


Abstract
Aim: To evaluate the influence of viral hepatitis status on the long-term outcome of patients with hepatocellular carcinoma (HCC) in non-cirrhotic livers. Patients and Methods: Two hundred and seventy-nine patients diagnosed with HCC underwent liver resection. Histologic examination of the resected liver confirmed the absence of cirrhosis in 145 patients. Clinical characteristics and surgical outcome were compared between patients with HCC derived from non-cirrhotic liver with (n=111) and without (n=34) viral hepatitis. Results: One-, three- and five-year disease-specific survival rates in patients without viral markers (97.0%, 93.9% and 88.1%, respectively) were significantly higher than in patients with positive viral markers (97.2%, 81.0% and 62.3%, respectively) (p=0.0151). The five-year remnant liver recurrence-free survival rate in patients with negative viral markers (64.1%) was significantly higher than in patients with viral markers (44.9%) (p=0.0412). Conclusion: Hepatic resection is beneficial for HCC in non-cirrhotic livers patients without viral hepatitis.
Hepatocellular carcinoma (HCC) is the fifth most common malignancy worldwide and is the third largest cause of cancer-related deaths (1-2). HCC commonly arises within a background of chronic liver disease, including viral hepatitis B or C, and cirrhosis (1). Although it often develops in cirrhotic livers, it occurs in non-cirrhotic livers in 10-15% of patients (3-5).
Recent studies reported that histopathologic tumor parameters, such as vascular invasion, presence of daughter nodules and tumor multiplicity, surgical radicality and postoperative adjuvant therapy, were prognostic factors of long-term outcomes of patients who underwent liver resection for HCC derived from non-cirrhotic livers (6-7). Of those patients from eastern countries who underwent hepatic resection for HCC arising from non-cirrhotic livers, 20-50% were negative for hepatitis B or C viral markers (8-9). However, few studies have focused on the influence of the viral hepatitis status on long-term outcomes for HCC in non-cirrhotic livers.
The aim of this study was therefore to evaluate this influence by comparing clinical features and surgical outcome between patients with HCC derived from non-cirrhotic livers with and without viral hepatitis.
Patients and Methods
From 1992 to 2007, a total of 279 patients diagnosed with HCC underwent liver resection with curative intent at the Yokohama City University Medical Center, Gastroenterological Center and Yokohama City University Graduate School of Medicine, Japan. Histologic examination of surgical specimens confirmed the absence of cirrhosis in 167 patients (59.9%). Of these, it was not possible to perform a curative hepatectomy in 21 patients, and one patient was lost to follow-up. Accordingly, data from the remaining 145 patients who underwent R0 resection for HCC were analyzed.
These patients were divided into two groups based on their serum viral hepatitis status: the B/C viral group, testing positive for hepatitis B virus surface antigens (HBsAg) or hepatitis C virus antibodies (HCVAb) (n=111); and the non-BC group, testing negative for both HBsAg and HCVAb (n=34). No patients in the latter were previously treated with any anti-viral agents, such as lamivudine, ribavirin, or interferon. Preoperative imaging for tumor staging included chest X-rays, abdominal ultrasonography (US), computed tomography (CT), and magnetic resonance imaging.
Hepatectomy procedures. Hepatic resection was conducted as the primary treatment for HCC when tumors were considered resectable, and was performed according to the anatomical principles of resection. The criteria employed to determine safe hepatic resection were based on a multiple regression equation using the factors of patient age, resection rate and indocyanine green retention at 15 min (ICG-R15), as described previously (10). When an anatomic resection was precluded, non-anatomic resections, local ablation therapy adjunctive to minor hepatic resections, or hepatic resection after portal vein embolization were performed. Major hepatectomy was defined as a surgery consisting of four or more Couinaud's segmentectomies. Operative procedures have been described previously (11-12). The Brisbane 2000 Terminology of the International Hepato-Pancreato-Biliary Association was used to describe liver anatomy and resections (13). Each resected specimen was examined grossly and microscopically as described elsewhere (14-15).
Adjuvant therapy and patient follow-up. After liver resection, adjuvant chemotherapy was administered to patients with pathologically confirmed satellite nodules, vascular invasion or hepatic duct invasion (14). From 2004, nine patients were administered lamivudine (n=3) or entecavir (n=2) for chronic hepatitis B, and interferon-alpha (IFNα) for chronic hepatitis C (n=4). A sustained virological response (SVR) was induced in four patients with hepatitis B and two patients with hepatitis C. Patients underwent a monthly follow-up evaluation at our outpatient clinic. The serum levels of α-fetoprotein and des-γ-carboxy prothrombin were measured monthly, CT or US was performed every 3-4 months, and a chest roentgenogram was obtained every six months.
