


Abstract
Background: Metallothioneins (MTs) are low molecular weight proteins present both in normal and neoplastic cells. They protect cells from the effects of heavy metals and from damage induced by free radicals. MT bind heavy metals, exert an anti-apoptotic effect and stimulate proliferation of neoplastic cells. The role of MTs in carcinogenesis has not been fully clarified yet. This study aimed at the evaluation of the intensity of metallothionein (MT-I/II) expression in various histological types of non-small cell lung cancer (NSCLC) and correlation of the expression intensity with clinical/pathological parameters and Ki-67 and minichromosome maintaince protein 2 (MCM-2) proliferation markers. Patients and Methods: The studies were performed on archival material, originating from 145 patients, 105 men and 40 women (65 adenocarcinomas, 67 squamous cell carcinomas, 13 large cell carcinomas). Results: A positive correlation was noted between expression of MT-I/II and expressions of Ki-67 (r=0.1863, p=0.0248) and MCM-2 (r=0.1766, p=0.0336) in NSCLC overall. The most pronounced expression of MT-I/II was noted in the large cell carcinomas. The expression of MT-I/II was significantly lower in the adenocarcinomas than in the squamous cell carcinomas (p=0.0028) and large cell carcinomas (p=0.0485). The expression of MT-I/II showed no differences related to individual degrees of NSCLC malignancy. Univariate analysis demonstrated no significant differences in overall survival related to the expression intensity of MT-I/II, Ki-67 or MCM-2, but the survival of the patients with high expression of MT-I/II and Ki-67 in the neoplastic cells, as compared to low expression of MT-I/II and Ki-67, was shorter (the difference approached statistical significance, p=0.067). Conclusion: MT-I/II expression is evident in proliferating NSCLC neoplastic cells, pointing to the prognostic importance of parallel expression of MT-I/II and Ki-67.
Both in Poland and all over the world, lung cancer represents the most frequent cause of death due to neoplastic disease, is the most frequent malignant tumour in men and despite advances in diagnosis and treatment, the prognosis remains unfavourable, with fewer than 15% of patients surviving more than 5 years (1, 2).
Metallothionein (MT) was isolated for the first time over 50 years ago (3). It is an intracellular, low molecular weight protein (6-7 kDa), with high cystein content, which permits the protein to bind metals indispensable for the body, such as zinc and copper, and toxic metals, e.g. cadmium, lead and mercury (4). MTs are broadly expressed in eukaryotic cells and depending upon the cell type are responsible for the homeostasis of zinc and copper and protect the cells from oxidative stress by inactivating reactive oxygen species (5, 6). The role of MTs in the process of carcinogenesis is not fully clarified but MTs are involved in processes such as proliferation, apoptosis and resistance to certain chemotherapeutic agents e.g. cisplatin (7-13). MT-I and M-II are present in majority of normal tissues, as well as in neoplastic cells (9, 14). In some tumours, increased expression of MT-I/II correlates with shorter survival of patients (8, 9, 14-17). Nevertheless, few studies have investigated the correlation between MT expression and known clinical/pathological variables or proliferations markers, particularly in cases of non-small cell lung cancer (NSCLC) (9, 16, 18).
Patient and tumour characteristics.
Ki-67 is a non-histone protein, binding DNA, and is manifested mainly in late G1, S, G2 and M-phases of the cell cycle, and is one of the most frequently employed markers of proliferation. However, some studies aimed at determining its value as a proliferation marker have yielded controversial results (17, 19). Minichromosome maintenance 2 (MCM-2) is one of six proteins (MCM-2 to -7) comprising the MCM family. MCM proteins are responsible for initiation and support of the replication process, suggesting that they might serve as a valuable marker of proliferation and indicator of prognosis in human tumours (20-24). However the significance of MCM-2 expression in NSCLC has only been analysed in three investigations (25-27).
Until now, no studies have examined the expression of MTs in parallel with the expression of these proliferation markers. Therefore, the present study aimed at the evaluation of MT-I/II expression intensity in individual histological types of NSCLC and correlation of the expression with recognized clinical/pathological parameters, including expression of Ki-67 and MCM-2 proteins.
