


Abstract
Introduction: Breast cancer (BC) is the most common cancer in women in Western countries, showing a bimodal age distribution with peaks at 50 and 70 years. Multiple factors are encountered in the etiology of BC, including hereditary and hormonal causes. A few viruses, including MMTV, EBV and HPV have been reported to be associated with BC. This group previously described the presence of the measles virus (MV) in biopsies of patients with Hodgkin's lymphoma. The present study explored MV antigens in BC patients. Patients and Methods: A total of 131 patients with invasive BC diagnosed during the years 1998-2005 were studied using immunohistochemistry (IHC) for the presence of MV antigens, hemagglutinin and nucleoprotein. Clinicopathological parameters included age, stage, histological grade and the expression of estrogen and progesterone receptors, HER2/neu, p53, and Ki67. Results: Hormone receptors and HER2/neu were positive in 54% and 18% of the tumors, respectively. Both MV antigens were detected in 64% of the tumors. All biopsies containing a DCIS component showed MV in DCIS in addition to invasive BC. In univariate analysis, MV correlated with estrogen receptor (p=0.018), low Ki67 index (<40%, p=0.029), low or intermediate grade (p=0.037), age under 50 years (p=0.039), progesterone receptor (p=0.043) and overexpression of p53 (p=0.049). In multivariate analysis, only grade (p=0.011), p53 (p=0.03) and age (p=0.041) remained associated with MV. Conclusion: This study provides evidence for the presence of MV antigens in a relatively large proportion of BC patients. MV was associated with younger age, lower histological grade and overexpression of p53, suggesting that it may play a role in the development of BC.
Breast cancer (BC) is the most common cancer among women of the Western world (1). The incidence of BC shows a bimodal age distribution. It increases with age: it starts to climb in the end of the third decade of life, peaks at the age of 50 and then peaks again at 70 years of age (2). The occurrence of this bimodal curve suggests that diverse factors may be encountered in the etiology of BC at different ages (3). The two breast/ovary hereditary cancer genes BRCA1/2 are characterized by high penetrance and are responsible for the occurrence of breast and ovarian tumors in patients with a strong family history. Prolonged exposure to estrogen in conditions such as early menarche, late menopause or nulliparity increases the risk for developing BC-expressing hormone receptors (4). Nevertheless, no clear etiology can be identified in the vast majority of BC patients.
Viruses have long been suspected for the etiology of BC. Three viruses, the Epstein-Barr virus (EBV), the mouse mammary tumor virus (MMTV) and the human papilloma virus (HPV) have been studied extensively for their association with BC (5, 6). EBV, DNA-fragments and viral antigens are rarely detected in biopsies of Western BC patients (7), and this virus is not considered to play an important role in the etiology of most BC tumors. The identification of MMTV may support a viral etiology for breast tumors in animals, but similar viral sequences found in humans are not believed to play any direct role in the development of BC (8, 9). Although high-risk HPVs are a well-established cause of cervical cancer, attempts to detect similar HPV-DNA sequences in BC using DNA amplification by PCR have yielded inconsistent results, arguing against its role in the pathogenesis of BC (10, 11). Despite a paucity of supportive evidence, viruses remain an attractive model for the etiology of BC, particularly in the younger age-group.
This group previously reported that the measles virus (MV) may be detected in tumors of Hodgkin's lymphoma, particularly in young female patients (12). It was later suggested that the sharp rise in the incidence of Hodgkin's lymphoma in Israel-born adults, most prominently in young adult females, may be related to countrywide outbreaks of measles (13). Since a similar rise in incidence has been observed in young BC patients (14), it was speculated that MV also may be associated with the occurrence of BC in this age group. This report describes the findings of MV antigens in breast tumors using similar immunohistochemistry (IHC) techniques.
Antibodies, suppliers, dilutions and techniques used for immunohistochemical evaluation of percentage and intensity of staining.
Patients and Methods
Study population. The study population consisted of newly-diagnosed BC patients with early or locally advanced, invasive ductal tumors, diagnosed at the Soroka Medical Center during the years 1998-2005. Male patients or patients with a histological diagnosis of BC other than invasive ductal carcinoma, bilateral breast tumors, or a previous history of another primary tumor were excluded from the study. Only patients with adequate pathological specimens and available clinical data were included in the study. Patients were selected according to the following parameters: age, lymph node, and hormone receptor status. Data encompassed demographic and clinical parameters and pathological stage according to the AJCC classification for BC, 2002 version (15). The study was conducted after the approval of the appropriate Ethical Review Boards.
