


Abstract
Background: To determine the potential activity and tolerability of sequential treatment in head and neck cancer, we conducted a phase II trial based on induction chemotherapy of two cycles of taxotere, cisplatin and 5-fluorouracil followed by radiotherapy plus weekly cetuximab. Patients and Methods: Thirty-six patients with stage III or IV squamous cell carcinoma of the oral cavity, larynx, oropharynx and hypopharynx were treated and evaluated for response and acute toxicity. Results: Eighty-one percent of patients had stage IV disease and 42% had hypopharyngeal and oral cavity primaries. The overall response rate was 81.8%, with 60.6% complete response and 33.3% partial response. Severe toxicities were febrile neutropenia (6%) during induction chemotherapy and dermatitis (48%), mucositis (33%) and dysphagia (12%) during the concurrent phase. Conclusion: Our protocol proved to be feasible, effective and well tolerated. This sequential strategy should be further investigated.
Current management of locally advanced head and neck squamous cell carcinoma (HNSCC) usually involves the combination of multiple therapies. Several trials showed that concurrent chemoradiotherapy (CT/RT), usually with a cisplatin-based regimen, improves survival rates when compared to radiotherapy (RT) alone (1, 2). However, this survival improvement is associated with increased toxicity (3).
Induction CT based on cisplatin plus fluorouracil could also be a valuable option of RT and CT association, with a survival benefit (4). Large clinical trials (5, 6) subsequently demonstrated that a three-drug regimen consisting of docetaxel, cisplatin and fluorouracil (TPF) is feasible and improves outcome compared with a treatment based on cisplatin and fluorouracil alone; nevertheless, induction chemotherapy might also increase toxicity and compromise the subsequent concurrent CT/RT (7). To reduce toxicity, recently, considerable attention has been focused on the use of cetuximab (Cet), for its efficacy and tolerability with RT (Cet/RT) (8). Thus, while some researchers tested concurrent association of Cet and CT/RT (9), others proposed Cet/RT as a suitable alternative to CT/RT for patients with locally advanced HNSCC (10).
Until 2006, when our study was designed, experiences based on a sequential associated regimen of Cet/RT after induction TPF chemotherapy had never been reported. Consequently, we conducted this phase II trial to assess toxicity and efficacy of a TPF-based neoadjuvant treatment followed by Cet/RT for patients with locally advanced HNSCC.
Patients and Methods
Patients were required to have non-metastatic, histologically proven, stage III or IV squamous cell carcinoma of the oral cavity, larynx, oropharynx and hypopharynx; age between 18 and 75 years old; measurable disease according to World Health Organization criteria (11); an Eastern Cooperative Oncology Group Performance Status 0-2; adequate haematological, hepatic, cardiac and renal functions. Exclusion criteria were: distant metastases, previous malignancy or previous CT and/or RT.
The study protocol consisted of two courses of induction chemotherapy (ICT) followed by RT concomitant with weekly Cet.
ICT consisted of docetaxel at a dose of 75 mg/m2 intravenously (i.v.), cisplatin at a dose of 25 mg/m2 i.v. on days 1 to 3; and fluorouracil at a dose of 250 mg/m2 per day, as an i.v. bolus, on days 1 to 3 every 21 days. After completion of the ICT, an interval of 21 days was scheduled before the loading dose of Cet (400 mg/m2 i.v. in 120 min) that was delivered 1 week before the start of RT. Weekly Cet (250 mg/m2) was administered during RT for at least six weeks. No Cet dose modification was allowed.
A conformal (3D-CRT) or intensity-modulated (IMRT) RT treatment was delivered using a 5 or 6 MV linear accelerator. The prescribed mean dose was 70 Gy to clinical target volume including the primary tumour and the metastatic lymph nodes. The uninvolved lymph nodes were treated with a mean dose of 56 Gy (50-66 Gy). The daily dose fraction was 1.8 or 2 Gy for 5 days per week. Surgery was planned for patients who had resectable residual disease after CT/RT.
Staging modalities were clinical examination, endoscopy, computed tomographic scan and/or magnetic resonance imaging. CT-PET was performed when clinically indicated. Baseline evaluation included a complete medical history, clinical examination and nutritional evaluation. All patients were offered dental prophylaxis. Toxicity assessments were performed weekly during the study and acute toxic effects were graded according to the Radiation Therapy Oncology Group (RTOG) toxicity criteria.