Patients and Methods
Patients. The studies were performed on archival material originating from patients (105 men and 40 women), sampled during surgical resection of NSCLC in 1999-2009 in the Lower Silesia Centre of Pulmonary Diseases in Wroclaw and included 65 adenocarcinomas, 67 squamous cell carcinomas (SCC) and 13 large cell carcinomas. The clinical data of the patients were obtained from the hospital archives. The mean observation time was 28.93±38.00 (range: 1-145) months. The mean diameter of the excised tumours was 4.37±1.98 (range: 0.5-10) cm. The clinical and pathological data of the examined patients are presented in Table I. The study was approved by the Commission of Bioethics at Wroclaw Medical University.
Immunhistochemistry (IHC). The isolated tumour samples were fixed in 10% buffered formalin, dehydrated and embedded in paraffin. The paraffin sections, stained with haematoxylin/eosin (HE) were used to verify the diagnosis and degree of tumour malignancy and for determining the presence or absence of necrosis. The IHC reactions were performed on 4-μm-thick paraffin sections fixed to microscopic slides (SuperFrost+, Menzel Glässer, Braunschweig, Germany). In short, deparaffinization and antigen retrieval were performed in Antigen Retrieval Solution (pH 9.0, 97°C, 20 min; DakoCytomation, Glostrup, Denmark). Subsequently, the sections were washed in TBS buffer and incubated with primary antibodies: anti-Ki-67 (clone MiB-1; DakoCytomation), anti-MT-I/II (clone E9; DakoCytomation) and anti-MCM-2 (NCL-MCM2, Leica/Novocastra, Newcastle upon Tyne, UK) in a Dako Autostainer Link48 for 20 min at room temperature. EnVison FLEX (DakoCytomation) reagents were used for visualization of all the studied antigens and the slides were counterstained with haematoxylin, as recommended by the manufacturer. The IHC reactions were accompanied by the negative control. Cases with absence of Ki-67 and MCM-2 expression were subjected to repeated staining with positive control (another tumour tissue) in order to exclude a reaction error.

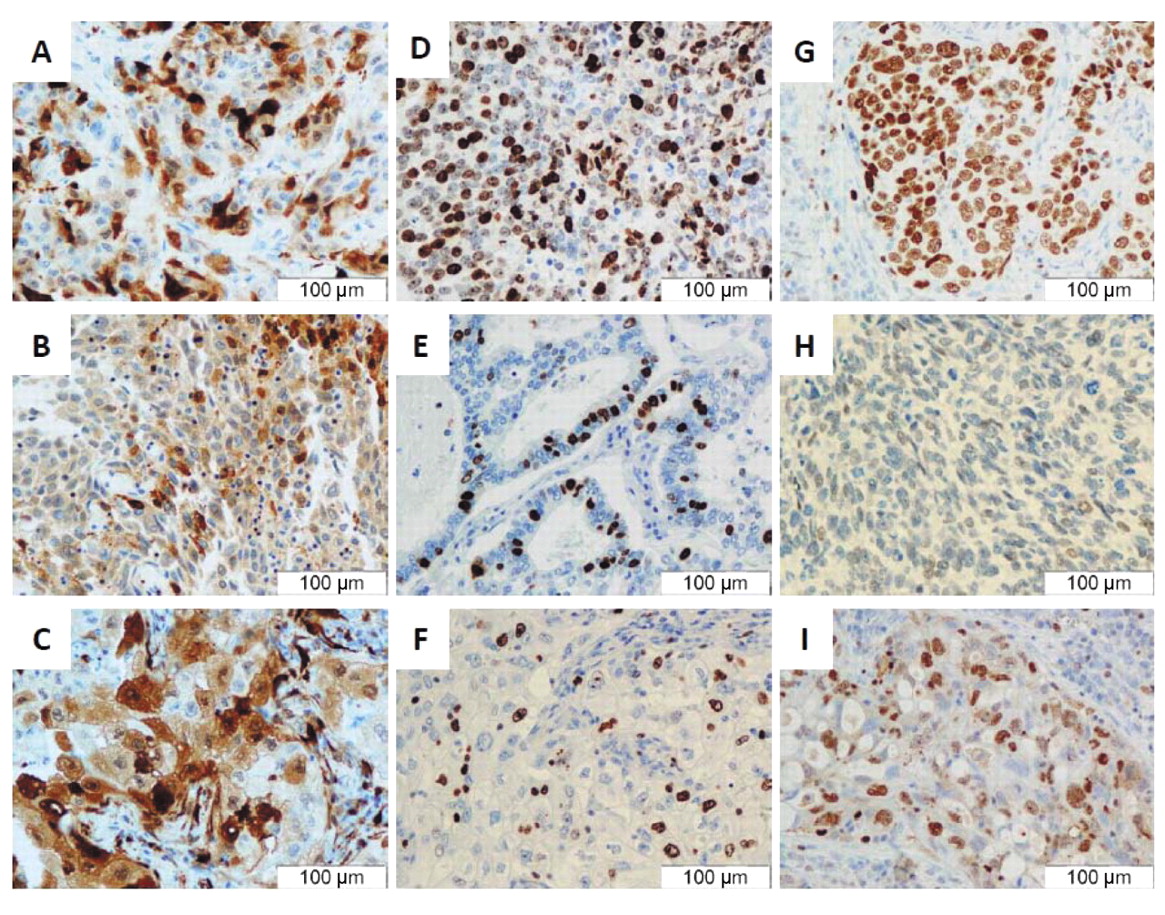
Representative expression of MT-I/II (A-C), Ki-67 (D-F) and MCM-2 (G-I) in different histological subtypes of NSCLC: squamous cell carcinoma (A, D, G), adenocarcinoma (B, E, H) and large cell carcinoma (C, F, I); magnification ×200.
