


Abstract
Background: A number of association studies have focused on the effect of polymorphisms related to DNA repair or the xenobiotic pathway, on the susceptibility to gastric cancer (GC). Here, the possible association between common polymorphisms in the X-ray repair cross-complementing groups (XRCC) 1, and glutathione-S-transferase (GST) genes and various clinicopathological characteristics, including overall survival, in GC patients were evaluated. Patients and Methods: XRCC1 Arg399Gln, and Arg194Trp, GSTP1 Ile104Val, and GSTT1, GSTM1 null polymorphisms were determined in 130 GC patients. Results: XRCC1 codon 194 Trp carriers (Trp/Trp + Arg/Trp) held a significantly higher risk of venous invasion (OR=3.76, 95%CI=1.05-13.51, p=0.043). A similar trend was also found for the XRCC1 codon 194 Trp/Trp genotype (OR=2.15, 95% CI=0.87-5.34, p=0.099). The frequencies of the XRCC1 codon 399 Gln/Gln and Arg/Gln genotypes tended to be lower in lymphatic invasion-positive GC (XRCC1 codon 399 Gln/Gln: OR=0.27, 95% CI=0.06-1.15, p=0.075, Gln/Gln + Arg/Gln: OR=0.46, 95% CI=0.20-1.06, p=0.069), while the frequencies of the XRCC1 codon 194 Trp/Trp genotype tended to be higher in lymphatic invasion-positive GC (XRCC1 codon 194 Trp/Trp: OR=7.70, 95% CI=0.95-62.60, p=0.056). The patients with the GSTT1 null genotype showed significantly better overall survival than the patients with the GSTT1 present genotype (p=0.019). Conclusion: XRCC1 codon 194 Trp carrier status is correlated with more aggressive biological behavior of GC, such as venous invasion, and the GSTT1 null genotype is associated with better survival in GC patients.
Gastric cancer (GC) is one of the most common and lethal malignancies in Japanese and East Asian populations and the second most common cause of cancer-related deaths in the world (1, 2). Although the incidence and mortality rate of GC located outside the cardia have been decreasing over the last few decades, a considerable percentage of patients still have advanced disease at diagnosis and some of them are not indicated for curative surgery.
Although, several mechanisms may be related to susceptibility to GC development there is accumulating evidence that DNA repair or the xenobiotic pathway might be involved in these processes. X-Ray repair cross-complementing groups (XRCCs) are important proteins of the DNA repair pathways. The XRCC1 gene is responsible for a scaffolding protein that directly associates with other proteins such as DNA polymerase β, PARP (ADP-ribose polymerase) and DNA ligase III in a complex, to facilitate the processes of base excision repair (BER) or single-strand break repair (3). The BER pathway repairs DNA damage caused by a variety of endogenous and exogenous factors, including oxidation, alkylating agents and ionizing radiation (4, 5). The XRCC1 protein can bind directly to both gapped and nicked DNA, as well as to gapped DNA associated with DNA polymerase β, suggesting that this protein might be independently involved in DNA damage recognition (6). Two polymorphisms, more often found in the XRCC1 conserved sites, lead to a C to T substitution at codon 194 in exon 6 and to a G to A substitution at codon 399 in exon 10 of the gene, leading to the amino acid alterations arginine (Arg) to tryptophan (Trp) and arginine (Arg) to glutamine (Gln), respectively. These changes in conserved protein sites may alter the BER capacity, increasing the chances of DNA damage (7). Both the Arg399Gln, and Arg194Trp variants have been associated with cancer susceptibility (8-12), including GC (13-16).
