


Abstract
Background: The prognosis of rhabdomyosarcoma (RMS) in children and adolescents has improved since the introduction of multi-agent chemotherapy. However, outcome data of adults with RMS are scarce. This multicenter retrospective study investigated the effect of age on outcome of RMS. Patients and Methods: Data were collected from three Dutch University Medical Centers between 1977-2009. The effect of age and clinical prognostic factors on relapse-free and disease-specific survival (DSS) were analyzed. Results: Age as a continuous variable predicted poor survival in multivariate analysis. Five-year DSS was highest for non-metastatic embryonal RMS, followed by non-metastatic alveolar RMS and was poor in metastatic disease. Higher age correlated with unfavorable histological subtype (alveolar RMS) and with metastatic disease at presentation in embryonal RMS. In non-metastatic embryonal RMS and in all alveolar RMS, higher age was an adverse prognostic factor of outcome. Conclusion: This study indicates that age is a negative predictor of survival in patients with embryonal and alveolar RMS.
Rhabdomyosarcoma (RMS) is a soft tissue sarcoma (STS) that occurs predominantly in children; 70% of cases are diagnosed within their first decade of life (1, 2). There is a second peak in incidence during adolescence (age 15-19 years), with RMS accounting for 1.7% of all malignancies in this age group (3). In adulthood, RMS is extremely rare, given that STS accounts for fewer than 1% of all malignancies, and that RMS comprises only 3.3 % of all STS (4).
The two main histological subtypes of RMS that occur in both adults and children are embryonal and alveolar RMS. Alveolar RMS, which occurs mostly in older children and adolescents, has a worse outcome compared to embryonal RMS, which is more common in young children.
The prognosis in children with RMS has dramatically improved during the past decades because of the introduction of multi-agent chemotherapy in consecutive multidisciplinary clinical trials, and treatment in a centralized setting (5-9). The Intergroup Rhabdomyosarcoma Study Group (IRSG) publications demonstrated successive increases in five-year survival rates between 1972 and 1997; from 55% on IRS-I (5) to 74% on IRS-IV protocols (8). In contrast, data on adults with RMS are scarce and in general show a worse outcome compared to the disease in children (10, 11). Additionally, a recent Surveillance, Epidemiology and End Results (SEER) report of 2,600 patients with RMS, confirms that no improvements in adults have been made over the past decades (12).
The reasons underlying the worse outcome in adult patients with RMS compared to children remain to be revealed. From larger pediatric studies, several prognostic factors have been established, such as site of the primary tumor (8), size below or above 5 cm diameter (12), histological subtype (14), stage of disease (15) and age at diagnosis (16, 17). In the scarce data on adult RMS, nearly identical factors have been described (10-12, 18-22).
To further substantiate the differences in outcomes between children and adults with RMS, the present Dutch multicenter study was conducted to investigate the role of age and other putative prognostic factors on outcome in a large cohort of both children and adult patients with RMS.
Patients and Methods
Patients. We selected all patients with RMS in PALGA, the Dutch National Histopathological Database System, treated at either the Pediatric Oncology Unit of the Department of Pediatrics or the Department of Medical Oncology at the University Medical Center Groningen, the Erasmus Medical Center, Rotterdam, or the Radboud University Nijmegen Medical Centre diagnosed between 1977 and 2009 (N=226). Patients were excluded if medical files were not available (N=10), or histological diagnoses were other than embryonal or alveolar RMS (N=47), as pathology reports were reviewed.
Data collection. The following data were collected: age at diagnosis, gender, site and size of the primary tumor, presence of metastases at diagnosis, metastatic site, lymph node involvement, treatment modalities (intention-to-treat principle), and follow-up status. Histological subtype was defined as embryonal or alveolar RMS. Botryoid RMS (a subtype of embryonal RMS occurring almost exclusively in infants and toddlers with a superior outcome) was analyzed separately.
