


Abstract
Background: Knowledge of the characteristics and effective use of tumour markers for mesothelioma is essential for early-stage diagnosis of mesothelioma. We examined whether renal dysfunction influences blood concentrations of promising new tumour markers, N-ERC/mesothelin (N-ERC) and osteopontin (OPN), to an important degree. Patients and Methods: Levels of serum N-ERC and plasma OPN in 32 patients with chronic renal dysfunction, 22 of whom were on hemodialysis (CKD group), and 102 healthy volunteers were measured. Results: Serum concentrations of N-ERC and plasma concentrations of OPN in the CKD group were significantly higher than those in volunteers, regardless of diabetes status and age. Blood concentrations of these markers increased as renal function decreased. Conclusion: N-ERC and OPN concentrations are significantly influenced by renal function. Therefore, the extent of renal failure must be considered when inferring the existence of tumours and chemotherapeutic response from the values of these markers in routine practice.
Individuals at high risk for mesothelioma due to severe exposure to asbestos can be readily identified, and diagnosis of malignant mesothelioma (MM) at an early stage improves its otherwise dismal prognosis (1). However, most patients are diagnosed at a clinically advanced stage because it is difficult to confirm the existence of these tumours with current imaging technology alone. Therefore, there is a strong need to study the characteristics of tumour markers for MM for them to be used more effectively.
We previously studied N-ERC/mesothelin (N-ERC) and osteopontin (OPN) (2-11) as promising tumour markers for MM. In the course of these studies, we found that the blood concentration of N-ERC increases with age and that the serum level of N-ERC is elevated in haemodialysis patients. These findings suggested renal function influences the concentrations of these tumour markers. Furthermore, most patients with MM are elderly and have various degrees of renal dysfunction, and their renal function sometimes becomes worse during chemotherapy. Therefore, it is important to determine the relations between the concentrations of tumour markers and the extent of renal failure to make an accurate early diagnosis and to judge the effect of chemotherapy.
In this study, we have examined whether and to what extent renal dysfunction influences the blood concentrations of N-ERC and OPN, tumour markers of MM.
Patients and Methods
Study samples and assays. This study was conducted as a part of our research program to develop tumour markers for mesothelioma (2, 3). This program was approved by the Institutional Review Board of Juntendo University School of Medicine, its hospital, Shouwakai Hospital, National Organization Tokyo Hospital, Hyogo Prefectural Amagasaki Hospital, Japan Anti-Tuberculosis Association Fukujuji Hospital, Yokosuka Kyosai Hospital, St. Marianna University School of Medicine, Tohoku University Hospital, and Immuno-Biological Laboratories, Ltd. This study primarily uses data from patients in the first two hospitals listed above.
Blood sample was collected once from patients with various levels of renal dysfunction, including those on dialysis, and healthy volunteers when they first visited hospital immediately after their informed consent were given, period from August 2005 until the end of March 2008.
We used the new estimated glomerular filtration rate (eGFR) for Japanese and the chronic kidney disease (CKD) classification, which define renal function more specifically and clearly, as follows: eGFR (ml/min/1.73 m2)=194×Cr −1.094×age−0.287 (female: ×0.739), with the CKD classifications according to eGFR in ml/min/1.73 m2 of stage I ≥90, stage II 60-89, stage III 30-59, stage IV 15-29, and stage V <15.
Characteristics of patients and volunteers.
The serum levels of N-ERC and the plasma levels of OPN were measured by a specialist at the Juntendo University School of Medicine with an N-ERC/mesothelin ELISA Kit (7-16) (Immuno-Biological Laboratories, Ltd., Gunma, Japan) and a Human Osteopontin Assay Kit (Immuno-Biological Laboratories), respectively.
Statistical analysis. ELISA data were analysed with JMP and SAS version 8.1.3 (SAS Institute, Cary, NC) and Graph Pad Prism 4.0 (GraphPad Software, San Diego, CA). To compare serum and plasma levels between groups, the Mann-Whitney test was used. Linear regression analysis was used to analyse the trend of increasing serum and plasma levels with increasing CKD stage. Furthermore, multiple linear regression analysis was used to estimate the important variables that caused the differences in concentrations of these markers between the CKD group and volunteers. A value of p<0.05 was considered statistically significant.