Evaluation of IHC reaction. IHC reactions were analysed under a BX-42 light microscope (Olympus, Tokyo, Japan). Expression of MT-I/II was evaluated using a 12-point semi-quantitative immunoreactive score (IRS), according to Remmele and Stegner (28). Briefly, the percentage of cells with positive reaction is taken into account (0 points: absence of cells with positive reaction, 1 point: 1-10% cells, 2 points: 11-50%, 3 points: 51-80%, 4 points: over 80% cells with positive reaction), as well as intensity of the reaction (0: no reaction, 1: low intensity of the reaction product, 2: moderate intensity of the reaction colour, 3: intense colour of the reaction). Expression of Ki-67 and MCM-2 was evaluated considering proportion of cells with reaction product: (0 points: absence of the reaction, 1: 1-10% cells with positive reaction, 2: 11-25%, 3: 26-50%, 4 points: over 50% cells with positive reaction).
Statistical analysis. For statistical analysis Prism 5.0 (GraphPad, La Jolla, CA, USA) was used. Correlations between the clinicopathological parameters and expression of the studied markers were analysed by Fisher's exact test. The Mann-Whitney U-test and Kruskall-Wallis test were used to compare the groups of data that failed to satisfy the assumptions of the parametric test. Survival times were determined by the Kaplan-Meier method and the significance of the differences was determined by a log-rank test. For each variable, the hazard ratio (HR) and 95% confidence interval (95% CI) were estimated. In all the analyses, the results were considered statistically significant when p<0.05.
Expression scores of MT-I/II, Ki-67 and MCM-2 in histological subtypes of non-small cell lung cancer in relation to grade of malignancy.
Results
Cytoplasmatic/nuclear expression of MT-I/II was observed in 101 (69.7%) cases out of the 145 examined tumours (Figure 1A-C). Nuclear expression of Ki-67 antigen was demonstrated in all the examined cases (Figure 1D-F), while nuclear expression of MCM-2 protein was noted in 127 (87.6%) cases (Figure 1G-I). In the negative cases repeated IHC reaction did not demonstrate expression of MCM-2. The expression of these proteins in the individual types of NSCLC is summarized in Table II.
