carcinomas, we undertook a study aiming to analyze a panel of 154 cases, using the same antibody preparation and methodology as before (23). For comparison, healthy controls (eight tumor-free epithelia, TFE) and pre-neoplastic areas (32 cases of low-grade dysplasia, LGD, and 137 cases of high-grade dysplasia, HGD) from peritumoral regions were processed under the same conditions. Data on MIF expression in oral cavity carcinomas were then analyzed to pinpoint any relation with clinical factors such as recurrence, metastasis, overall patient survival and the development of a second primary tumor.
Materials and Methods
Patients' characteristics. A total of 154 patients with oral cavity carcinomas who underwent surgery aimed at curative tumour resection, were studied. The patient files were compiled retrospectively (December 1996 to February 2008) from the records of Erasme (Brussels, Belgium), Centre Epicura (Baudour, Belgium), and CHU Saint-Pierre (Brussels, Belgium). The description of the tumor status was based on the histopathological grade of tumor differentiation and the TNM staging classification (25, 26). Detailed information on the patients' age, gender, tumor histopathology, treatment, response to treatment at the primary tumor site and follow-up data up to the last contact with the patient, together with the status of the disease at the last examination were available for all patients (see Table I). This study was approved by the local Institutional Review Board.
Immunohistochemistry. All tumor samples were fixed for 24 h in 10% buffered formaldehyde, dehydrated and routinely embedded in paraffin. The specimens were routinely processed according to an optimized protocol detailed previously (23). Briefly, immunohistochemistry was performed on 5-μm thick sections mounted on silane-coated glass slides. After a microwave treatment for antigen retrieval, hydrogen peroxide was used to block endogenous peroxidase activity. Thereafter, sections were successively exposed for 20 min to solutions containing avidin and biotin to avoid false-positive staining reactions resulting from endogenous biotin. These preliminary steps were followed by sequential incubations with (i) the primary antibody to MIF, (ii) the corresponding biotinylated secondary antibody (polyclonal goat anti-rabbit IgG) and (iii) the avidin-biotin-peroxidase complex [ABC kit, DakoCytomation (Glostrup, Denmark)]. Presence of antigen (MIF) in the sections was visualized by incubation with a chromogenic substrate mixture containing diaminobenzidine and H2O2. Finally, sections were counterstained with luxol fast blue. Controls included sections processed, without the incubation step, with the MIF-specific antibody.
DNA extraction. The formalin-fixed, paraffin-embedded tissue specimens were sectioned (10×5 μm), deparaffinized and exposed to proteinase K overnight at 56°C. DNA was isolated using the QIAamp DNA Mini Kit (Qiagen, Benelux, Belgium), according to the protocol recommended by the manufacturer.
Detection of Human Papillomavirus (HPV) by polymerase chain reaction (PCR) amplification. HPV detection was performed by PCR using GP5+/GP6+ primers (synthesised by Eurogentec, Liege, Belgium). These GP5+/GP6+ primers amplify a consensus region located within L1 region of the HPV genome. PCR for HPV-L1 DNA amplification was performed in 25 μl of a reaction mixture, containing 2 μl of extracted DNA, 2.5 μl 1x PCR buffer, 0.025 U Taq DNA polymerase (Roche, Mannheim, Germany), 200 μM dNTPs and 0.5 pmol of each primer. The cycling conditions for PCR were as follows: denaturation was performed at 94°C for 1 min, annealing was performed at 55°C for 1 min 30 s and extension was performed at 72°C for 2 min for a total of 45 amplification cycles. The first cycle was preceded by a 7-min denaturation step at 94°C. The last cycle was followed by an additional 10-min extension step at 72°C. Aliquots (10 μl) of each PCR product were electrophoresed through a 1.8% agarose gel and stained with ethidium bromide to allow for visualization of the amplified HPV-L1 DNA fragments (27).