Results
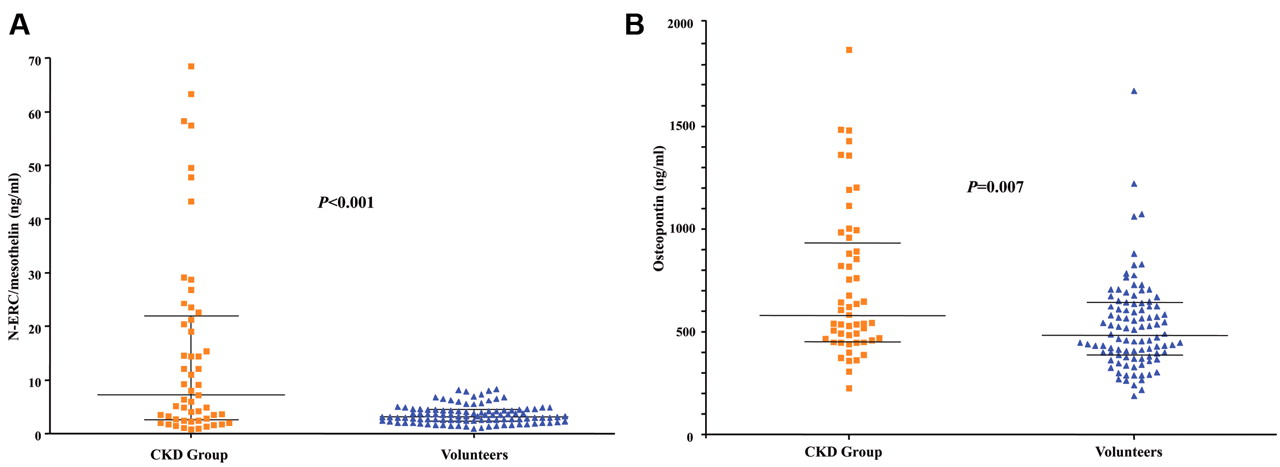
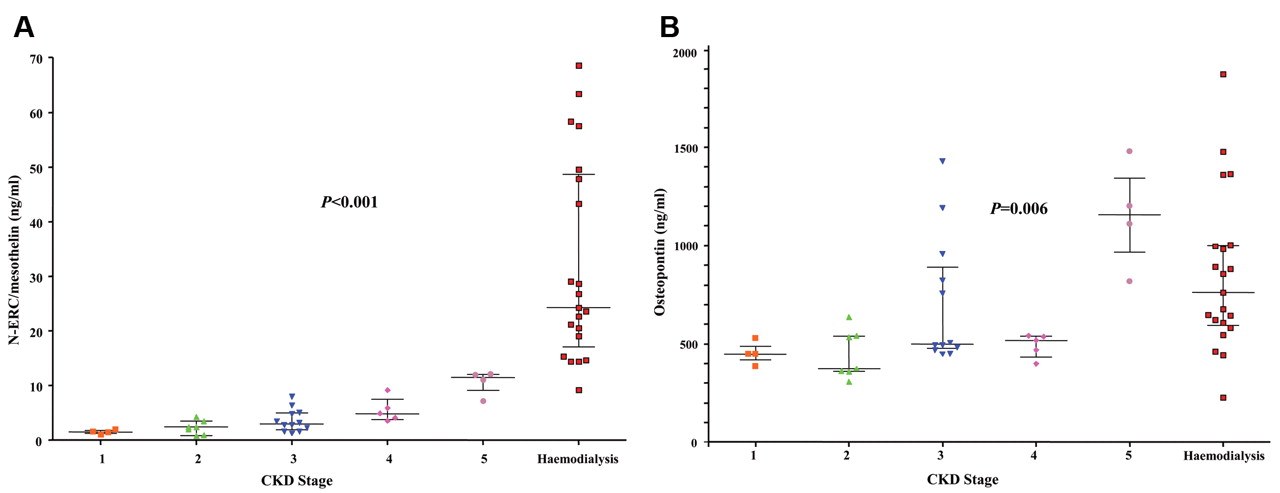
Blood samples were obtained from 32 patients with chronic renal dysfunction, 22 of whom were on haemodialysis (CKD group), and from 102 healthy volunteers. Characteristics of the patients are shown in Table I. Serum concentrations of N-ERC and plasma concentrations of OPN in the CKD group were significantly higher than those in the volunteers (Figure 1). The blood concentrations of both markers increased as renal function decreased (Figure 2). This tendency was especially strong for N-ERC.
To confirm that the upward trend in the concentrations of these markers was caused by renal dysfunction and not by other factors (age, sex, diabetes, and hypertension), we examined these factors with multiple regression analysis. The results of this analysis show that renal function strongly influenced the concentrations of these markers, regardless of any effect of the other covariates (Table II).