Tumor responses after ICT and 8-12 weeks after CT/RT were assessed according to WHO criteria (11). Patients were monitored for recurrence every 2 months for 2 years, and computed tomographic scans were performed every 4 months. From year 3 to 5 post diagnosis, patients underwent a clinical examination every 4 months and computed tomographic scans every 6 months.
Statistical analysis. The primary end point of the trial was efficacy, as measured by the objective response rate at the end of the whole treatment. Sample size and decision criteria were calculated with a two-stage design method, to minimize the accrual into a protocol unacceptable for low clinical response or high toxicity rate (12). In the first stage, after testing the treatment on 12 patients, the study would be stopped if 8 or fewer responses were observed, or 6 or more patients experienced unacceptable toxicity (i.e. early discontinuation of treatment or treatment-related death). If the second stage of the study was reached, a total of 32 patients would be enrolled to detect at least 23 (72%) objective responses and an unacceptable toxicity in 18 patients (56%) or fewer (αR=0.10, αT=0.15, (1-β)=85%). Assuming 10% non-evaluable patients, a total of 36 patients were enrolled.
Local and locoregional control rates (LC, LRC), progression-free survival (PFS) and overall survival (OS) analyses were performed. Time to disease progression, LC and LRC were calculated from the date of initial diagnosis until the first imaging or histological diagnosis of relapse. PFS was intended as time to relapse at any site, whether locoregional or distant. OS was calculated from the date of primary diagnosis until death or last date of follow-up. At the time of analysis, patients who were not reported as having died were censored at the date they were last known to be alive.
The median response duration and OS were calculated using 95% confidence intervals (CI). Statistical calculations were performed using STATA software (Stata Statistical Software: Release 11.0; Stata Corporation, College Station, TX, USA). Descriptive statistics, including mean, standard deviation, median, range, and percentage, were used to describe patient demographics, pathological, and clinical characteristics. Comparisons were performed using chi-square and Fisher test. Survival curves were generated using Kaplan-Meier method. Results were considered significant for p<0.05.
Patient and tumour characteristics (N=36).
Results
