


Abstract
Curcumin's instability and its metabolite, tetrahydrocurcumin (THC) pose a major issue for the establishment of dependable pharmacokinetics and excretion profiles. Additional pharmacokinetic variances are associated with durations of intravenous infusions. We found that stabilizing curcumin with phosphoric acid allows accurate quantitative determinations of curcuminoids in the plasma and bile, by preventing degradation during the analytical processes. Two male and two females dogs were infused with Lipocurc™ 10 mg/kg over two hours, and another four dogs (two males and two females) were infused with Lipocurc™ 10 mg/kg over eight hours. Plasma levels of curcumin and THC were determined during the infusions and at necropsy. THC levels were 6.3-9.6-fold higher than curcumin during both infusion rates, suggesting a combination of a high-rate of enzymatic curcumin metabolism and a comparatively slower rate of blood THC clearance. When levels of curcumin and THC were compared during infusion durations, the two-hour infusion levels were significantly higher than the eight-hour infusion. The plasma half-lives of both compounds following the two-hour infusion ranged from 0.4-0.7 hours, and was a consequence of both hepatic and renal clearance However, at higher plasma concentrations renal excretion predominated, particularly with THC. Enhanced clearance rates were noted during eight-hour infusions, which prevented achieving a steady state. These observations suggest that for leukemias and lymphomas, the two-hour infusion may be advantageous based upon higher concentration profiles, and unstimulated clearance rates, however data on curcumin penetration into circulating hematopoietic cancer cells and efficacy data are required in order to confirm these suggestions.
Abbreviations: HPLC, high-performance liquid chromatography: LC-MS/MS, liquid chromatography-tandem mass spectrometry, THC, tetrahydrocurcumin.
The parenteral administration of Lipocurc™ with therapeutic, intent poses several questions relating to deciding an optimal rate of administration for patients with neoplastic diseases. Options ranging from bolus intravenous injections to constant infusions are impacted by enzymatic metabolism, pH-dependent degradation, renal and hepato-biliary excretion mechanisms. During pre-clinical toxicological evaluation in dogs, dose-dependent hemolysis was noted following brief infusions of 20 mg/kg and greater curcumin content. Ten mg/kg doses infused over 2 hours were non-toxic. This same two-hour infusion schedule was used in an ascending-dose Phase 1 trial in normal human subjects where the highest intravenous dose administered (5 mg/kg) was without adverse reaction. In planning a clinical cancer trial with parenteral Lipocurc™ the most efficient administration schedule will be a function of multiple pharmacological and cellular attributes. The only modality capable of modulation is the dose and schedule of administration. To avoid toxicity from a too-high Cmax we designed a two-hour infusion schedule, however in view of the unknown metabolic and elimination factors in dogs we compared two-hour and four-fold longer infusions (eight hours) to determine any advantages.
Materials and Methods
Plasma concentration data arising from the infusion of Lipocurc™ in eight (4 female and 4 male) Beagle dogs were used to assemble this report. The results and analysis for the study are presented for intravenous infusion dosing of a total dose of 10 mg/kg infused over a period of either 2 or 8 hours. Plasma levels of curcumin and its metabolite, tetrahydrocurcumin (THC) were measured at timed intervals post-initiation of dosing. All animals were killed and subject to necropsy 15 minutes post-infusion and samples of plasma, bile and urine were taken. The purpose of the study was to determine, the pharmacokinetics of curcumin and THC following two different rates of infusion and an analyte stabilization method using phosphoric acid (H3PO4). In this report the plasma pharmacokinetics, urine and bile levels of curcumin and THC are discussed. A summary of the treatment groups is presented below.
Summary of treatment groups.
Lipocurc™ was administered to 8 Beagle dogs by intravenous infusion over two hours (Part A) or eight hours (Part B), as shown in Table I. For the 2-hour infusion, blood samples were taken at pre-dose and 0.25, 0.5, 1.5 and at 2-hours during infusion and at 15 minutes post-infusion. For the 8-hour infusion, blood samples were taken at predose and 0.25, 0.5, 1.5, 4, 4, 6 and at 8 hours during infusion and at 15 minutes post-infusion.