Real-time quantitative PCR amplification of type-specific HPV DNA. DNA extracts were routinely tested for the presence of 18 different HPV genotypes using TaqMan-based real-time quantitative PCR targeting type-specific sequences of the following viral genes: 6 E6, 11 E6, 16 E7, 18 E7, 31 E6, 33 E6, 35 E6, 39 E7, 45 E7, 51 E6, 52 E7, 53 E6, 56 E7, 58 E6, 59 E7, 66 E6, 67 L1 and 68 E7. For the different real-time quantitative PCR assays, the analytical sensitivity ranged from 1-100 copies and was calculated using standard curves for 18 type-specific PCRs constructed with plasmids containing the entire genome of the different HPV types. Real-time quantitative PCR for the detection of β-globin mRNA was performed in each PCR assay to verify the quality of the DNA in the samples and to measure the amount of input DNA. The following HPV types that were tested were considered to be high-risk (hr): 16, 18, 31, 33, 35, 39, 45, 51, 52, 53, 56, 58, 59 and 66.
Computer-assisted microscopy. Quantitative assessment of MIF immunostaining was performed using a Zeiss Axioplan microscope, equipped with a colour CCD camera (ProgRes C10plus; Jenoptik, Jena, Germany). Morphological analysis was achieved using the KS 400 imaging software (Carl Zeiss Vision, Hallbergmoos, Germany). The quantitative analysis of immunohistochemical staining generated the following two variables: (i) the labeling index (LI), defined as the percentage of positive tissue areas, and (ii) the mean optical density (MOD), defined as the mean staining intensity of positive cells.
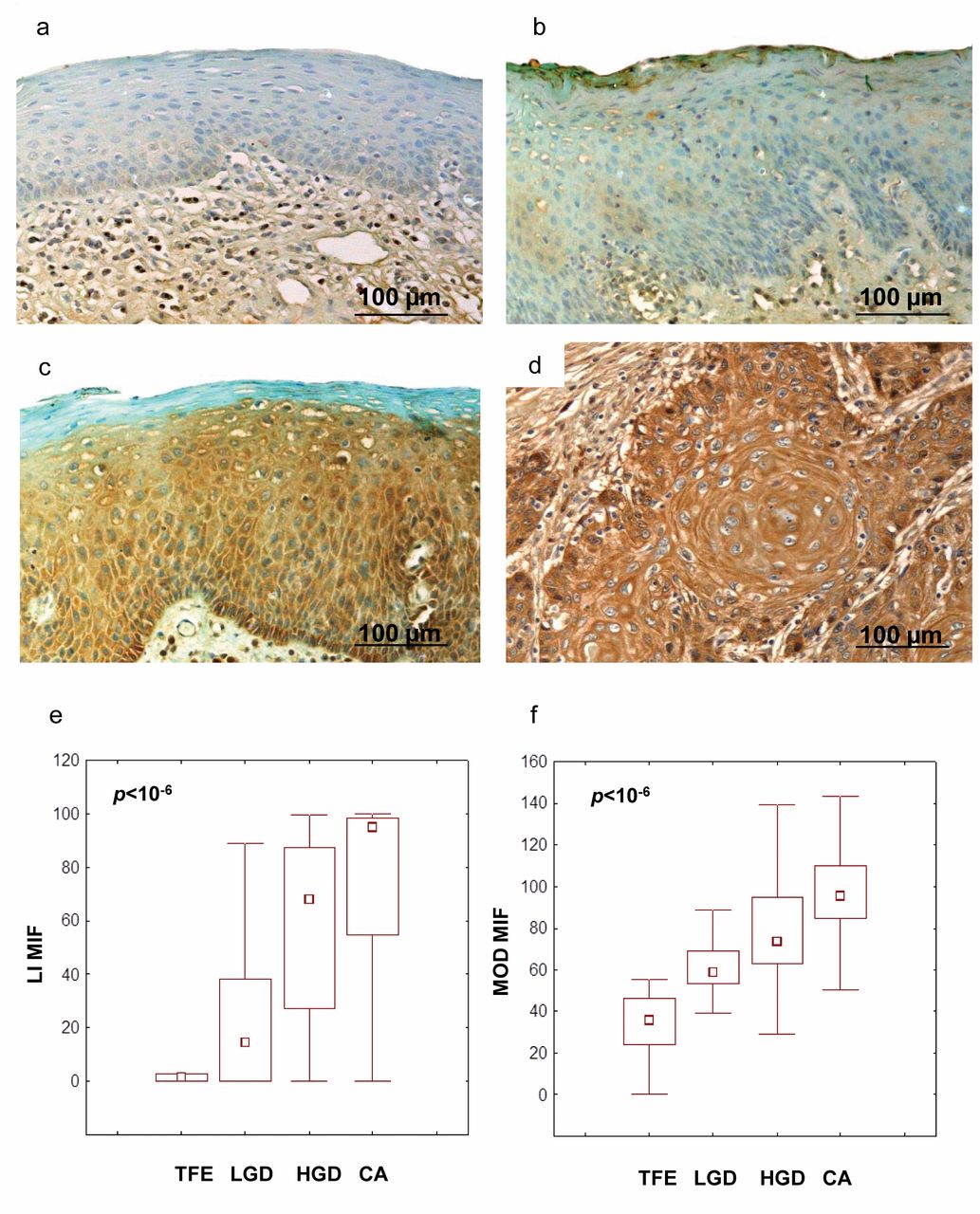
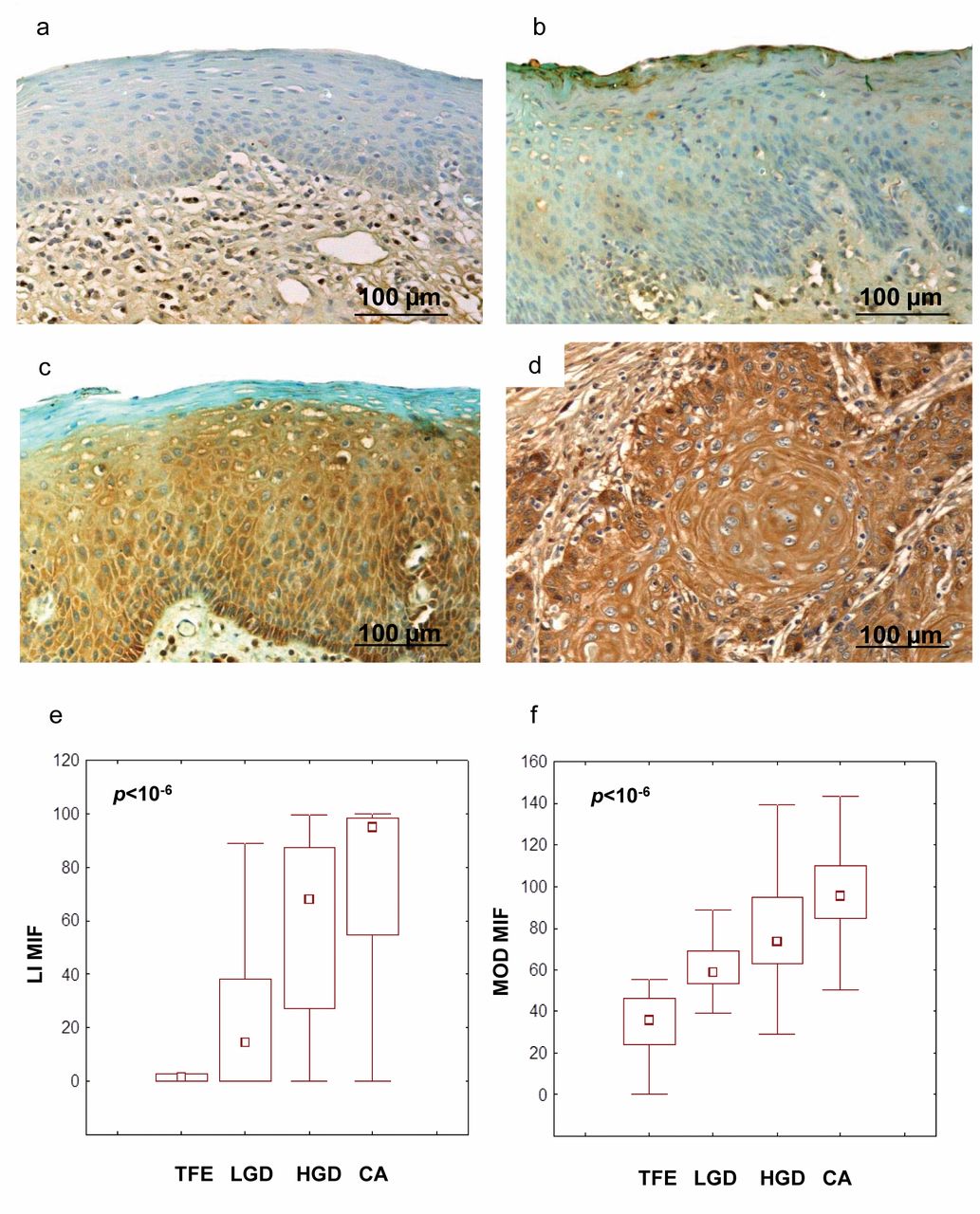
Immunohistochemical demonstration of Macrophage migration-inhibitory factor (MIF) in tumor-free epithelium (TFE) (a), low-grade dysplasia (LGD) (b), high-grade dysplasia (HGD) (c) and carcinoma (CA) (d). Quantitative determination of the percentage of tissue-area staining for MIF presence (LI) (e) and the intensity staining (MOD) (f) for TFE, LGD, HGD and CA. e, f: Non-parametric analysis of data by Kruskal-Wallis and post-hoc tests.