From November 2007 to November 2009, 36 patients were enrolled onto this phase-II trial from 6 centres in Italy. Patients' characteristics are summarized in Table I. Most patients (97.2%) completed two cycles of ICT, but dose reductions were required for four patients due to hematological toxicity, while one patient experienced G4 hepatic toxicity after the first cycle and received no further chemotherapy treatment. Overall, 85.7% (30/35) of patients received the intended dose of chemotherapy.
Three patients were unable to enter the post-induction phase (Cet/RT) and were subsequently treated off-protocol: one patient developed a second primary tumour after ICT and was excluded from the evaluation of response rates and toxicity; in the second, study treatment was interrupted due to severe hepatotoxicity and in the third due to progressive disease (PD) after ICT. Therefore, 33 patients started RT and were evaluable for response to the Cet/RT regimen.
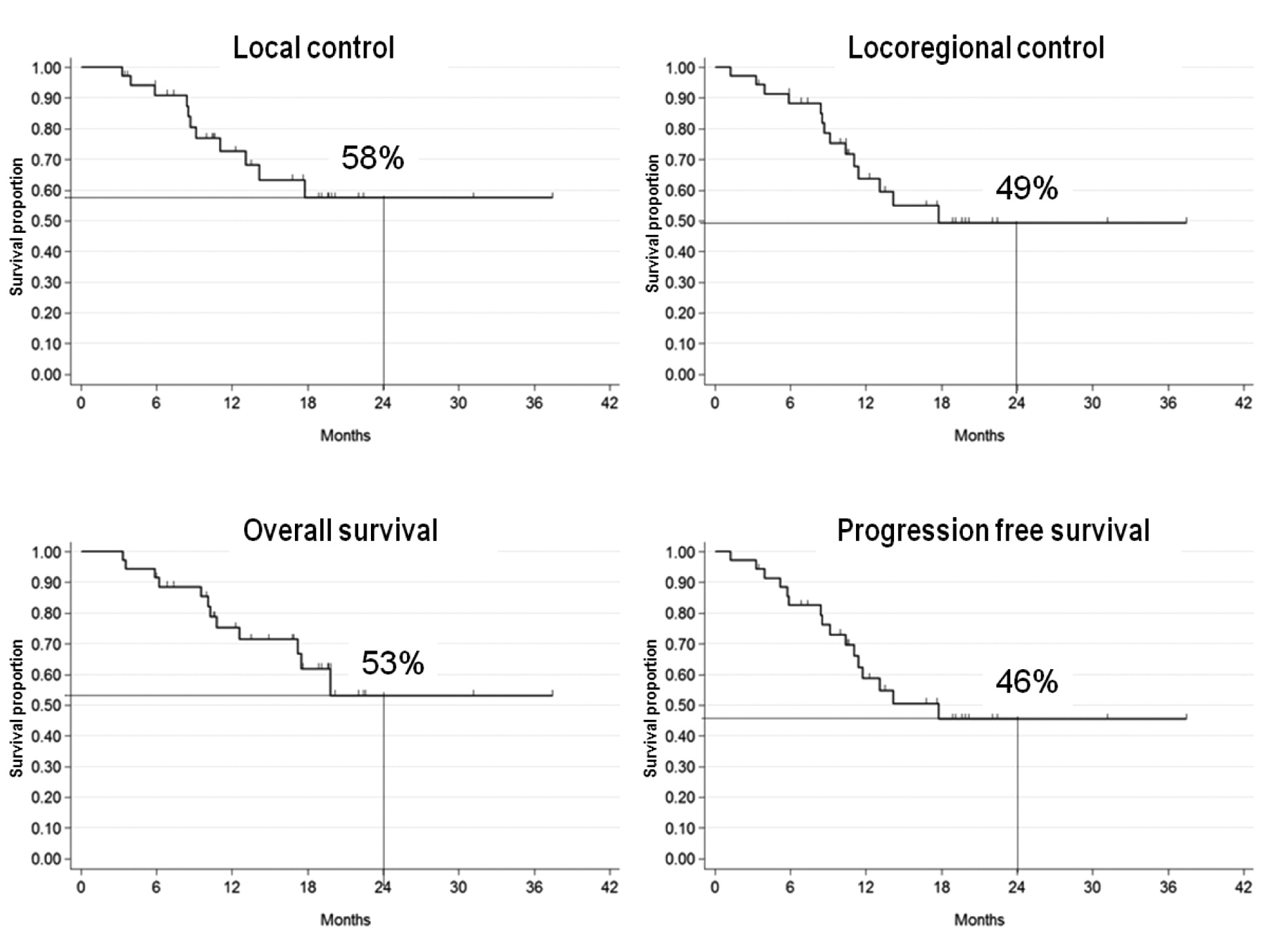
Kaplan-Meier estimates of 24-month actuarial local control, locoregional control, overall survival and progression-free survival after TPF and Cet/RT.
Twenty-seven patients (82%) were treated with 3D CRT, five patients (15%) with IMRT and one patient (3%) was treated with initial 3D CRT followed by an IMRT boost. Thirty-two out of 33 patients completed the whole RT treatment as one patient died due to sepsis at a total dose of 64 Gy. Only two patients out of these 32 required more than three days of RT interruption, due to severe mucositis.
Thirty patients out of 33 (91%) received Cet/RT as planned. Hypersensitivity reactions and severe acneiform rash were responsible for Cet discontinuation.
After ICT, the overall response rate (ORR) in 35 evaluable patients was 82.8% (95% CI=66.4%-93.4%) (Figure 1) with 5.7% of complete response (CR), 77.1% of partial response (PR), 11.4% of stable disease (SD) and 2.8% PD.
After Cet/RT, 33 patients were evaluable. The ORR was 81.8% (95% CI=66.4%-93.4%) with 48.5% of CR, 33.3% PR, 6.1% of SD and 6.1% PD. Two patients (6.1%) were not assessable: one due to an early death and one who was lost to follow-up. Five patients out of 11 with PR underwent salvage surgery achieving four (12.2%) consequent CR and one (3%) PD. Overall, 60.6% (95% CI=44.8%-74.9%) of patients (20/33) achieved a CR to protocol.
Twenty-four months actuarial LC and LRC rates were 57.5% (95% CI=35.2%-74.5%) and 49.4% (95% CI=28.7%-67%), respectively, with a median follow-up of 17.5 months (range: 4-35 months). Twenty-four-month OS and PFS rates were 53% (95% CI=28.9%-72.3%) and 45.5% (95% CI=26.2%-62.9%), respectively. Survival curves using Kaplan-Meier methods are shown in Figure 1.