Staging. Staging at diagnosis started with physical diagnosis. Evaluation of the location, size and local extent of the tumor was additionally evaluated with computerized-tomography (CT) and/or magnetic resonance imaging (MRI). Regional lymph nodes were considered positive when suspicious at physical examination, and when confirmed by CT scanning and/or histological or cytological evaluation. Further staging included chest X-ray and/or CT scan, bone scintigraphy and bone marrow aspiration. Pre-treatment staging in children was based on the IRSG classification (23). Adult patients were staged according to the TNM classification, based on local tumor extension and/or fixation to surrounding tissues (T), tumor size <5 cm or ≥5 cm, lymph node involvement (N) and presence of metastatic disease (M), and were translated into IRSG classification to facilitate comparison. Favorable locations of the primary tumor included the orbit, head and neck but not parameningeal, and paratesticular sites, whereas unfavorable locations included all other sites, as stated by the IRSG studies. Post-surgical clinical grouping (CG) staging was based on the extent of residual tumor after the initial resection, according to the IRSG clinical grouping system.
Treatment. Most children were treated according to the Children's Oncology Group (COG) or the International Society of Paediatric Oncology (SIOP) guidelines (24, 25). Local control consisted of primary surgery or surgery after neoadjuvant chemotherapy and/or radiotherapy. Adjuvant systemic treatment consisted of combinations of vincristine, D-actinomycin, and either iphosphamide or cyclophosphamide. Anthracyclines were added in the case of advanced disease.
Treatment of adults consisted of surgery and/or radiotherapy for local control following the STS protocols. Additionally, chemotherapy, mainly consisting of anthracyclines in combination with one or more of vindesine/vincristine, iphosphamide, and etoposide, was administered to the majority of adult patients.
Statistical analyses. Follow-up data were collected in a database and statistical analyses were performed by Statistics 16.0 (SPSS, Chicago, IL, USA). Frequency distribution of patient characteristics and prognostic factors for the different histological subtypes were assessed with the Chi-square test. The relation between age and prognostic factors was assessed using non-parametric testing with the Kruskal Wallis, or the Mann Whitney U-test when appropriate.
Overall survival (OS) probabilities were assessed using the Kaplan Meier method and compared with the log-rank test. OS was defined as the time from onset of disease until death from any cause. A multivariate Cox proportional hazards analysis, including age and other prognostic factors was used to analyze whether age was an independent prognostic factor in disease-specific survival (DSS) and relapse-free survival (RFS), using a backward conditional model. Furthermore, we tested the interaction between the effect of age and histological subtype on DSS and RFS. Treatment modalities were selectively tested based on clinical relevance. DSS was defined as the time from disease onset until death due to disease. RFS was defined as the time from the end of treatment with complete remission (CR) until local and/or distant recurrence. CR was defined as no evidence of residual disease at the end of treatment, confirmed by radiography and/or histopathology. Patients who never experienced an event were censored at the last contact date with the hospital and/or medical correspondence.
Results
Patients. A total of 169 patients were eligible for analysis. The median age at diagnosis was 8 years (range 0-73 years). Because all patients younger than 16 years were treated by a pediatric oncologist in all centers, we separated our patients into age groups <16 and ≥16 years. Patients' and tumor characteristics are summarized in Table I.
A significantly higher rate of alveolar subtypes and tumors arising at unfavorable sites (mainly involving parameningeal and extremity sites), more lymph node involvement, a higher rate of distant metastasis, a lower probability of CR, a higher rate of relapse, and a trend towards higher IRS stage was demonstrated in patients ≥16 years, in comparison to patients <16 years.
Pre-treatment prognostic factors. Age was significantly related to histological subtype (p<0.001, Table I, Figure 1A and B). Embryonal RMS occurred mainly in young children (median age=7 years). Botryoid RMS mostly occurred in infants and toddlers (median age=4 years). Alveolar RMS (median age=15 years) showed two peaks in incidence: one in young children and one in adolescence and young adulthood.
Because of this strong correlation, we compared prognostic factors for the different histological subtypes (Table II). Embryonal RMS was characterized by a significantly higher rate of favorable primary sites, absence of regional lymph node involvement and metastatic disease, with a consequently lower IRS stage at diagnosis when compared to alveolar RMS.
Patients' characteristics.