For all groups, plasma curcumin and THC were determined using a method developed by the Bioanalytical Department at Nucro-Technics (1). Bioanalysis was performed on two sets of samples, one that was treated with phosphoric acid and one that was not. Phosphoric acid was used to treat one set of samples based on preliminary studies indicating that phosphate increased the stability of curcumin and THC in the tissue matrix. Values that were below the limit of quantification were assigned a value of 0.
As there were no consistent differences between the plasma levels of curcumin in male and female dogs, the average plasma concentrations from male and female dogs were used to perform the PK analysis. Plasma concentration vs. time profiles were analyzed averaging the data from four dogs. Plasma profiles for the test article are presented as the mean data±SE of four dogs. Average plasma concentrations were used to perform the PK analysis. Plasma concentration vs. time profiles were analyzed and the PK parameters were estimated using WinNonlin Version 5.2.1, employing the intravenous infusion model with first order elimination. The plasma concentration-time profiles for the test articles are presented as the mean data±SE of four dogs.
Results
The plasma levels and AUC of curcumin and THC following either 2-hour (high rate) or 8-hour (low rate) infusion were clearly higher in the presence of phosphoric acid (Figure 1, Tables I and II), suggesting that phosphoric acid increased the stability of curcumin and THC in plasma samples. This was also the case for bile, but less so, while for urine the impact of the addition of phosphoric acid was variable (Figure 2). Equivocal data for the bioanalysis of curcumin in the plasma of rats not treated with phosphoric acid has been observed in the literature following oral administration of high doses (2). Detection methods, rather than plasma stability were speculated as the