Multivariate analysis of risk factors for the elevation of blood concentration of tumour markers in the CKD group.
Discussion
Mesothelioma initially progresses along the surfaces of the pleura and peritoneum without forming masses, which means that it is anatomically difficult to diagnose at an early stage with current imaging technologies. Therefore, the need for tumour markers is greater for mesothelioma than for other tumour types. Furthermore, it is important not only to develop high quality tumour markers but also to use them effectively.
Tumour markers can be influenced by many factors, one of which is renal function. At present, there are a number of published reports that suggest a relation between renal function and the blood concentrations of tumour markers (13-22). However, the published data are still very limited and insufficient to allow the knowledge to be put into effective clinical practice. We think it is important to determine how strong this relation is because such information may lead to the development of new and more sensitive diagnostic strategies.
Our study has shown that the concentrations of N-ERC and OPN are influenced by renal function. First, we simply compared the concentrations of N-ERC and OPN from patients with CKD to those of healthy volunteers. In the case of N-ERC, the results show there is a possibility that renal function strongly influences its concentration (Figure 1A, median: 7.144 versus 3.175 ng/ml for the CKD and control groups, respectively, p<0.0001). In the case of OPN, the P-value was statistically significant (p=0.007), but the difference in median values was smaller (Figure 1B).
We then examined the relation between the degree of renal dysfunction and the concentrations of these markers. The concentration of N-ERC increased as the CKD stage increased (Figure 2), which indicates that there is a strong relation between renal function and the concentration of N-ERC. OPN showed a tendency similar to that of N-ERC, but the tendency was weaker, and the variance was wider.

A: Serum N-ERC/mesothelin levels in the chronic kidney disease group (CKD, comprising renal dysfunction and hemodialysis patients) and healthy volunteers. B: Plasma osteopontin levels of the CKD group and the volunteers. The lines indicate the 25 percentile, median (50 percentile) and 75 percentile.

A: Correlation between chronic kidney disease stage and serum levels of N-ERC/mesothelin. B: Correlation between chronic kidney disease stage and plasma levels of osteopontin.
We finally investigated the strengths of the influence of renal dysfunction, diabetes, hypertension, and age on the concentrations of N-ERC and OPN because of the fact that more than half of the study patients with CKD had diabetes and hypertension and because our previous data showed serum N-ERC to increase with age (2). Our results supported the hypothesis that renal dysfunction influences the concentrations of these markers. A previous report showed a relation between the tumour marker for mesothelioma, megakaryocyte proliferating factor (MPF), and renal dysfunction (23). Because MPF is the same molecule as N-ERC, which is an N-terminal fragment of the mesothelin molecule, this finding also supports our hypothesis.
Of course, the present study is small and requires further validation. Other factors that are thought to influence the concentration of these markers should be assessed. However, the results of our study show that the consideration of renal function is very important in daily practice and suggests that investigating other factors that have the possibility of affecting the concentration of tumour markers is also important for their effective use.
Our next steps will be to study to what extent diagnostic specificity is increased by developing a new marker that has been adjusted to the severity of renal dysfunction and to investigate in detail whether there are other important diseases that influence the concentrations of N-ERC and OPN. We will also determine the generality of these effects by examining other markers that may be affected by renal dysfunction.
Conclusion
The concentration of N-ERC/mesothelin appears to be strongly influenced by the degree of renal dysfunction. The concentration of osteopontin is also influenced by renal dysfunction but to a lesser extent than that of N-ERC. The extent of renal failure must be considered when these markers are used in routine practice.
Acknowledgements
We thank Naoko Aoki and Masaaki Abe for their help in the management of this study.
- Received December 15, 2010.
- Revision received March 10, 2011.
- Accepted March 11, 2011.
- Copyright© 2011 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Mesothelioma Biomarkers: A Review Highlighting Contributions from the Early Detection Research Network
- Proteome Screening of Pleural Effusions Identifies Galectin 1 as a Diagnostic Biomarker and Highlights Several Prognostic Biomarkers for Malignant Mesothelioma
- Challenges and controversies in the diagnosis of mesothelioma: Part 1. Cytology-only diagnosis, biopsies, immunohistochemistry, discrimination between mesothelioma and reactive mesothelial hyperplasia, and biomarkers
- Effectiveness of mesothelin family proteins and osteopontin for malignant mesothelioma