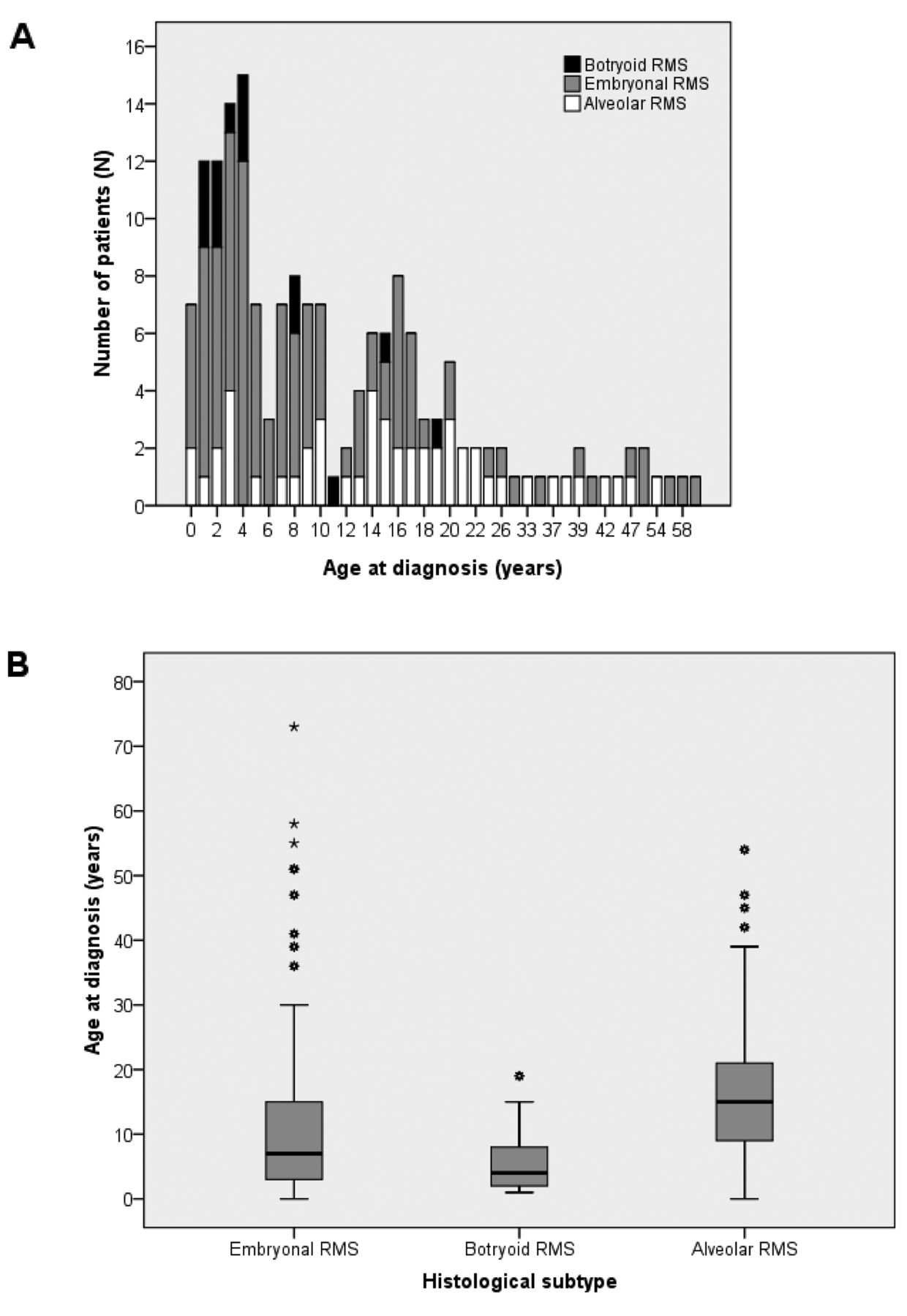
A: Frequency distribution by age and histological subtype. B: Age distribution by histological subtype. This figure shows the box plots of the age distribution by histological subtype. Stepwise non-parametric testing was performed. Age differed significantly between patients with alveolar (median=15 years) and those with embryonal RMS (median=8 years, p<0.001) and botryoid RMS (median=4 years, p<0.001). There was a trend for a difference in age between embryonal and botryoid RMS (p=0.084).
Pre-treatment prognostic factors by histological subtype.
In the largest group, namely embryonal RMS, higher age was related to a higher rate of metastatic disease at diagnosis (p=0.001) and IRS stage (p=0.002). Within the group of alveolar RMS, higher age was related to IRS stage (p=0.026), and there was a trend for a relation between higher age and greater lymph node involvement (p=0.079). Tumors arising at unfavorable primary sites (p=0.068), such as parameningeal versus other primary locations (p<0.001), were also related to higher age.
Treatment. Out of all 169 patients, six patients did not receive any treatment due to varying reasons (Table VIII). Out of the remaining patients (N=163), 22 did not complete treatment.