Spearman's rank correlation test showed positive correlation between the expression of MT-I/II in NSCLC and the expression of Ki-67 antigen (r=0.1863, p=0.0248) and MCM-2 antigen (r=0.1766, p=0.0336). A pronounced positive correlation was also documented between expressions of Ki-67 antigen and MCM-2 antigen (r=0.6950, p<0.0001). In the case of SCC, the only significant correlation involved expression of Ki-67 antigen and MCM-2 antigen (r=0.7483, p<0.0001), as no correlation was detected between MT-I/II expression and the two proliferation markers. In adenocarcinoma, on the other hand, positive correlation was revealed between MT-I/II and Ki-67 (r=0.2672, p=0.0314) and significant, positive correlation between the expressions of the proliferation markers (Ki-67, MCM-2) (r=0.7483, p<0.0001). In large cell carcinoma, statistical analysis demonstrated only a pronounced correlation between the expressions of Ki-67 and MCM-2 proteins (r=0.7989, p=0.0011), as no such correlation was noted for MT-I/II expression.
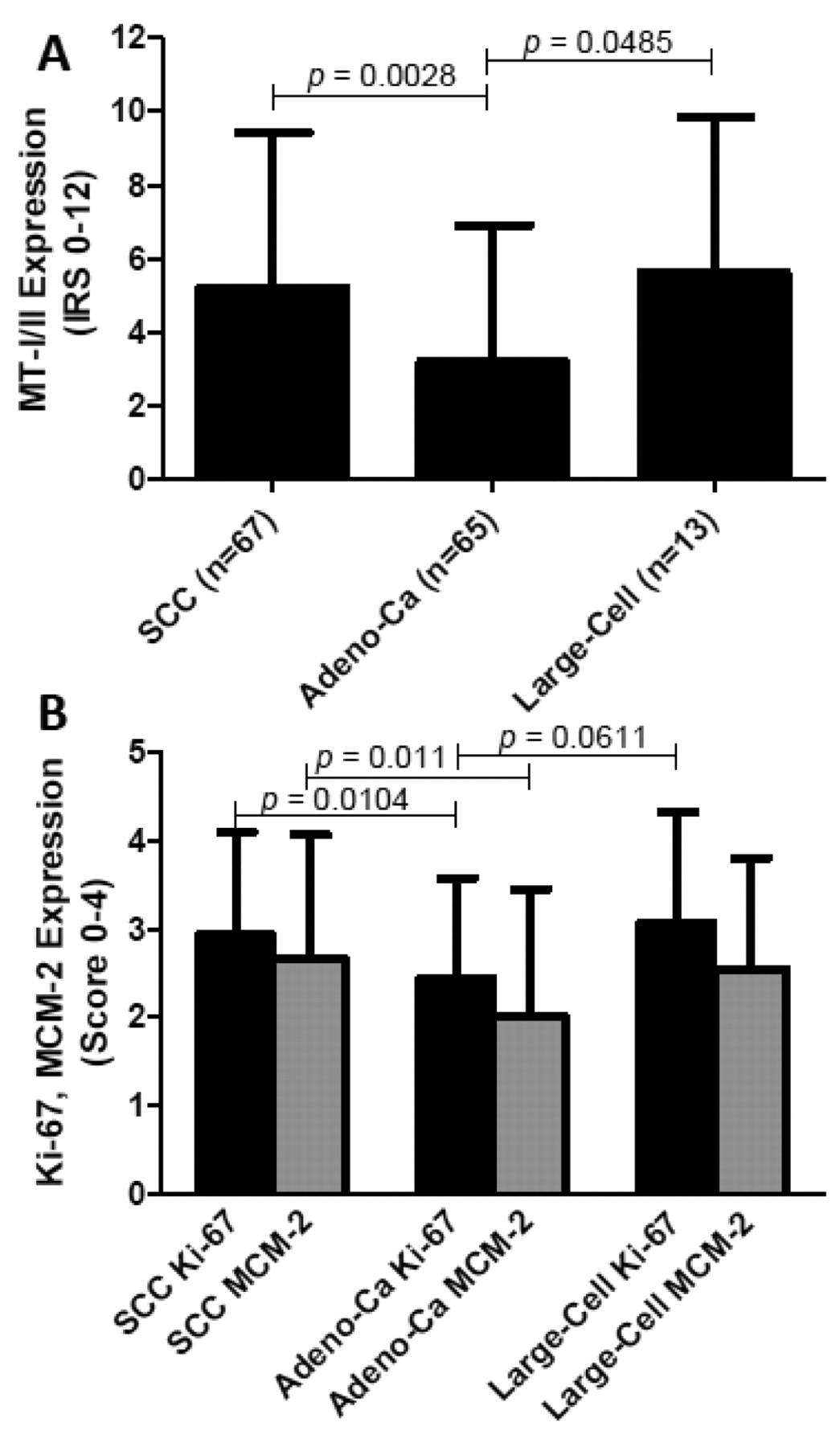
Expression of MT-I/II (A), and Ki-67 and MCM-2 (B) in individual histological types of NSCLC.