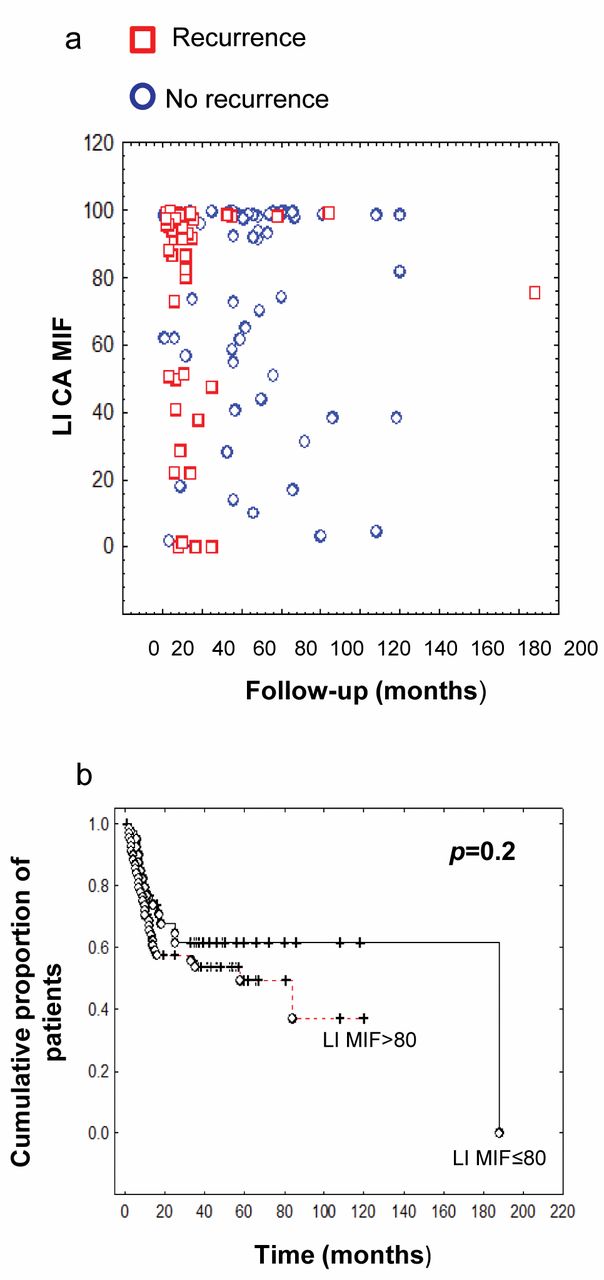
Macrophage migration-inhibitory factor (MIF) immunostaining expressed as Labeling index (LI) in oral cavity carcinoma specimens from patients with or without recurrence (a). Patient survival curves and log-rank test distinguishing between high expression of tissue MIF (LI >80, n=36) and low expression of MIF (LI ≤80, n=15) in tumors of patients with recurrence (log-rank test, p-value=0.2) (b).
Data analysis. Groups of data were compared using the non-parametric Mann-Whitney U-test (two groups) or Kruskal-Wallis test (more than two groups). In the latter case, post-hoc tests (Dunn procedure) were used to compare pairs of groups (to avoid multiple-comparison effects). The standard survival time analyses were performed using the Kruskall-wallis test and the Gehan generalized Wilcoxon test. As previously described, we applied a decision tree-based technique to determine the threshold MIF values required to discriminate for patient low- and high-MIF expression (5). Statistical analyses were carried out using the Statistica software (Statsoft, Tulsa, USA).
