


Abstract
Aim: To assess the relationship between the timing of radiotherapy and the risk of local failure in patients with endometrioid–type endometrial cancer who had undergone surgery and adjuvant external pelvic radiotherapy (with or without brachytherapy), but not chemotherapy. Patients and Methods: One hundred and seventy seven patients were analyzed in this study. The median follow-up of the survivors was 72 months. Results: Radiotherapy was delivered after a median time of 14.6 weeks from surgery and the median overall treatment time was 6.4 weeks. The tumor relapsed in 32 (18.1%) patients after a median time of 21 months. The local recurrence (vaginal or central pelvic) occurred in 11 patients. The local recurrence rate was associated with tumor grade (p=0.02), myometrial invasion (p=0.046), FIGO stage (p=0.003), pathological node status (p=0.037) and time interval from surgery to radiotherapy using 9 weeks as the cut-off value (p=0.046), but not with the overall treatment time. All the local relapses occurred in patients who received adjuvant irradiation after an interval from surgery >9 weeks. Conclusion: The time interval from surgery to radiotherapy might affect the local recurrence rate in patients not receiving chemotherapy. Every possible effort should be made to start radiotherapy within 9 weeks, when radiotherapy only is deemed necessary as adjuvant treatment.
Endometrioid carcinoma, which accounts for approximately 85-90% of all endometrial malignancies, is usually associated with a good clinical outcome. FIGO stage, tumor grade, depth of myometrial invasion and lymph node status are the strongest clinical-pathological prognostic variables (1-3). Surgery is the cornerstone of the treatment, and consists of laparotomy, peritoneal washing, total hysterectomy and bilateral salpingo-oophorectomy with or without lymph node dissection, although laparoscopic or robotic-assisted laparoscopic hysterectomy appears be a safe and effective alternative surgical approach (4, 5). The recurrence rates range from 11 to 23%, the sites of relapse are equivalently distributed between loco regional and distant, and most failures develop within 3 years (6-10). Poor histological differentiation and deep myometrial invasion have been reported to be predictors of local recurrence (1, 6). External pelvic radiotherapy significantly reduces loco regional recurrences without improving survival and offers a benefit in terms of clinical outcome only in patients with both deep myometrial invasion and poorly differentiated grade (11-18).
A retrospective cohort investigation on a large series of breast cancer patients aged over 65 years, who received conservative surgery and radiotherapy, but not chemotherapy, showed a continuous relationship between the interval from surgery to radiotherapy and the risk of local recurrence (19). On the other hand, the cumulative analysis of 963 patients, included in three International Breast Cancer Study Group trials, treated with breast-conservative surgery, radiotherapy and adjuvant endocrine therapy, revealed that the timing of radiotherapy was not significantly associated with the interval to local recurrence, after adjusting for age, menopausal status and estrogen-receptor status (20). Published data on the clinical relevance of the timing of adjuvant radiotherapy in endometrial cancer are not currently available. Therefore, the aim of this retrospective mono-institutional study was to assess the relationship between the timing of radiotherapy and the risk of local failure in patients with endometrioid–type endometrial cancer who had undergone surgery and adjuvant external pelvic radiotherapy but not chemotherapy .
Patients and Methods
The present retrospective analysis included 177 patients who had undergone adjuvant external pelvic irradiation following total hysterectomy and bilateral salpingo-oophorectomy for endometrial cancer between 1987 and 2009. All the patients had been referred to the multidisciplinary Committee of Gynecologic Oncology of the Pisa University Hospital. Eighty-one patients had histologically proven negative lymph nodes after pelvic and/or para-aortic lymph node dissection (negative pathological node status) and 96 patients had not undergone any lymph node dissection (unknown pathological node status). Patients with histologically proven positive pelvic and/or para-aortic lymph nodes, patients who had undergone adjuvant sequential and/or concomitant chemotherapy and/or para-aortic irradiation and patients who were lost to follow-up were excluded from the present analysis.
Surgery was performed by laparotomy in 145 patients, laparoscopy or robotics in 7 and the vaginal route in 25. The patients were staged retrospectively according to the International Federation of Gynecology and Obstetrics (FIGO) classification 2009 (21). The histological classification was performed according to the World Health Organization classification (2). The architectural grade was defined as: G1, ≤5%, G2, 6-50% and G3, >50% of non-squamous or non-morular solid growth pattern. Notable nuclear atypia, inappropriate for the architectural grade, raised the grade of G1 or G2 tumors by one grade.
External beam irradiation was performed with a 15 MV beam and with a four-field technique (gantry angles at 0°, 90°, 180°and 270°). A 45-50.4 Gy dose was given in daily fractions of 1.8 Gy. The pelvic target volume was outlined on a CT scan. Radiotherapy prescription had changed during the observation period. Vaginal cuff high-dose rate (HDR) brachytherapy was added in selected cases with histmus or stromal cervical involvement after external beam irradiation with a cylinder applicator. The treatment planning was performed on a CT scan. The prescribed dose was 10-15 Gy in 5 Gy fractions. Rectal and bladder doses were estimated from a dose volume histogram on the CT based plan and were evaluated to the dose points specified by the International Commission on Radiation Unit and Measurements.