The highest expression of MT-I/II was detected in the large cell carcinomas and the least in adenocarcinomas (adenocarcinomas versus SCC, p=0.0028, and versus large cell carcinoma, p=0.0485) (Figure 2A). A similar relationship was detected for the two proliferation markers (Figure 2B). Expression of Ki-67 and MCM-2 was significantly higher in SCC than in adenocarcinoma (p=0.0104 and p=0.011). The difference in intensity of Ki-67 antigen expression between adenocarcinoma and large cell carcinoma approached the threshold of statistical significance (p=0.0611). No significant differences were detected in intensity of MT-I/II expression between individual malignancy grades of SCC and adenocarcinoma, although a trend for increasing expression (statistically insignificant), paralleling increasing malignancy of adenocarcinoma was demonstrated (Figure 3A and B). In SCC, a significantly higher expression of Ki-67 antigen was noted in G2 and G3 cases, as compared to G1 cases (p=0.0131 and p=0.0186). In adenocarcinomas, the only significant difference involved intensity of Ki-67 antigen expression between G1 and G2 cases. No significant differences were observed in expression of MCM-2 between individual grades of malignancy in SCC or adenocarcinoma (Figure 3 C, D).

Expression of MT-I/II (A, B) and Ki-67 and MCM-2 (C, D) in SCC (A, C) and adenocarcinoma (B, D) according to grade of malignancy.
None of the studied markers demonstrated a correlation with the size of the primary tumour or patient age in NSCLC overall or with the individual histological subtypes (Spearman's rank correlation test, data not shown). Moreover, no relationship was demonstrated between expression of the studied markers and the presence of metastases in the lymph nodes or the presence of necrosis in the tumour (Fisher exact test, data not shown). No differences were shown in the intensity of MT-I/II, Ki-67 and MCM-2 expressions and the gender of the patients (Mann-Whitney's test, data not shown).
Kaplan-Meier analysis demonstrated no significant differences in patients' survival according to intensity of MT-I/II, Ki-67 or MCM-2 expression in the NSCLC carcinoma overall to or individual histological types of tumour. As compared to the patients with T1 and T2 tumours, the patients with T3 or T4 tumours manifested significantly shorter survival (p=0.001), similarly to patients with metastases in the lymph nodes (p=0.0001). The univariate analysis is summarized in Table III. Analysis of survival based on the expression of MT-I/II supplemented by one of the proliferation antigens (Ki-67 or MCM-2) showed no statistically significant differences, although the shorter survival of patients with high expression of MT-I/II and Ki-67 in the tumour cells as compared to patients with low expression of MT-I/II and Ki-67 was close to statistical significance (Figure 4 A and B).