Statistical analysis. Continuous variables were expressed as the mean±standard deviation and were compared using the Mann-Whitney U-test. Categorical variables were compared using the chi-squared test. Survival rate was calculated by the Kaplan-Meier method, and statistical analysis of differences in survival curves was carried out by log-rank test. All statistical analyses were performed using the SPSS computer software package version 10.0 for Windows (SPSS, Inc., Chicago, IL USA). Probability (p) values <0.05 were considered to be statistically significant.
Results
Population study. During the 15-year study period, the median follow-up time was 25.3 months (range 1-159 months). In the non BC group (34 patients), the underlying liver status was alcoholic liver injury in 4 patients, autoimmune hepatitis in 1 patient, cryptogenic hepatitis in 17 patients and histologically normal livers in the remaining 12 patients. No patient was positive for anti-HB core antibodies (HBcAb).
Clinical findings. The clinicopathological findings are summarized in Table I. The mean age of the non-BC group was 65.1±7.6 years and that of the B/C viral group 63.6 ±9.3 years. Gender ratio was comparable in the two groups. Incidence of diabetes mellitus in the non-BC group was significantly higher than that in the B/C viral groups (47.1% versus 20.7%; p=0.0024). The number of patients with histologically normal livers in the non-BC group was also significantly higher than in the B/C viral group (35.3% versus 9.9%; p=0.0004). No significant differences were found in body mass index (BMI) and prognostic nutritional index [(PNI)=albumin ×10+ lymphocytes ×0.005] between the two groups.
Clinical features of patients without cirrhosis.
Intraoperative data. The non-BC group was more likely to undergo major (four or more segments) resection compared to the B/C group (50.0% versus 23.4%; p=0.0030) (Table II). The resected liver volume in the non-BC group (780.1±915.2 g) was significantly heavier than in the B/C group (463.1±558.3 g) (p=0.0152). The proportion of patients who underwent anatomical resection was similar between the two groups. No significant differences were found in operative time, blood loss, the incidence of red blood cell transfusion, postoperative hospital stay, or the incidence of postoperative complication. The mortality rates within 30 days after the operation in the non-BC group and the B/C group were 0% and 0.9%, respectively.
Pathology. Among the histopathological variables, there was a significant difference in the number of patients with well-differentiated hepatocellular carcinoma (the non-BC group versus the B/C-group: 38.2% versus 20.7%) (p=0.0386). There was no significant difference in the number of patients whose tumor had not invaded the hepatic vein, nor in that for those with peritumor satellite nodules. The B/C group was marginally more likely to have portal vein invasion compared to the non-BC group (p=0.097) (Table III).
Recurrence and survival. Of those patients undergoing an R0 resection of non-cirrhotic livers, 83 (57.2%) developed recurrence during the follow-up period; 59 patients had an HCC recurrence in the liver (9 in the non-BC group, 50 in the B/C viral group), 8 had recurrences both in the liver and extrahepatic sites (2 in the non-BC group, 6 in the B/C viral group), and 16 developed their first recurrence in an extrahepatic site (3 in the non-BC group, 13 in the B/C viral group). Eleven patients in the B/C viral group underwent repeat hepatic resection. No patient in the non-BC group had repeat resection for liver recurrence, as the three who were able to do so instead received local ablative therapy for single hepatic recurrence.

Disease-specific survival after hepatic resection for hepatocellular carcinoma in non-cirrhotic livers. Statistical analysis shows a significantly improved survival after resection in the non-BC group compared with the B/C viral group (p=0.0151, log-rank test).
Type of resection, intraoperative and postoperative outcomes for patients without cirrhosis.
Macroscopic and microscopic characteristics of tumors in non-cirrhotic patients.