reason for the discrepancy, however, it appears that plasma/tissue stability would also be an issue in the bioanalysis of curcumin. For consistency and in light of the impact of phosphoric acid on the quantification of curcumin and THC in plasma, a discussion of the results of this study will be based on the bioanalysis of plasma, bile and urine samples in the presence of phosphoric acid.
AUC of plasma concentration vs. time for curcumin and THC upon bioanalysis in the presence and absence of phosphoric acid1.
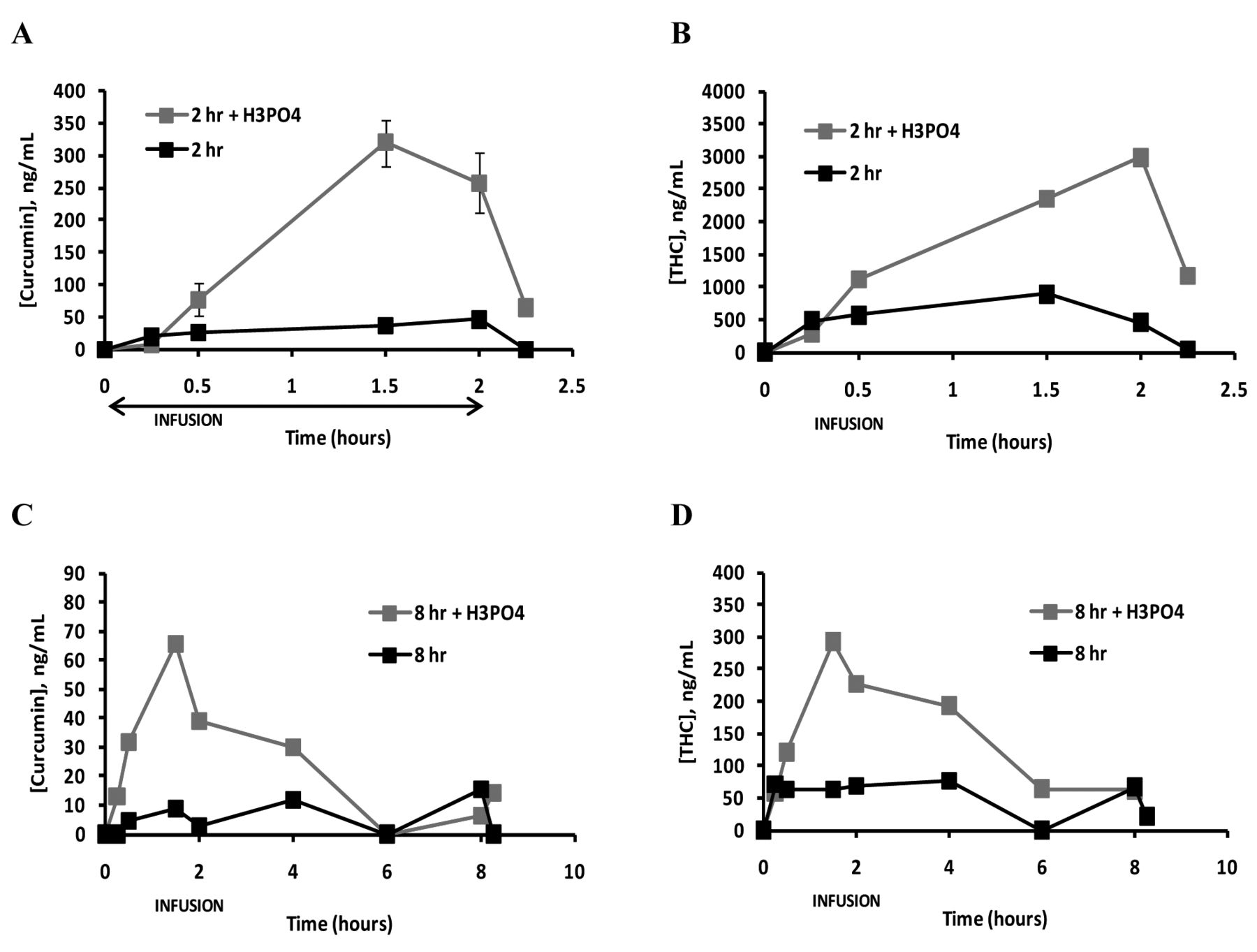
Upon a two-hour infusion of curcumin at 5 mg/kg/hr (total dose 10 mg/kg), the plasma levels of curcumin rose to attain a maximum concentration of 320 ng/mL by 1.5 hour, and then began to stabilize/fall during the infusion. Upon cessation of the infusion, there was a rapid drop in plasma concentrations of curcumin from 257 ng/mL to 65 ng/mL in 15 minutes. THC had a similar concentration-time profile. For the eight-hour infusion of curcumin at a rate of 1.25 mg/kg/hr (total dose 10 mg/kg), peak plasma concentrations of 187 ng/mL were also reached by 1.5 hours and then began to fall during the infusion period and thus, steady-state levels were not achieved; a similar concentration-time profile was also observed for THC. The ratio of THC to curcumin, based on AUC was 9.6 for the 2-hour infusion and 6.3 for the 8-hour infusion. The drop in plasma levels of both curcumin and its metabolite, THC, upon 8-hr infusion suggests that infusion of curcumin may activate or enhance its own elimination.

Plasma Levels of A) curcumin following a 2-hour infusion of 5 mg/kg/hr curcumin; B) THC following a 2-hour infusion of 5 mg/kg/hr curcumin C) curcumin following a 8-hour infusion of 1.25 mg/kg/hr curcumin; and D) THC following a 8-hour infusion of 1.25 mg/kg/hr curcumin in the presence and absence of phosphoric acid. Values are presented as the mean±standard error of four dogs.