Surgery was performed slightly more frequently in patients <16 years (p=0.051), whereas radiotherapy was more frequently administered to patients ≥16 years (p=0.003, Table III). A significantly lower number of patients ≥16 years underwent chemotherapy when compared to patients <16 years (p=0.003). The reason why not all patients received chemotherapy could not be retrieved for all cases. Some patients were in a poor clinical condition, impairing administration of chemotherapy; others had had a resection of a small tumor and were apparently deemed to have been optimally treated in earlier years of this retrospective study. Most children received multi-agent chemotherapy but no anthracyclines (63.5%), with the addition of anthracyclines only to patients with advanced disease (29.6%). Adults mainly received anthracycline-based multi-agent chemotherapy, resulting in a more frequent use of anthracyclines in patients ≥16 years, when compared to patients <16 years (p<0.001).
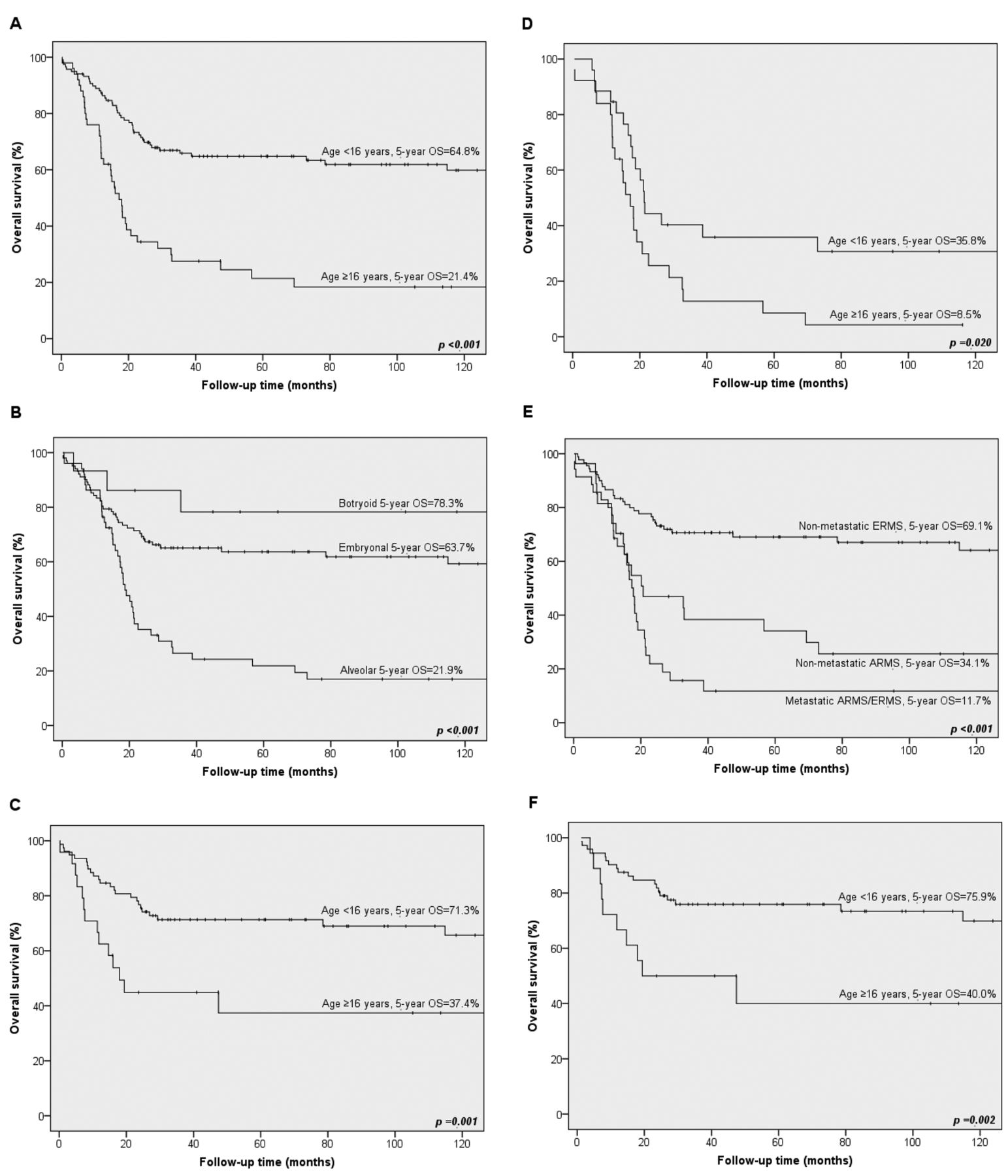
Survival. Five-year OS for the whole cohort was 52.0±4.0%. Patients ≥16 years had a disadvantage in outcome when compared to patients <16 years (5-year OS 21.4±6.4% versus 64.8±4.5%, p<0.001, Figure 2A).