Pathology. Hematoxylin and eosin-stained slides were reviewed for confirmation of histopathological diagnosis and for selection of specimens for analysis. The histological identification of BC was determined as recommended by the World Health Organization (16). Grade was determined according to the Allred score applying the modified Scarff-Bloom-Richardson grading system (17) by two pathologists (DB and NSV) who were blinded to the clinical data. In each case, a representative paraffin block of the tumor was chosen and sections were selected for IHC studies. In addition to invasive carcinoma, all specimens were reviewed for the presence of a DCIS component. In patients who received neoadjuvant chemotherapy, pathological data also included state of response (pCR) after completing chemotherapy.
IHC. Standard IHC studies were performed for estrogen, progesterone and HER2/neu receptors, Ki67 proliferation index and p53 according to the manufacturer's instructions (Table I). IHC studies for MV were performed using the avidin-biotin peroxidase complex (Envision; DAKO, Glostrup, Denmark). IHC studies were performed as follows: 4 μm tissue sections of paraffin-embedded tissue were mounted on glass slides coated with silane (Sigma Chemical Co., Saint Quentin, France). Sections were dried at 37°C for 48 h before deparaffinization. Deparaffinization was performed for 20 min and rehydrated with alcohol 100%, 90%, and 70%, 3 min each. After deparaffinization, the slides were washed in distilled water and incubated in 3% hydrogen peroxide in methanol for 15 min to block the endogenous peroxidase activity. After incubation the slides were incubated in 10 mmol/l citrate buffer (pH 6) and heated in a microwave oven at 800 W for cycles of 15 min for antigen retrieval. After heating the slides were allowed to cool at room temperature for 30 min and washed in phosphate-buffered saline (PBS) before staining. The primary antibody was applied to the slides and incubated at room temperature for 1 h. After three washes in PBS, the slides were treated with Envision anti-goat IgG biotin-labeled secondary antibodies (Envision; DAKO) at a dilution of 1:500 (diluted in 0.05% PBS-Tween 20) at room temperature for 1 h. Bound antibodies were washed three times in PBS. Finally, the slides were reacted with the 3,3 diaminobenzidine chromagen (Sigma Chemical Co.), washed, counterstained with hematoxylin, dehydrated, treated with xylene and mounted.
Assignment of MV status according to staining intensity for anti-nucleoprotein (NP 39/22) and anti-hemagglutinin (HL 77).
Antibodies. Two anti-measles monoclonal antibodies, anti-nucleoprotein (L39/61) and anti-hemagglutinin (L77), were used for staining. Both were provided by Birrer et al. (18). The specificity of these antibodies was established by Western blotting. A neuroblastoma cell line that was permanently infected by MV was used as a positive control and the same cell line without infection with MV was used as a negative control. L39/61 antibody was diluted in 1:100, and L77 antibody was diluted in 1:70.
Antibodies for the following antigens were used for other IHC studies: estrogen receptor (ER), progesterone receptor (PgR), HER2/neu, p53, and Ki67. A full list of the antibodies used and the evaluation criteria for each is presented in Table I. Expression for cases with a HER2 HercepTest score of 3 were scored as positive, and those of 0 or 1 were scored as negative as described in the HercepTest (Dako) protocol (19). Cases with HER2/neu score of 2 were re-evaluated by fluorescence in situ hybridization (FISH) assays.
Evaluation of MV antigens. The cytoplasmic intensity of MV hemagglutinin and MV nucleoprotein were evaluated separately and scored semi-quantitatively as negative (0; no expression or weakly-positive staining in ≤ 30% of cells or strongly-positive staining in <20% of cells), weakly positive (+1; strongly-positive staining in >20% of cells or weakly-positive staining in >50% of cells) and strongly-positive (+2; strongly-positive staining in >50% of cells). Patients with tumors showing a weak (+1) or strong (+2) immunoreactivity were assigned to the MV-positive group. In order to increase the stringency of the MV assay, a case was considered positive for MV if both anti-nucleoprotein and anti-hemagglutinin staining were positive. Table II shows the criteria for MV status assignment (positive versus negative).