The patients were periodically followed until February 2011 or until death. The median follow-up of survivors was 72 months (range, 8-273 months)
Statistical analysis. Patient age, tumor grade, myometrial invasion, FIGO stage, pathological node status, overall treatment time and time interval between surgery and the start of external beam irradiation were analyzed for association with local recurrence risk, progression-free survival and overall survival. Peritoneal, hematogenous and lymph node recurrences outside the retroperitoneal area were considered as distant failures.The SAS statistical package (release 8.2, SAS Institute, Cary, NC, USA) was used for the computations. The rate of recurrences was compared to the explicative variables using Pearson's chi-square test (or two-tailed Fisher's exact test when appropriate). The time from surgery to recurrence was defined as disease-free survival. The time from surgery to death of disease or last observation was defined as cause-specific survival. The cumulative probability of disease-free survival and cause-specific survival were estimated by the product-limit method. The log-rank test was used to compare the homogeneity of disease-free survival and cause-specific survival functions across strata defined by categories of prognostic variables. Values of p<0.05 were considered as being significant.
Results
The median age of the women was 62 years (range, 34-80 years). The FIGO stage was Ib in 147 (83.0%) patients, II in 21 (11.9%), IIIa in 5 (2.8%) and IIIb in 4 (2.3%), respectively. The tumor grade was G1 in 38 (48.0%) cases, G2 in 85 (21.5%), and G3 in 54 (30.5%). Myometrial invasion was ≤50% in 42 (23.7%) women and >50% in 135 (76.3%). As far as the 81 patients who had undergone lymph node dissection are concerned, the median number of removed nodes was 16 (range, 2-52).
External beam irradiation was delivered after a median time of 14.6 weeks (range, 3 to 33 weeks) from surgery. Forty-two (23.7%) women started radiotherapy within 9 weeks from surgery. The median overall treatment time for external beam irradiation was 6.4 weeks (range, 5-8.4 weeks). Vaginal cuff brachytherapy was delivered to 32 (18.1%) patients within two weeks following the completion of external beam irradiation.
The tumor relapsed in 32 out of the 177 (18.1%) patients. The median time from surgery to recurrence was 21 months (range, 7-129 months). Recurrence sites were: local in 3 cases (vaginal in 1, central pelvic in 2), distant in 16, para-aortic lymph nodal in 3, para-aortic lymph nodal plus distant in 2, local (3 vaginal and 5 central pelvic) plus distant in 8. Therefore, recurrent disease involved the vagina or central pelvis in 11 (6.2%) patients, distant sites in 26 (14.7%), and the para-aortic lymph nodes in 5 (2.8%). Twenty-two (12.4%) women died of tumor after a median time of 27 months from surgery (range, 12-109 months). Ten (5.6%) women died of unrelated causes after a median time of 158 months (range, 34-212 months).
The local recurrence rate was associated with tumor grade (p=0.02), myometrial invasion (p=0.046), FIGO stage (p=0.003), pathological node status (p=0.037) and time interval from surgery to radiotherapy using 9 weeks as the cut-off value (p=0.046), but not with patient age, overall treatment time and time interval from surgery to radiotherapy using 14.6 weeks as the cut-off value (Table I).
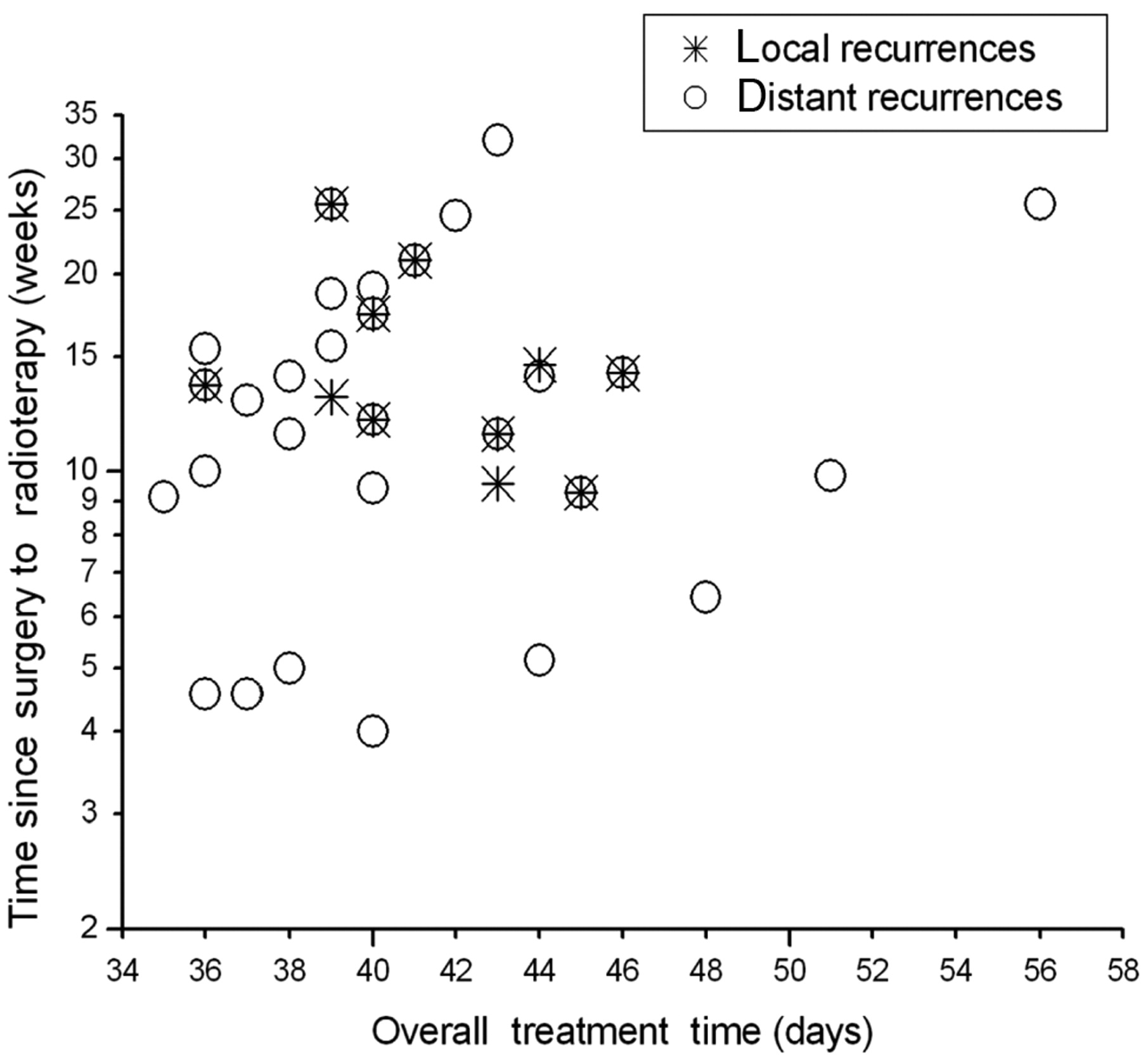