A significant difference in survival was seen for the different histological subtypes (Figure 2B). Botryoid RMS had the best 5-year OS (78.3±11.1%), whereas alveolar RMS demonstrated poor outcome (5-year OS=21.9±6.1%). Patients with embryonal RMS had an intermediate 5-year OS of 63.7±4.9%.
For embryonal RMS, a superior survival was seen in patients <16 years (5-year OS=71.3±5.2%) versus patients ≥16 years (5-year OS=37.4±11.0%, p=0.001, Figure 2C). For alveolar RMS, an advantage in survival for patients <16 years, when compared to patients ≥16 years, was also seen (5-year OS=35.8±9.7% versus 8.5±5.8%, p=0.020, Figure 2D). In Figure 2E, we show OS in non-metastatic embryonal RMS (5-year OS=69.1±5.0%), non-metastatic alveolar RMS (5-year OS=34.1±9.5%), and metastatic embryonal and alveolar RMS (5-year OS=11.7±5.9%). Furthermore, within the subgroup of non-metastatic embryonal RMS, there was a significant disadvantage in survival for patients ≥16 years (5-year OS=40.0±13.0%), when compared to children <16 years (75.9±5.1%, p=0.002, Figure 2F). Exclusion of patients who did not receive chemotherapy resulted in a 5-year OS 49.2±15.4% in patients ≥16 years versus 78.1±5.0% in patients <16 of age (p=0.021).
Treatment characteristics by age group.
Prognostic factors. All RMS patients: In all RMS patients (Table IV), increasing age [p<0.001, Hazards Ratio (HR)=1.028], unfavorable primary site (p=0.012, HR=2.51), lymph node involvement (p=0.023, HR=1.94) and the presence of metastatic disease (p=0.009, HR=2.16) were multivariate predictors of poor DSS. Increasing age (p<0.001, HR=1.031) was the only significant multivariate prognostic factor of poor RFS, along with a trend towards a negative prognostic effect of alveolar subtype (p=0.057, HR=1.96) and metastatic disease (p=0.094, HR=1.89). To further exclude the interaction between the effect of age and histological subtype on outcome, we analyzed embryonal and alveolar RMS separately.

Rhabdomyosarcoma survival. Kaplan-Meier overall survival (OS) curves for patients with rhabdomyosarcoma (RMS) by age group (A), patients <16 years: N=118 patients, N at 5 years=51, patients ≥16 years: N=50 patients, N at 5 years=7; by histological subtype (B), embryonal RMS: N=102 patients, N at 5 years=41, botryoid RMS: N=15 patients, N at 5 years=8, and alveolar RMS: N=51 patients, N at 5 years=9; by age group for embryonal RMS (C), patients <16 years: N=78 patients, N at 5 years=36, patients ≥16 years: N=24 patients, N at 5 years=5; by age group for alveolar RMS (D), patients <16 years: N=26 patients, N at 5 years=7, patients ≥16 years: N=25 patients, N at 5 years=2; for non-metastatic embryonal RMS, non-metastatic alveolar RMS and metastatic embryonal and alveolar RMS (E), non-metastatic embryonal RMS: N=90 patients, N at 5 years 40, non-metastatic alveolar RMS: N=27 patients, N at 5 years=8, metastatic embryonal and alveolar RMS: N=35 patients, N at 5 years=2; and by age group for non-metastatic embryonal (F), patients <16 years at diagnosis: N=72 patients, N at 5 years=36, patients ≥16 years at diagnosis: N=18 patients, N at 5 years=4.
Prognostic factors in Cox proportional hazards analysis for all patients.