Discussion
The present results confirmed the observations of Theocharis et al. (16), that higher expression of MT-I/II was demonstrated in SCC than in adenocarcinoma. In addition, high expression of MT-I/II in large cell carcinoma was documented. The present study also showed significantly higher expressions of both MCM-2 and Ki-67 in SCC than in adenocarcinoma and the highest expressions of MCM-2 and Ki-67 in poorly differentiated tumours of all the subtypes of NSCLC, which confirmed the findings of Yang et al. (26), in relation to MCM-2 in squamocellular and poorly differentiated G3 carcinomas. In the present study, the expression of MT-I/II increased, though not significantly, with the grade of malignancy (peak expression in G3) and correlated with the proliferation markers (Ki-67, MCM-2), which confirmed the earlier observations made in other malignant tumours (29, 30). Interestingly, expression of MT-I/II failed to correlate with Ki-67 antigen expression in SCC, but correlated significantly with its expression in adenocarcinoma, which may point to a more pronounced role of MT-I/II in development of this type of cancer.
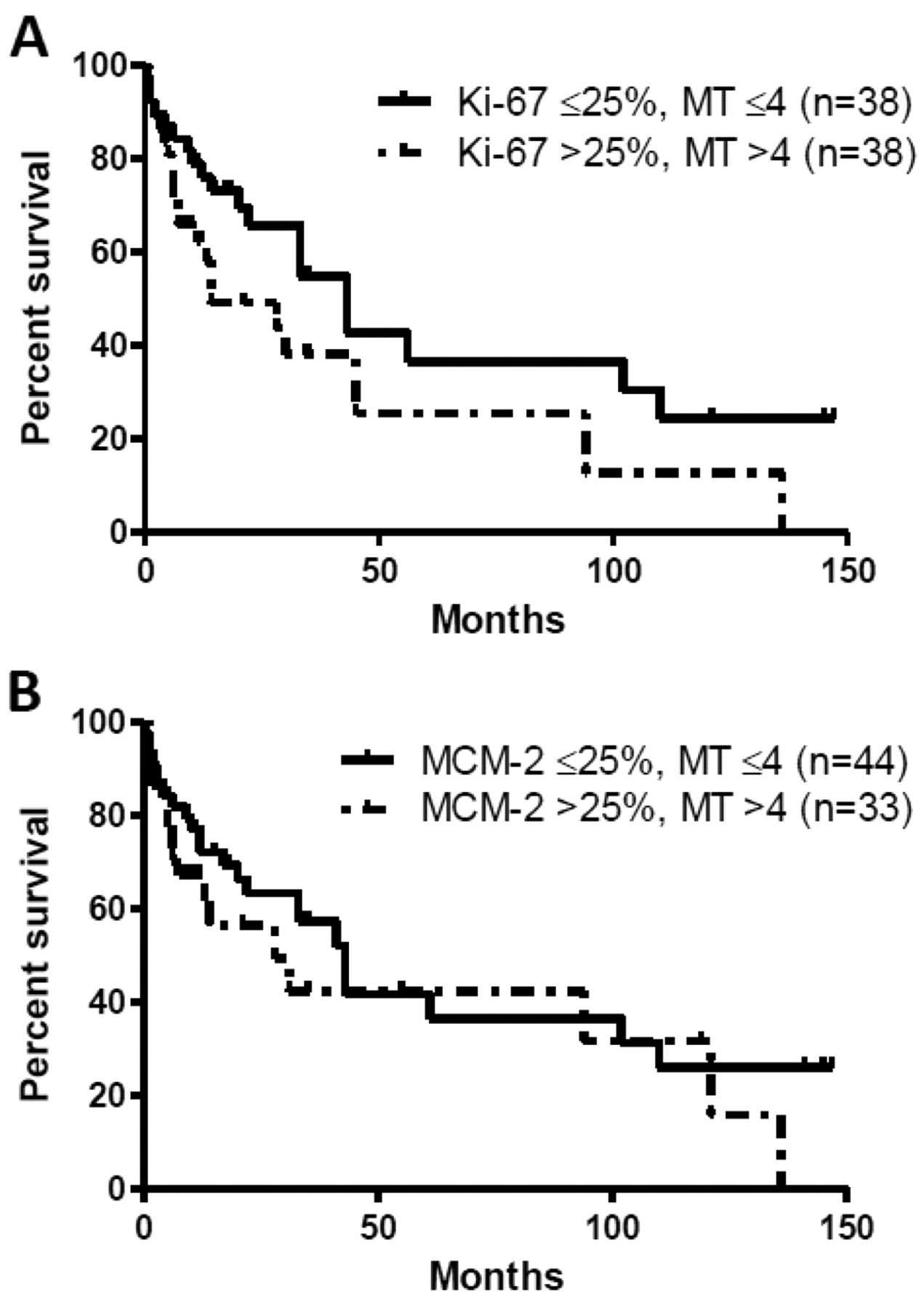
Kaplan-Meier survival curves for pairs of prognostic factors. Combination of MT-I/II and Ki-67 positivity (p=0.0673) (A), and combination of MT-I/II and MCM-2 positivity (p=0.3002) (B).