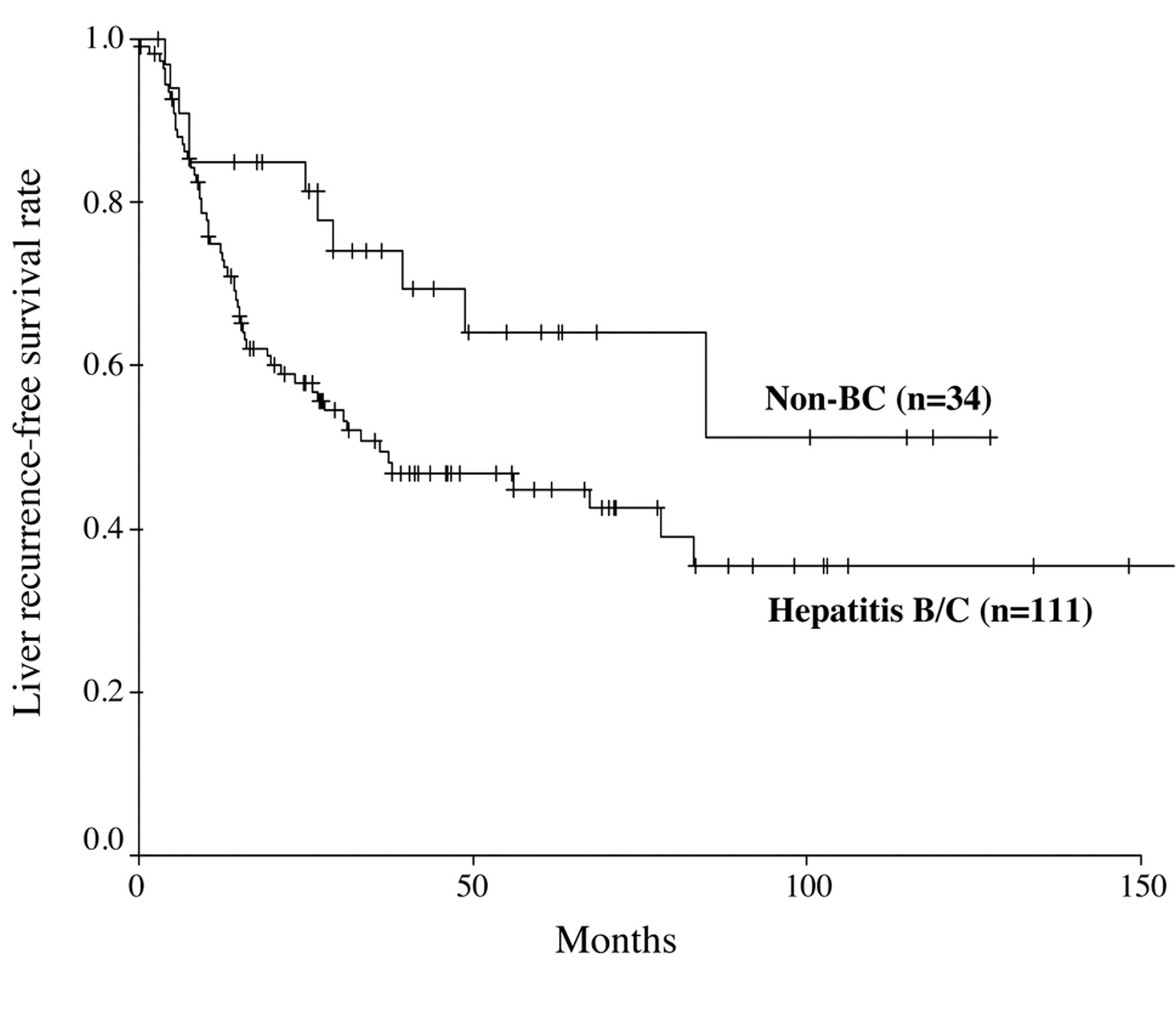
Liver recurrence-free survival after hepatic resection for hepatocellular carcinoma in non-cirrhotic livers. Statistical analysis shows a significantly improved liver recurrence-free survival after resection in the non-BC group compared with the B/C viral group (p=0.0412, log-rank test).
The disease-specific survival rates in the non-BC group (one-, three- and five-year: 97.0%, 93.9% and 88.1%, respectively) were significantly higher than those of the B/C-viral group (one-, three- and five-year: 97.2%, 81.0% and 62.3%, respectively) (p=0.0151) (Figure 1). The five-year remnant liver recurrence-free survival rate in the non-BC group (64.1%) was significantly higher than that of the B/C viral group (44.9%) (p=0.0412) (Figure 2).