Results and Discussion
MIF expression during tumor progression in oral cavity squamous cell carcinomas. The intensity of MIF immunostaining was determined in a panel of 154 squamous cell carcinomas of the oral cavity. The staining patterns of these carcinomas were compared to eight cases of TFE, 32 cases of LGD and 137 cases of HGD. TFE generally stained weakly for MIF in the intermediate and superficial layers, when compared to dysplasia and carcinoma shown for comparison (Figure 1a-d). The LI increased during tumor progression (p<10−6, Kruskal-Wallis test, Figure 1e), as was also seen for the MOD (p<10−6, Kruskal-Wallis test, Figure 1f). On the basis of LI values, we observed significant increases between TFE and cancer samples (p=0.00006, post-hoc test), and also between TFE and HGD (p=0.02, post-hoc test). LI values were also significantly higher in HGD, as compared to LGD (p=0.006, post-hoc test), in cancer as compared to LGD (p<10−6, post-hoc test), and in cancer compared with HGD (p=0.00001, post-hoc test) (Figure 1e). A significant increase of MOD was apparent in cancer compared with TFE (p=0.00002, post-hoc test), in HGD compared with TFE (p=0.02, post-hoc test), in cancer compared with LGD (p<10−6, post-hoc test) or HGD (p<10−6, post-hoc test) (Figure 1f).
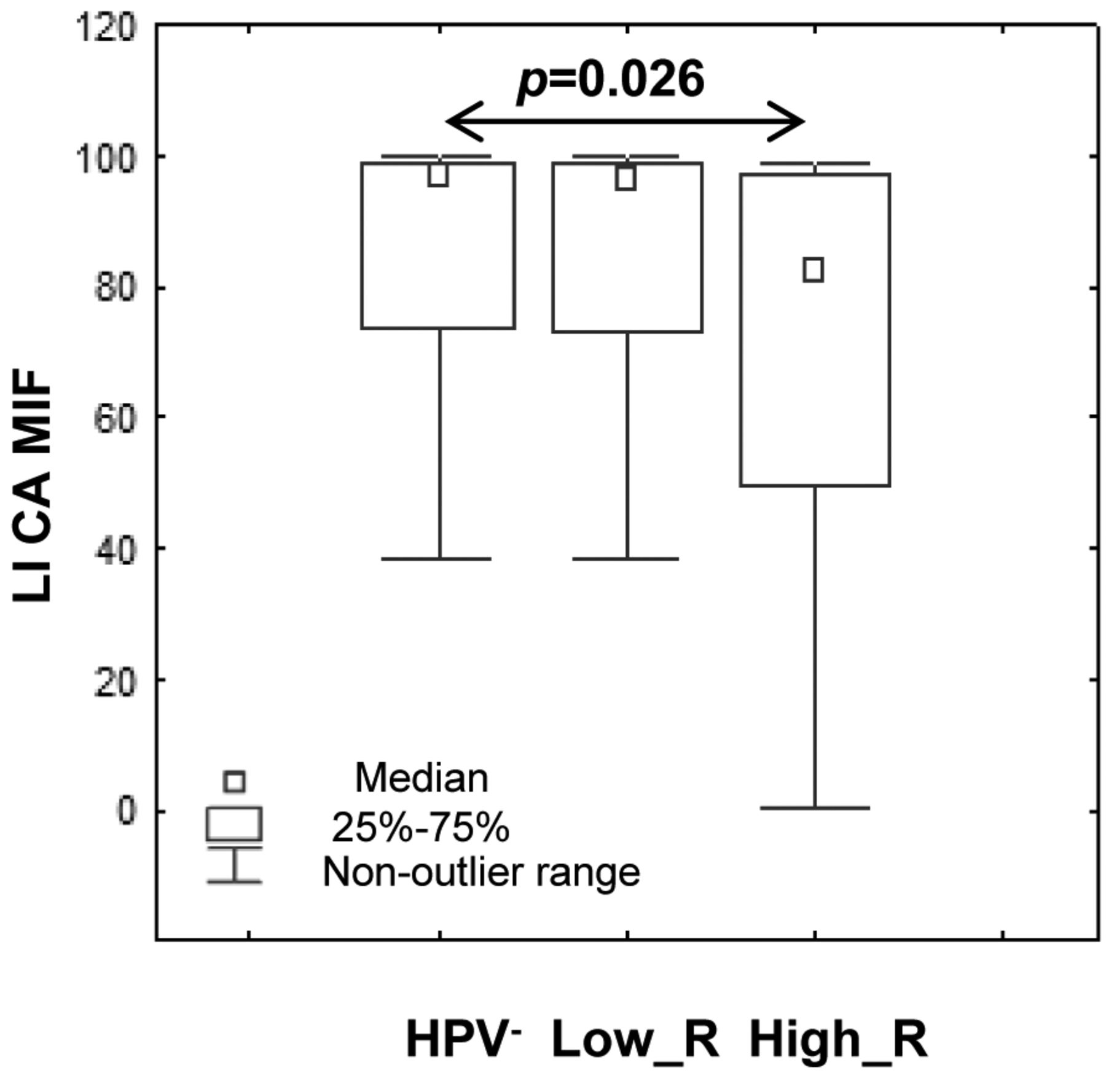
Increased MIF expression in tumor tissues is associated with the development of a second primary tumor during the follow-up period. Following the analysis of the staining patterns, we processed the data to look for possible correlations between MIF and clinical stage (T and N stage), recurrence and survival. No significant predictive measure for recurrence in patients suffering from oral squamous cell carcinoma (Figure 2a and b), even with the help of a decision tree technique used for identifying potential discriminatory thresholds for the two quantitative variables (LI and MOD), was found. In addition, no significant relation with TNM status or tumor grading was observed. Interestingly, the percentage of immunopositive tissue areas was significantly higher in patients with oral carcinoma presenting with a second primary tumor during the follow-up period. The staining for MIF in tumor tissues was also more intense in specimens (Figure 3a) from patients with a second primary tumor (n=12), compared with patients (Figure 3b) where no second primary tumor developed (n=91) (Mann-Whitney test, p-value=0.01, Figure 3c). Finally, we assessed whether MIF expression was related to HPV status. In our series of oral cavity carcinomas, a total of 44% were positive for hr-HPV types and 26% were positive for the low-risk HPV types. hr-HPV-type infection was mostly found in tumors with a low level of MIF expression (Figure 4).