Figure 1 shows the distribution of recurrences according to the overall treatment time and time interval from surgery to radiotherapy. All the local relapses occurred in those patients who received adjuvant irradiation after an interval from surgery longer than 9 weeks, whereas the distant recurrences were not related to the time elapsed from surgery to radiotherapy.
Local recurrence rate according to clinical-pathological variables (11 patients).
The 5 and 10-year disease-free survival rates were 81.0% and 78.5%, respectively. Disease-free survival was significantly associated with tumor grade (p=0.002) and FIGO stage (p=0.042) (Table II).
The 5-year and 10-year cause-specific survival rates were 87.1% and 83.4%, respectively
Cause specific survival was significantly associated with tumor grade (p=0.004) (Table III).
Discussion
A meta-analysis of four randomized trials enrolling 1770 patients showed that external pelvic radiotherapy following surgery significantly reduced the loco regional recurrence rate, with a relative risk (RR) reduction of 72% (95% confidence interval [CI]=56-83%, p<0.00001) (11-15). However, there were no statistically significant differences between the patients who had radiotherapy and those who had not as far as distant metastases, endometrial cancer-related deaths and deaths from all causes were concerned. The analysis of the subset of patients with both G3 differentiation and myometrial invasion greater than the half revealed a trend towards a reduction in the risk of death from all causes (RR=0.76; 95% CI=0.49-1.19) and of endometrial carcinoma-related death (RR=0.65; 95% CI=0.38-1.44) for the patients who received external radiotherapy, although the differences were not statistically significant. Another meta-analysis, including data from the reported four trials and from another US trial of preoperative radiotherapy (16), led to similar conclusions (17).

Distribution of local and distant recurrences according to overall treatment time and interval from surgery to radiotherapy.
To our knowledge, no clinical investigation has assessed the relationship between the time interval from surgery to adjuvant radiotherapy and the risk of local recurrence in patients with endometrial cancer. In the present study the local recurrence rate was significantly associated with tumor grade, myometrial invasion, FIGO stage and pathological node status in agreement with literature data (1-6). It is noteworthy that disease recurred locally in none of the 42 patients who received radiotherapy after an interval from surgery of <9 weeks compared with 11 out of the 135 (8.1%) patients who received radiotherapy later (p=0.046). Conversely, the overall treatment time had no significant impact on local recurrence rate.
External pelvic radiotherapy, with or without brachytherapy, is often used as adjuvant treatment in patients with intermediate- or high-risk endometrial cancer (11-15, 17, 18). The retrospective, non-randomized nature of the present study and the limited number of events do not allow definitive conclusions to be drawn about the clinical relevance of the time elapsed from surgery to adjuvant radiotherapy. However, the observation that all the local relapses occurred in patients who received radiotherapy after an interval longer than 9 weeks suggests that every possible effort should be made to start radiotherapy within this time frame, when radiotherapy only is deemed necessary as adjuvant treatment.
Variables predictive of disease-free survival by log-rank test.
Variables predictive of cause-specific survival by log-rank test.
- Received August 30, 2011.
- Revision received November 25, 2011.
- Accepted November 28, 2011.
- Copyright© 2012 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}