Embryonal RMS: In embryonal RMS (Table V), increasing age (p=0.001, HR=1.038), unfavorable primary site (p=0.006, HR=4.21), and lymph node involvement (p<0.001, HR=5.47) were significant multivariate predictors of poor DSS, whereas a trend was seen for metastatic disease (p=0.063, HR=2.45). Higher age (p<0.001, HR=1.043), unfavorable primary site (p=0.033, HR=2.50), and lymph node involvement (p=0.015, HR=3.47) were multivariate predictors of poor RFS.
To eliminate a possible effect of metastatic disease in older patients as mentioned before, non-metastatic embryonal RMS was analyzed separately (Table VI). Increasing age (p=0.001, HR=1.045), unfavorable primary site (p=0.011, HR=4.00), and lymph node involvement (p<0.001, HR=6.44) were significant multivariate predictors of poor DSS, whereas higher age (p<0.001, HR=1.043), and unfavorable primary site (p=0.045, HR=2.52) were predictors of poor RFS.
Furthermore, we investigated the effect of treatment modalities (chemotherapy, radiotherapy, surgery, and Clinical Group I-IV) on DSS in non-metastatic embryonal RMS. In univariate analysis, no administration of chemotherapy (p=0.011, HR=5.19, 95% Confidence Interval (CI)=1.47-18.63), no surgery for primary tumor and/or metastases (p=0.004, HR=3.66, 95% CI=1.515-8.83), and Clinical Group III versus I (p=0.013, HR=5.06, 95% CI=1.41-18.20) predicted poor DSS. In a multivariate model including age, lymph node involvement, primary tumor location, Clinical Group, radiotherapy, chemotherapy and surgery (N=79), higher age (p=0.005, HR=1.07, 95% CI=1.019-1.115), lymph node involvement (p=0.003, HR=6.51, 95% CI=1.90-22.25), Clinical group III versus I (p=0.021, HR=23.45, 95% CI=1.61-342.34), and no radiotherapy (p=0.048, HR=3.68, 95% CI=1.01-13.37) were predictors of poor DSS.
Prognostic factors in Cox proportional hazards analysis for patients with embryonal rhabdomyosarcoma (ERMS).
Alveolar RMS: In alveolar RMS (Table VII), there was a trend for poorer DSS with increasing age (p=0.078, HR=1.02), and metastatic disease (p=0.095 HR=1.82). A nearly identical result was seen for RFS.
Discussion
In this multicenter retrospective clinical study, we demonstrated in multivariate analysis that increasing age as a continuous variable is a strong prognostic factor of a poor therapeutic outcome in patients with embryonal and alveolar RMS aged 0-73 years. Moreover, histological subtype and clinical presentation at diagnosis (e.g. tumor location, lymph node involvement and presence of metastatic disease) were prognosticators of outcome in the whole cohort.
Whereas prognostic factors in children with RMS have been investigated extensively over the past decades (5-8), until recently, data on prognostic factors in adult patients were scarce, most likely due to the rarity of these tumors and the dispersion of patients treated in adult oncology centers (11).
Our study confirms previous findings in cohorts aged 0-75 years, with additional correction for treatment modalities. La Quaglia et al. were the first who described both adults and children with RMS and found age, TNM stage, and histological subtype to be prognostic factors of survival (22). Furthermore, a population-based study including 2,600 patients of all ages with RMS, was recently published (12), indicating that age, histological subtype, primary site location, stage, and local control with surgery and/or radiation were significant predictors of survival. In contrast to that large study, in this present study we attempted to add an analysis of chemotherapy schedules that were administered, excluding pleiomorphic RMS, which occurs exclusively in adults.
Histological subtype is an established prognostic factor of survival in RMS in children. This holds true with the present findings for the whole cohort in univariate analysis. Moreover, results of our multivariate model for the whole cohort indicate that this disadvantage in outcome for alveolar RMS might have a stronger relation to an unfavorable clinical presentation (e.g. unfavorable primary site and the presence of lymph node and distant metastases) than to alveolar histology itself, as reported by Sultan et al. (12). In addition, a trend for unfavorable primary location (i.e. parameningeal) and lymph node involvement at a higher age in alveolar RMS was found, which might explain the worse outcome in older patients. However, it should be mentioned that the documentation and assessment of lymph node involvement was suboptimal during the early time-period. Nevertheless, the reported effect of lymph node involvement on survival in the current study is in line with a recent report, and supports the view that lymph node involvement should be considered as an important prognosticator, especially in alveolar RMS (26). Regarding histological subtype, it should be taken into account that refinement of the histological diagnosis of RMS with molecular and genetic diagnostic techniques has been discribed in other studies during the period of our present research (7, 27).