Four patients (11%) developed distant metastases (three in lung and one in lung plus bone); two of these patients also developed local relapse. Eleven patients (31%) died: 9 (26%) due to PD, 1 due to cerebrovascular accident and 1 due to sepsis.
During TPF therapy, grade G≤2 anaemia and thrombocytopenia affected 47% and 22% of patients, respectively; G3-4 neutropenia was observed in 31.4% of patients, febrile neutropenia in 5.7%. We have already reported on the case of severe hepatic toxicity that caused CT withdrawal. There was one case of severe allergic reaction to the loading dose of Cet. During Cet/RT severe adverse events consisted of G3 acneiforme rash (6%), nail toxicity (6%), G3 radiodermatitis (48%), G3 mucositis (33%), and G3 dysphagia (12%). A mild folliculitis (G1-G2) affected 82% of patients, and G ≤2 anaemia was recorded in 16 cases. In 18% of patients, there was a modest weight loss (of up to 5% of initial body weight), while a greater weight loss (5-10%) was observed in six patients. All patients received oral nutritional support with dietary supplements and only for one patient percutaneous endoscopic gastrostomy was required for enteral feeding.
Discussion
Our trial can thus be considered successful because we achieved 81.8% ORR after the whole protocol and severe toxicity rate was maintained under 50%, in line with the statistical endpoints. Infact, the most relevant severe toxicity rate was observed during concomitant phase and it was G3 radiodermatitis, detected in 48% of patients. The ORR of ICT was historically near 60% with two drug regimens (cisplatin plus fluorouracil), and became higher than 70% in TPF-based schedule such as in Posner et al.'s study (5); thus our results of 82.8% of ORR after ICT with only two cycles of TPF can be considered satisfactory.
In line with our findings, several other researchers (13-16) reported a similar acute toxicity profile for Cet/RT treatment, even though Bonner et al. (8) observed fewer G3-G4 in-field skin reactions (35%). It is, however, necessary to stress that clinical scoring of skin reaction is a very sensitive point. In our experience, advanced medications and systemic antibiotic obtained rapid healing of severe skin lesions with no residual scars and few RT interruptions (17).
Some authors proposed Cet/RT as a feasible alternative to CT/RT (10), while the concurrent use of Cet and CT/RT, although with a high activity rate (70%-90%), was associated with severe toxicity (9, 18). We chose the sequential approach of TPF-based ICT followed by Cet/RT and, in order to increase compliance, we decided to use only two cycles of TPF as, when this study was designed, no experiences had been reported on this schedule. Moreover, to reduce toxicity, it is unclear whether it is better to reduce the induction (19) or the post-induction phase (20), or to tune them on the basis of predictive factors (21). The post-induction ORR (82.8%) obtained in our study was similar to those of other authors who adopted more intensive ICT (5, 6, 22), whereas the post-induction CR rate was lower [5.7% in our study vs. 8.5% by Vermorken et al. (6) and 17% by Posner et al. (5)]. However, the final CR rate in our study was 48.5%, comparable with the results of more intensive TPF regimens. The reduced toxicity of the treatment might have allowed a better compliance: indeed, in our trial, 32/35 (91.4%) patients completed the whole protocol, while in other trials, only 79.2% and 88% did (5, 6). In fact, OS and PFS were inferior to those reported in trials with more intensive TPF schedules: Posner et al. and Paccagnella et al. reported two-year OS and PFS of 67% and 53%, and of 61% and 55.6%, respectively (5, 23). However, the shorter follow-up time of our patients does not allow definitive conclusions to be drawn.
Conclusion
Our protocol can be considered feasible, effective and well tolerated due to an encouraging response rate and a manageable toxicity pattern, such that it constituted the basis for an ongoing multicentric phase III trial (24) that will investigate the role of ‘standard’ concomitant CT/RT versus three TPF cycles followed by RT and Cetuximab.
Acknowledgements
We thank Dr. G. Rossi for his careful contribution to data collecting and analysis.
- Received October 12, 2011.
- Revision received November 14, 2011.
- Accepted November 15, 2011.
- Copyright© 2012 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}