Statistical analysis. Descriptive statistics were calculated as frequencies to summarize clinicopathological characteristics. The following parameters were retained or converted into dichotomic variables and studied for correlation with MV status: age, ethnicity and place of birth, tumor stage (T), lymph node stage (N), histological grade, presence of a DCIS component, pathological complete response (pCR) after neoadjuvant chemotherapy, ER, PgR, HER2/neu, p53, and Ki67. The χ2 and Mann-Whitney U-tests were used as appropriate. Results of the univariate analysis were further used to identify predictors for MV status in the subsequent multivariate analysis. All statistical tests were two-sided and statistical significance was defined at a level less than 0.05. The STATA® software (STATA for Windows, version release 9.0; StataCorp LP, College Station, TX, USA) was used for all statistical analyses. Table III shows all the variables used for the analysis.
Assignment of demographic, clinicopathological, and IHC variables in BC patients.
Results
Table IV summarizes the frequencies of baseline characteristics of all BC patients sorted according to ER status. A total of 131 patients with a diagnosis of limited or locally-advanced BC were included in the study. Out of these, 112 patients were diagnosed with limited disease and underwent primary surgical procedure, while 19 patients were diagnosed with locally advanced disease and received neoadjuvant chemotherapy before surgical intervention. The latter group of patients was excluded from correlation analyses for tumor size or lymph node involvement but was evaluated for response to chemotherapy. The average age was 49 years (range, 27 to 79 years), with 81 patients being younger than 50 years and 50 patients being above 50 years of age. Nine of the 131 patients (7%) were Bedouin Arabs. Hormone receptors were detected in 72 patients (55%). The tumor size was more than 10 mm in 48 out of 114 patients (42%). A DCIS component was found in 53 of 131 patients (40%). Sixty-two out of 112 patients (47%) showed regional lymph node involvement. Nineteen patients received neoadjuvant chemotherapy with one of them showing pCR. Low or intermediate pathological grade (G1-2) was found in 50 out of 71 patients (70%) with ER-positive tumors and in 11 out of 60 patients (18%) with ER-negative tumors. In 60 out of 131 patients (46%), PgR was positive. Positive Ki67 staining was found in 22 out of 60 patients (37%) with ER-negative tumors, compared with 2 out of 71 patients (3%) with ER-positive tumors. Overexpression of p53 was found in 28 out of 60 patients (47%) with ER-negative tumors, compared with 14 out of 70 patients (20%) with ER-positive tumors. Positive HER2/neu status was found in 23 patients (18%). Positive staining for MV hemagglutinin and MV nucleoprotein was found in 100 (76%) and 107 (82%) out of 131 patients, respectively, while positive staining for both antigens was observed in 84 patients (64%). Staining for both MV antigens was cytoplasmatic and all biopsies containing DCIS component (40% of cases) showed MV in DCIS in addition to the presence of MV antigens in the invasive component. Figure 1 shows degrees of positive IHC staining (+1, weakly positive; +2, strongly positive) for MV hemagglutinin and MV nucleoprotein in BC biopsies.
Demographic, clinicopathological and IHC characteristics of BC patients according to ER status.
Factors associated with MV positive status in BC patients.
In the univariate analysis, positive MV status (positive expression of both MV antigens, Table V) was associated with ER-positive expression (p=0.018), negative Ki67 status (p=0.029), low to intermediate pathological grade (G1-2) (p=0.037), younger age (p=0.039), PgR-positive expression (p=0.043) and overexpression of p53 (p=0.049). Positive MV status was not associated with place of birth, ethnic origin, tumor size, regional lymph node involvement, DCIS component in the biopsy or HER2/neu overexpression. Stepwise multivariate regression analysis resulted in the determination of the optimal set of variables to be included in the equation, as follows: (i) age ≤50 years (yes=1, no=0), (ii) low or intermediate histological grade (yes=1, no=0), (iii) Ki67 index <40% (yes=1, no=0), (iv) positive ER status (yes=1, no=0), (v) positive PgR status (yes=1, no=0), (vi) positive p53 status (yes=1, no=0) and (vii) lymph node involvement (yes=1, no=0). The logistic regression model provided the estimated probability of positive MV status for a particular patient with BC. In the multivariate logistic regression analysis (Table VI), the only independent variables associated with positive MV status were low and intermediate grade (p=0.012), positive p53 staining (p=0.033) and age ≤50 years (p=0.041).