Computer-assisted pharmacokinetic analysis of the plasma concentration data was only possible for the 2-hour infusion. The estimated PK parameters for curcumin and THC are shown in Table III, while the Cmax observed and calculated AUC are shown in Table I. The rapid decrease in plasma concentrations of curcumin is consistent with short t1/2(e) and MRT values of 0.4 and 0.6 hours, respectively, as a result of a high clearance of 20.6 L/kg/hr from a volume of distribution of 12.7 L/kg. The fitted Cmax and AUC values of 233 ng/mL and 485 ng*hr/mL are close to the observed Cmax of 320 ng/mL and calculated AUC of 394 ng*hr/mL. THC had estimated t1/2(e) and MRT values close to those of curcumin with the estimated values being 0.5 and 0.7-hours, respectively with Cmax and AUC values of 2,429 ng/mL and 5,185 ng*hr/mL, compared to the observed values of and 2,983 ng/mL and 3,797 ng*hr/mL. The observed Cmax values for curcumin at infusion dose rates of 1.25 and 5.0 mg/kg/hr were close to be dose-proportional to the dosing rate, with dosing-rate normalized Cmax values (Cmax/Dosing rate in mg/kg/hr) of 64 and 53 ng/mL observed for the two- and eight-hour infusions. The AUDs and infusion dose-rate normalized AUDs up to two hours for the high- and low-infusion rates were 354 and 82 ng*hr/mL and 59 and 66 ng*hr/mL, respectively, also consistent with dose-proportionality.
Measurement of the levels of curcumin and THC in the plasma, urine and bile provide additional information concerning the disposition of curcumin (Figure 2; Table IV). For bile, the levels of curcumin and THC were somewhat higher in females compared to males. At both the high- and low-infusion rate of 1.25 mg/kg/hr, curcumin was found at higher concentrations in the urine and bile compared to the plasma. At the low-infusion rate, the urine and bile to plasma concentration ratios were 10 and 32, respectfully, while