Discussion
In this study, we compared clinical characteristics and surgical outcomes between patients with HCC derived from non-cirrhotic livers with and without viral hepatitis in order to evaluate the influence of viral hepatitis status with HCC in non-cirrhotic livers.
Generally, because of the absence of chronic hepatic disease in non-cirrhotic patients, HCC is usually diagnosed when it has reached a size that triggers symptoms (7). Fortunately, large resection is possible on these non-cirrhotic livers. In our study, the mean tumor diameter was 72.4±51.4 mm (range 8-220 mm), and more than three segments were resected in the majority of patients in the non-BC group. Despite the large resections encountered, there was no postoperative mortality and a similar rate of postoperative complications was observed in the two groups (Table II).
The natural course of HCC arising in normal liver parenchyma cannot be assumed to be similar to that in patients with HCC in cirrhotic livers (16-17) because the complications of liver cirrhosis and portal hypertension contribute to the disease process in such patients. Previous studies found that heavy alcohol intake was the only obvious risk factor in some HCC patients without cirrhosis (18). However, in the present study, only four patients had alcoholic liver injury. Type 2 diabetes has been shown to be a risk factor for both chronic liver disease and HCC (19), while obesity is a known risk factor for HCC (20). In our studies, the number of patients with a history of diabetes mellitus in the non-BC group (47.1%) was significantly higher than in the B/C viral group (20.7%) (Table I). In the non-BC group, there was no significant difference in disease-specific survival rate or remnant liver recurrence-free survival rate between patients with a history of diabetes mellitus and those without (data not shown). The number of patients in each subgroup was small, so further studies of a larger number of patients will be necessary to confirm this.
With regard to histologic characteristics of the primary tumor, our results showed a predominance of well-differentiated tumors in the non-BC group (Table III). Compared with conventional HCC associated with viral hepatitis infection, HCC in non-BC partients was found to have a more malignant potential, with poor differentiation of tumor cells, invasive vascular involvement, and intrahepatic metastases (21-22). In our study, we failed to find any of these features in non-BC patients. One of the reasons for this discrepancy might be that the malignant potential of HCC in non-BC patients was simply attributed to the more advanced stage of the disease at diagnosis, rather than to the invasive nature of the cancer. Non-BC patients generally do not have active liver disease and consequently may not have image-based liver screening until symptoms appear.
Data concerning the survival rate after hepatic resection for HCC in non-cirrhotic liver without underlying viral hepatitis are rarely reported. Lang et al. found that the three-year overall survival rate was 38% (23), while Lubrano et al. observed a five-year overall survival rate and disease-free survival rate of 64% and 58%, respectively (24). Our results are concordant with those of Lubrano et al., with a 67.9% five-year overall survival rate and a 55.7% disease-free survival rate. In our studies, both the disease-specific and liver recurrence-free survival rates in the non-BC group were better than in the B/C group (Figures 1 and 2).
Recurrence remains the main problem after liver resection. With respect to postoperative intrahepatic recurrences in HCC, these are common from primary advanced stage tumors with vascular invasion (25, 26), whereas multicentric carcinogenesis in the remnant liver commonly occurs in HCC associated with a viral hepatitis infection (22, 25–28). Based on these observations, a more favorable surgical outcome for HCC in patients with non cirrhotic livers without viral hepatitis might be expected if sufficient hepatectomies that eliminate microscopic lesions surrounding the main tumor are performed at the first diagnosis of HCC.
Attempts to improve long-term patient outcomes with adjuvant therapy, such as oral acyclic retinoid acid (29), adoptive immunotherapy (30), intra-arterial radioiodine therapy (31), and interferon therapy (32-33), after potentially curative HCC treatment have had limited success. In our study, nine patients received postoperative antiviral therapy and SVR was induced in four patients with hepatitis B and two patients with hepatitis C. In the future, further studies of large numbers of patients will be necessary to confirm the benefits of adjuvant therapy for HCC in patients with non-cirrhotic livers with or without underlying viral hepatitis.
In conclusion, non-BC patients with non-cirrhotic livers were more likely to have large and well-differentiated tumors and had a higher rate of diabetes mellitus. Hepatic resection can be beneficial for patients without viral hepatitis for HCC in non-cirrhotic livers because hepatectomies can increase survival and remnant liver recurrence-free survival with no mortality and comparable morbidity.
- Received December 19, 2010.
- Revision received February 3, 2011.
- Accepted February 4, 2011.
- Copyright© 2011 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}