Immunohistochemical demonstration of Macrophage migration-inhibitory factor (MIF) in a tumor of patients with a second malignancy (a) or without a second tumor (b). Patients with a second tumor location (n=12), present an increased level of MIF expression compared to patients who did not develop a second primary tumor (n=91) (Mann-Whitney test, p-value=0.01).
Based on the data described above, MIF presence may thus be included among the factors which can favor tumor progression and, possibly, favor development of further primary tumors. As noted before for hypopharyngeal tumors (23), MIF expression increased in parallel with neoplastic transformation (i.e. normal epithelium>dysplasia>neoplasia). These results encourage further investigations in vitro on cell culture models, as recently exemplified by a study of our group on laryngeal tumors (28). They also highlight the importance of galectin combination (e.g. the anti-apoptotic galectin-3, which uses intracellular binding to B-cell lymphoma-2 (BCL-2), and other members of the galectin family) which should be examined in order to pinpoint a potential for additive/synergistic effects. Induction of Cys-Cys (CC) chemokines by galectin-3 treatment of human monocytes (29) and up-regulation of MMP-9 expression in murine lymphoma cells and HeLa cells by galectin-7 (30, 31), which have also been shown to be correlated in laryngeal cancer (32), illustrates the relevance of this reasoning.
Patient population characteristics.

The human papillomavirus (HPV)-positive subgroup (and specifically the high-risk (hr_R) HPV+subgroup) is associated with low expression of MIF in oral carcinoma (CA) tissue, compared to low-risk (lr HPV+ and HPV-patients (Kruskal-Wallis test, p-value=0.026).
Acknowledgements
NK is the recipient of a fellowship from the Fondation Rose and Jean Hoguet. CD and GL are Senior Research Associates with the National Fund for Scientific Research (FNRS, Belgium). Support from an EC grant (contract no. 26060; GlycoHIT) is gratefully acknowledged.
- Received June 12, 2012.
- Revision received August 9, 2012.
- Accepted August 10, 2012.
- Copyright© 2012 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}
{kind=link}