Prognostic factors in Cox proportional hazards analysis for patients with non-metastatic embryonal rhabdomyosarcoma (ERMS, M0).
Prognostic factors in Cox proportional hazards analysis for patients with alveolar rhabdomyosarcoma (ARMS).
Treatment intention and follow-up.
Metastatic disease is a strong adverse prognostic factor in all patients with RMS, leading to poor survival not exceeding 30% (11, 12, 28, 29). In our cohort, 5-year overall survival of patients with metastatic disease hardly exceeded 10%. Importantly, the presence of metastatic disease correlated with higher age at diagnosis, even in the restricted group of embryonal RMS. Unfavorable clinical presentation with increasing age was also reported by others (11, 20, 21). Importantly, we found age to be a prognosticator of DSS in non-metastatic embryonal RMS. Although age as a prognostic factor in this particular subset of patients has been previously reported (22), to our knowledge, the present study is the first that has evaluated age as a continuous factor in multivariate analysis including treatment modalities.
Apart from tumor-specific factors, treatment-related aspects play a role in the final outcome of RMS patients. Pediatric patients (up to 21 years) are generally treated on study protocols developed by, for example, the SIOP (Europe) and COG (formerly IRSG, United States), including systemic treatment for all patients. In adults, we show that systemic treatment is administered, although less frequently, and comprising other agents. Of note, anthracyclines were applied more frequently as part of the primary treatment for adult patients. The underlying reason for this discrepancy in the treatment approach is not fully clear. The lack of international protocols for the elder RMS population and the rarity of the disease within the adult oncologic population may play an important role (30). Although we found that age remained of prognostic significance after including treatment modalities in a multivariate model, we were not able to correct for the different regimens and the given dose intensities. Whether these observed differences in chemotherapy schedules might play a role should be further investigated. Importantly, Ferrari et al. previously hypothesized that survival in adults would be comparable to that of children, if they received the appropriate treatment as prescribed in the current childhood regimens (11).
Other suggested explanations for poor survival of adults with RMS are differences in oncogenesis and biological behavior. Advanced clinical presentation with increasing age, as well as age per se being a prognostic factor in uniformly treated children, support this idea (17, 26, 31, 32). Despite investigations focusing on understanding oncogenesis and biological behavior, limited data are available with regard to age-related biological differences of RMS. Younger onset of RMS is associated with several rare syndromes that harbor specific genetic alterations, including those of the germline p53 tumor-suppressor gene, HRAS oncogene, and neurofibromin (NF1) gene, suggesting a different genetic background for early RMS genesis within these patients (33). Furthermore, the PAX7/FKHR translocation t(1;13)(p36;q14) in alveolar RMS, is associated with younger onset of disease, primaries of the extremity, localized disease, and better outcome, whereas the more common PAX3/FKHR translocation t(2;13)(q35;q14) is associated with higher age at diagnosis and represents a highly malignant phenotype with a predilection for bone marrow involvement and worse outcome (34, 35). However, although a recent study confirmed the relation of PAX3/FKHR with a higher age and metastatic potential, it did not confirm a higher rate of bone marrow involvement and worse outcome for patients with these tumor types (36). A higher expression of drug-efflux pumps in adult RMS, thereby potentially contributing to worse response to chemotherapy, was also proposed to explain differences in terms of biological behavior (37).
Conclusion
In conclusion, age is a strong adverse prognostic factor of survival in patients with embryonal and alveolar RMS. Whether the dismal outcome is caused by a biological or treatment effect remains to be elucidated. With the introduction of more homogeneous treatment protocols for both children and adults, the contribution of age-related biological factors can be further explored. Given the presumably lower tolerance of adults to high doses of chemotherapy administered in childhood RMS (20), dose schedules should be adapted. Based on the results of our study and the recently published SEER data, collaboration between pediatric and medical oncologists regarding patients with RMS is urgently needed, and should ideally take place at a global level, given the rarity of these tumors (30).
Footnotes
-
↵* Preliminary data of this study were presented and discussed at the ASCO Annual Meeting 2008, May 30-June 3 2008, Chicago, IL, USA. Session: Sarcoma, soft tissue, poster discussion, Abstract No: 10514.
- Received June 21, 2012.
- Revision received July 31, 2012.
- Accepted August 1, 2012.
- Copyright© 2012 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.