Multivariate logistic regression analysis, showing factors associated with MV-positive status in BC patients.
Discussion
This study reported the presence of MV antigens in a relatively large proportion of patients with BC. The occurrence of MV antigens was associated with certain biological parameters, including lower histological grade, p53-positive status, and age less than 50 years. It was not associated with either hormone receptor status or involvement of regional lymph nodes. Since most patients belonging to the younger age group were premenopausal, the association of MV antigens with this age group probably indicates a premenopausal state. Although the clinical course of BC in younger patients is more aggressive than in older patients, molecular studies have shown that there are few age-specific differences in breast tumor biology and age alone does not appear to provide an additional layer of biological complexity above that of BC subtype and grade (20). Molecular studies have shown a specific genetic profile in breast tumors expressing hormone receptors (21). However, the presence of MV antigens in the present study was not associated with hormone receptor status. This finding may imply that MV infection probably occurred at an early point of BC development, before cells are committed to the expression of hormone receptors. In addition, MV was detected in all DCIS components of MV-positive, but not MV-negative tumors, suggesting that MV infection precedes transformation of DCIS to invasive cancer. Regional lymph node involvement is a major clinical predictor of BC aggressiveness and metastatic potential (22). Despite the fact that the occurrence of MV antigens was not associated with regional lymph node involvement, the relatively short follow-up time and the limited number of relapsing patients in the present study preclude any conclusion with regard to the effect of MV on prognosis.
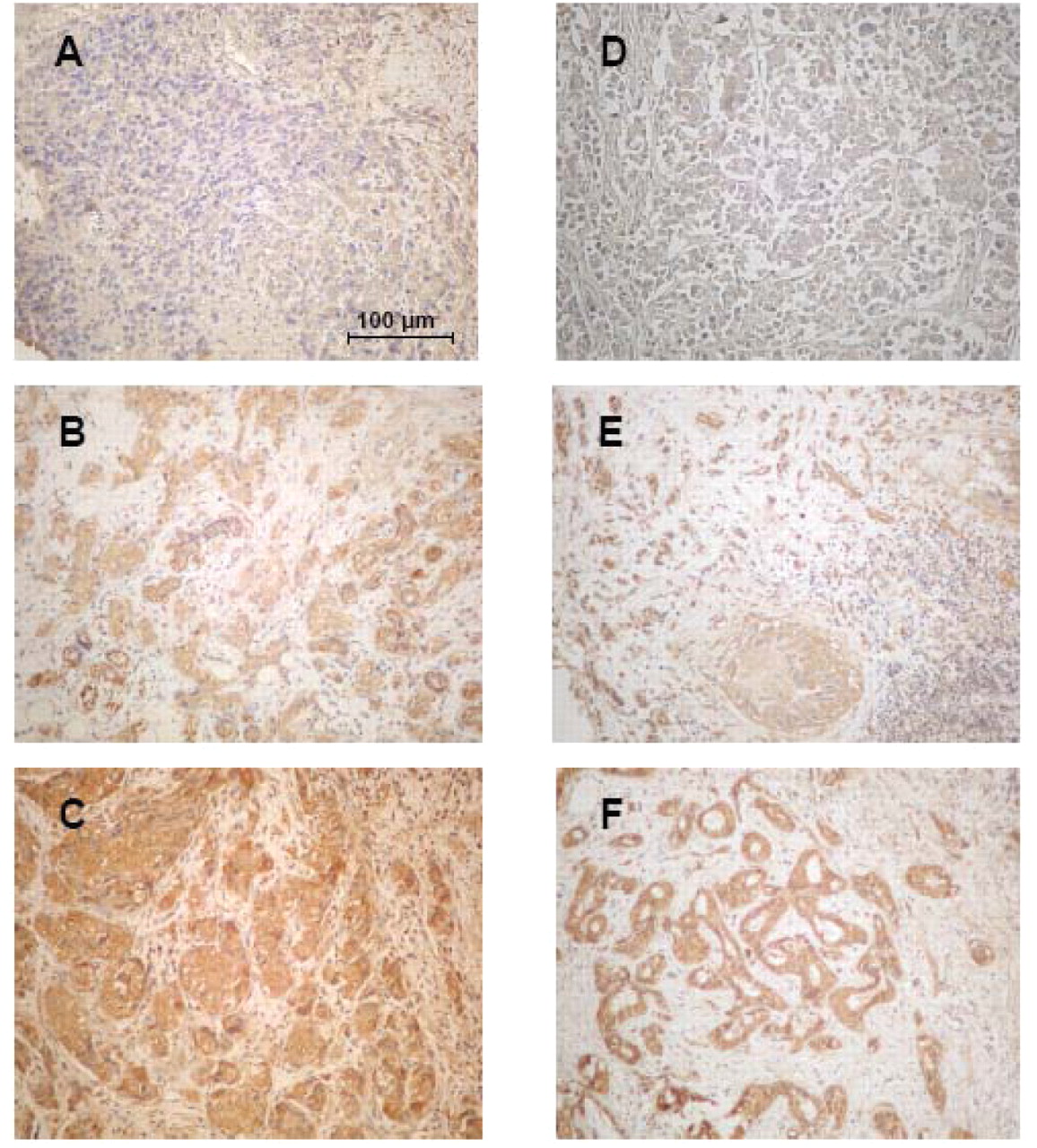
IHC for MV antigens in BC biopsies (with diaminobenzidine, ×240). (A-C) L77 anti-hemagglutinin antibody: (A) negative, (B) mildly positive (+1) and (C) strongly positive (+2). (D-F) NP 39/22 anti-nucleoprotein antibody: (D) negative, (E) mildly positive (+1) and (F) strongly positive (+2).
MV is a ubiquitous RNA virus with highly contagious properties in unvaccinated populations and lifetime immunity after infection. Nevertheless, vaccinated individuals to measles may mount anti-MV antibody titers in a significant proportion, indicating subclinical measles (23). In addition, MV persistence is probably not a rare phenomenon in asymptomatic populations. MV RNA was detected in 8-20% of organs studied from autopsies (24), and MV wild-type genome was detected in peripheral blood lymphocytes of 46% of children who were vaccinated two months earlier or longer (25). All cases showed the same circulating strain in the community.