at the higher infusion rate, the observed values were 44 and 16, respectfully. These observations suggest that 1) both the liver and the kidney can eliminate curcumin from the plasma and 2) at higher plasma concentrations the kidney can excrete THC by the hepatic and extra-hepatic tissues with accumulation of THC in the plasma and excretion via the urine. These observations suggest that 1) both the liver and the kidney can eliminate curcumin from the plasma and 2) at higher plasma concentrations the kidney can excrete more curcumin while biliary excretion is approaching saturation. This suggestion is consistent with studies in rats where tissue disposition studies of intravenously-administered curcumin demonstrated the highest exposure in the liver and kidney (3). Thus, modulation of renal transporters may play an important role in the enhancement of the elimination of curcumin previously mentioned. For THC the urine to plasma concentrations ratios were higher than the bile to plasma concentration ratios both at the low- and high-infusion rates, with values of 3.1 and 4.4 compared to 0.3 and 1.2, respectively. This observation is consistent with the metabolism of curcumin to THC by the hepatic and extra-hepatic tissues, accumulation of THC in the plasma and excretion via the urine.
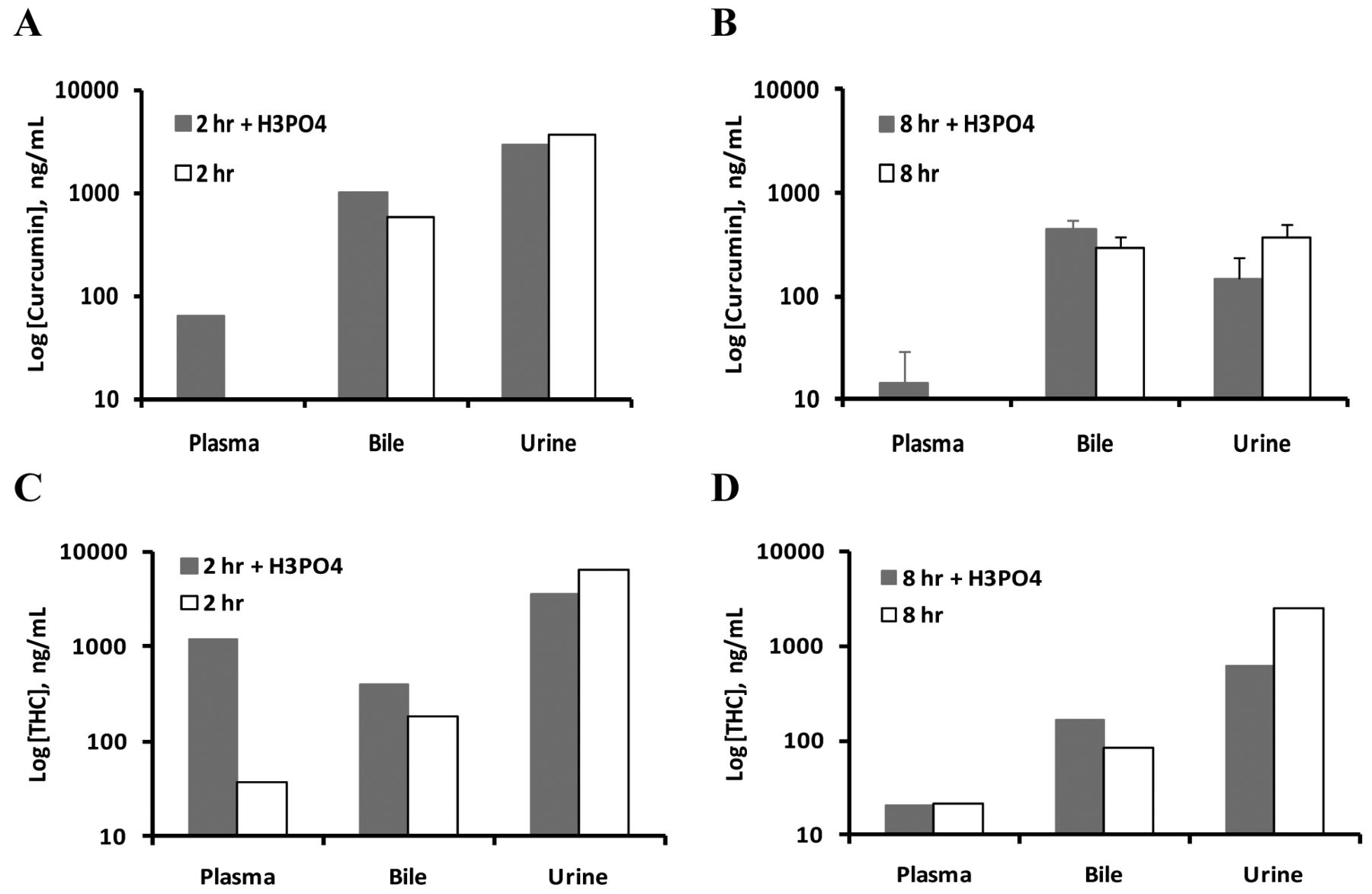
Fifteen minutes post-infusion plasma, bile and urine levels of A) curcumin following a 2-hour infusion of 5 mg/kg/hr curcumin; B) curcumin following a 8-hour infusion of 1.25 mg/kg curcumin; C) THC following a 2-hour infusion of 5 mg/kg/hr curcumin and D) THC following a 8-hour infusion of 1.25 mg/kg/hr curcumin in the presence and absence of phosphoric acid; for THC in the absence of phosphoric acid, the value is presented as the mean±SE of three determinations, otherwise all values are presented as the mean±standard error of four dogs.