To date, the commonly used marker of proliferation has been the Ki-67 antigen. In NSCLC, Ramnath et al. (25) found that higher expression of MCM-2 correlated with shorter survival of the patients and represented an independent prognostic factor. The results were also corroborated by observations of Hashimoto et al. (27). The present results, however, indicated a lack of prognostic significance of both Ki-67 and MCM-2, and of MT-I/II, even though earlier studies pointed to their unfavourable prognostic role in various types of tumours (15-19, 25, 27, 29, 30). Our earlier investigations (18) suggesting prognostic value of MT-I/II expression in NSCLC were conducted on a low number of cases, which might explain the difference in study results. This report is the first to document the absence of prognostic significance linked to MCM-2 protein expression. Other recognized prognostic factors, e.g. tumour size and the presence of metastasis to lymph nodes, had the expected negative prognostic significance, which pointed to reliable selection of the studied group. The survival analysis according to parallel Ki-67 and MT-I/II expression yielded an evident prognostic effect when groups with the most and the least pronounced expression of the two proteins were compared. In contrast, no such effect was noted when the common expression of MCM-2 and MT-I/II was used in the analysis, where the difference in patients' survival did not even approach statistical significance.
Kaplan-Meier analysis of prognostic factors in 145 patients with non-small cell lung cancer.
In summary, MT-I/II expression has higher significance in the pathogenesis of pulmonary adenocarcinoma, as compared to other histological types, although the lack of correlation with tumour size, the presence of lymph node metastases and patients' survival indicates that it cannot be regarded as a prognostic marker of NSCLC. Due to the complexity of mechanisms of the neoplastic process, the importance of analysing expression of several (e.g. MT-I/II, Ki-67), simultaneously, is supported by the present results.
Acknowledgements
This research was supported by Wroclaw Research Centre EIT+ under the project ‘Biotechnologies and Advanced Medical Technologies’, BioMed (POIG.01.01.02-02-003/08) financed from the European Regional Development Fund (Operational Programme Innovative Economy, 1.1.2).
- Received April 18, 2011.
- Revision received June 14, 2011.
- Accepted June 15, 2011.
- Copyright© 2011 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Loss of long-range co-expression is a common trait in cancer
- MCM5 Expression Is Associated With the Grade of Malignancy and Ki-67 Antigen in LSCC
- Expression of Metallothionein I/II and Ki-67 Antigen in Graves' Disease
- SATB1 Level Correlates with Ki-67 Expression and Is a Positive Prognostic Factor in Non-small Cell Lung Carcinoma
- Expression of SATB1, MTI/II and Ki-67 in Mycosis Fungoides
- Expression of MCM-3 and MCM-7 in Primary Cutaneous T-cell Lymphomas
- The Lack of Evidence for Correlation of Pyruvate Kinase M2 Expression with Tumor Grade in Non-small Cell Lung Cancer
- In Vitro Analysis of the Relationships Between Metallothionein Expression and Cisplatin Sensitivity of Non-small Cellular Lung Cancer Cells
- TSH induces metallothionein 1 in thyrocytes via Gq/11- and PKC-dependent signaling
- Expression of Metallothionein-III in Patients with Non-small Cell Lung Cancer
- Tissue Microarray Technique in Evaluation of Proliferative Activity in Invasive Ductal Breast Cancer