Since MV is not considered to be an oncogenic virus, the key question is certainly whether the presence of MV antigens in BC may be associated with the development or the biology of BC. This study showed that the presence of MV antigens in breast tumors is associated with overexpression of p53, a crucial regulator of cell proliferation. MV phosphoprotein modulates PIRH2, an ubiquitin-ligase for p53, by preventing PIRH2 ubiquitination and redistributing it outside the nucleus, within intracellular aggregates (26, 27). p53 is a common target for several oncogenic viruses, including HPV and CMV. The HPV-E6 protein binds and degrades the p53 protein through the ubiquitin pathway (28), while the HCMV IE1-72 and IE2-86 bind p53 and suppress its transactivating function (29), which is important for the induction of apoptosis.
MV antigens, hemagglutinin and nucleoprotein, were detected in this study on IHC. A major concern of this study has been the determination of cut-off values, since the clinical relevance of minimal staining with the anti-MV antibodies has yet not been standardized. Although non-commercial monoclonal antibodies were used, their specificity against MV had previously been validated on Western blot and in cell lines persistently infected with MV (30). In the present study, immunostaining for MV antigens was evaluated by a semi-quantitative method, while strict criteria were employed for positive identification of MV, which included positive staining of both antigens. Another limitation of the present study is the lack of molecular validation for the presence of MV in breast tumors. It was previously shown by this group that MV IHC findings correlate with FISH and reverse transcription-polymerase chain reaction results in patients with Hodgkin's lymphoma (12).
In conclusion, this study provided evidence for the presence of MV antigens in a relatively large proportion of BC patients in Israel. MV was linked to younger patient age, lower histological grade and overexpression of p53. It is, therefore, suggested that MV may be involved in one of a series of steps required for tumor development in some BC patients.
- Received January 21, 2011.
- Revision received February 25, 2011.
- Accepted February 25, 2011.
- Copyright© 2011 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.