Discussion
These data demonstrate drug stability, dose and schedule of administration further representing important and malleable components of curcumin clinical therapeutics. Tissue phenotype, metabolism, excretion routes, transport mechanisms and distribution are important but less subject to modification. Out of these parameters, curcumin degradation prior to and during analytical procedures, is critically important and contributes to the variences and validity of plasma levels reported in animal studies of oral and parenteral curcumin administration. The high succeptibility to ambient light and pH of curcumin was resolved by limiting the exposure of samples to ambient light and the addition of phosphoric acid to stabilize curcumin prior to analytical processing. Another factor contributing to misinformation regarding curcumin blood levels in animal models is the effect of metabolic activity. Curcumin can be released as free curcumin from any of the delivery vehicles and can distribute into tissue lipids because of low aqueous solubility or is metabolized to a number of secondary compounds via conjugation with glucuronides or sulfates, or is reduced to dihydrocurcumin, tetrahydrocurcumin and octahydrocurcumin. However, the specific and collective biological activity of these metabolites in animal models has not been published. The predominant reduced metabolite incorporated in this study appears to be THC. It does have similar biological activity to curcumin (4-8). Conversion to THC by NADH-dependent dihydrocurcumin reductase intestinal E.Coli has been published (9). The conversion to THC from curcumin via this specific enzyme reductase is well-documented. The enzyme has a molecular mass of 82 kDa, consists of two identical subunits and has a restricted substrate spectrum, preferentially acting on curcumin. Its mechanism of action on curcumin is rendered in two steps (two-enzyme reactions). The first is a NADPH-dependent reduction to an intermediate dihydrocurcumin and the second is NADPH-dependent curcumin/dihydrocurcumin reductase to tetrahydrocurcumin. The enzyme is part of the medium chain dehydrogenase-reductase superfamily, and its presence raises intriguing issues of enzyme origins and distribution. It is found in the blood of mice following intraperitoneal administration of curcumin, and it is assumed that the enzyme is present in human tissues: particularly the liver in humans. It is also found in a particular strain of human origin intestinal E.coli: K-12 substr. MG1655 version 15.1. It is unknown whether this enzyme has a metabolic role as a reductase for unknown substrates in E.coli in addition to curcuminoid structures. While there are no published reports on tissue levels of this reducing enzyme in animal models, the significant presence of THC in the plasma of dogs strongly suggests the presence of the enzyme in tissues. In conclusion the addition of phosphoric acid to plasma and bile samples in dogs prevented the degradation of curcumin and THC which raises issues of validity of published data on curcumin distribution and excretion. Infusion of lipocurc™ in dogs at two different infusion rates resulted in higher plasma levels of curcumin and THC with a 2-hour infusion compared to an 8-hour infusion. The Cmax and AUC2 normalized to the infusion dose-rate were proportional. The plasma levels of THC were higher than curcumin with the ratio of plasma THC to curcumin ranging from 6.3-9.6. These data emphasize the putative presence of a curcumin reducing enzyme in blood or tissues. Analysis of the 2-hour curcumin infusion data provided estimates of the plasma t1/2(e) and the mean residence times (MRT) which were short, ranging from 0.4-0.7 hours. The short plasma t1/2(e) and MRT are likely a consequence of the clearance of curcumin by both hepatic and renal routes.
Plasma concentration vs. time for curcumin and THC upon bioanalysis in the presence and absence of phosphoric acid.
Estimated PK parameters of curcumin and THC for a 2 hr intravenous infusion at a dose rate of 2 mg/kg/hr; total dose 10 mg/kg1.
Plasma, urine and bile levels of curcumin and THC 15 minutes post-2- and 8-hour infusion in the presence and absence of phosphoric acid.
Clearances of curcumin and THC at over 8-hour infusions are augmented, preventing attainment of a steady-state. The mechanism may potentially be through modulation of renal transporters. Comparing two- and eight-hour infusion schedules of the same total applied dose in dogs led us to tentatively conclude the two-hour infusion would be preferable for liquid malignancies (10) and the eight-hour infusion for solid tumors in the absence of tumor cell/tissue data.
Acknowledgements
Curcumin(diferuloylmethane), 99.2 % pure and tetrahydrocurcumin was manufactured and supplied by Sabinsa Corporation, Princeton New Jersey.
Footnotes
-
This article is freely accessible online.
- Received July 13, 2012.
- Accepted September 4, 2012.
- Copyright© 2012 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Distribution and Metabolism of Lipocurc™ (Liposomal Curcumin) in Dog and Human Blood Cells: Species Selectivity and Pharmacokinetic Relevance
- Curcumin Promotes Autophagic Survival of a Subset of Colon Cancer Stem Cells, Which Are Ablated by DCLK1-siRNA
- The Molecular Basis for the Pharmacokinetics and Pharmacodynamics of Curcumin and Its Metabolites in Relation to Cancer
- Effect of Liposomal Curcumin on Red Blood Cells In Vitro
- Novel Curcumin Oral Delivery Systems
- Tissue Distribution of (Lipocurc™) Liposomal Curcumin and Tetrahydrocurcumin Following Two- and Eight-hour Infusions in Beagle Dogs