Glutathione-S-transferases (GSTs) are important enzymes of the xenobiotic pathway. These enzymes catalyze the conjugation of potentially mutagenic electrophilic compounds, with nucleophilic glutathione yielding less toxic and more water-soluble compounds, which are readily excreted via urine or bile (17). Thus, GSTs protect the body from the harmful effects of carcinogens and a reduction of their activity can render an individual more susceptible to various carcinomas (18). Both GSTT1 and GSTM1 genes of the GST super gene family exhibit null or deletion polymorphism (18, 19). Individuals homozygous for the null allele lack GST enzyme activity and hence have an increased risk of cancer (18). GSTP1 also exhibits a polymorphism within its coding region, leading to an A to G substitution at codon 104 of the gene, leading to the amino acid alteration isoleucine (Ile) to valine (Val), which reduces enzyme activity (20). GSTM1, GSTT1 and GSTP1 polymorphisms have also been studied in several malignancies including GC (21-24).
Because of their important roles in DNA repair and the xenobiotic pathway, a number of studies have evaluated the association between XRCC1 and GST polymorphisms with susceptibility to GC (13-16, 23, 24). In addition, several studies have also investigated the association between these polymorphisms and survival in GC patients, using anticancer drugs (25, 26).
Since XRCC1 and GST polymorphisms might have important roles in cancer development, we speculated that these biological polymorphisms may also be associated with distinct behavior of GC. In this study, the association between XRCC1 Arg399Gln and Arg194Trp, GSTP1 Ile104Val, and GSTT1 and GSTM1 null polymorphisms and various clinicopathological characteristics of GC and overall survival were evaluated in a Japanese population.
Patients and Methods
Patients, DNA extraction, and Helicobacter pylori infection status. The studied population comprised 130 patients with GC being treated in our hospitals. All GC cases were diagnosed histologically and were classified according to Lauren's classification. Detailed information was obtained concerning anatomic location, lymph node and distant metastasis, and peritoneal dissemination. Information on venous, and lymphatic invasion was also obtained in 100 out of 107 resected cases. Based on this information, early GC was defined as localized within the mucosa or submucosa, irrespective of lymph node metastasis and all others were defined as advanced GC.
Clinicopathological characteristics of GC patients.
Among 128 patients, including 23 unresectable and 105 resectable cases, overall survival, defined as the time from the date of surgery for resectable cases and the date of initial chemotherapy for unresectable cases, was recorded. H. pylori infection status was assessed by serologic or histological analysis, or urea breath test. Patients were diagnosed as infected when at least one of the diagnostic tests was positive. The Ethics Committee of the Fujita Health University School of Medicine approved the protocol, and written informed consent was obtained from all the participating subjects.
Genotyping for polymorphisms. Genomic DNA was extracted from uninvolved mucosa of the gastric antrum or peripheral blood using the standard phenol/chloroform method in all the patients.
Genotyping for the XRCC1 gene codons 399 and 194, and GSTP1 polymorphisms were carried out by multiplex PCR-RFLP, as previously described (9, 27), while the GSTT1 and GSTM1 null polymorphisms were detected by PCR, using exon 7 of the constitutional CYP1A1 gene as internal control, as previously described with slight modifications (28). Instead of multiplex PCR, genotyping for GSTT1 and GSTM1 was conducted separately.
Statistical analyses. Genotype frequencies were calculated by direct counting. Logistic regression analysis with adjustment for sex and age was used to assess the association between the clinicopathological characteristics and the genotypes. Survival among different genotypes was assessed using the Kaplan–Meier method and compared using the log-rank test. A probability value of less than 0.05 was considered as statistically significant.
Results
Characteristics of subjects, association between XRCC1 codons 399 and 194, GSTP1, GSTT1, and GSTM1 polymorphisms and clinicopathological characteristics of GC. The characteristics of the 130 GC patients are shown in Table I, and the association between XRCC1 codons 399 and 194, GSTP1, GSTT1 and GSTM1 polymorphisms and the clinicopathological characteristics of GC are shown in Table II. The GSTT1, and GSTM1 polymorphisms were successfully genotyped for all the patients. The XRCC1 codon 399 and 194 polymorphisms could not be genotyped for two patients. The GSTP1 polymorphism could not be genotyped for one patient. The frequencies of the XRCC1 codon 399 Gln/Gln and Arg/Gln genotypes tended to be lower in lymphatic invasion-positive GC (XRCC1 codon 399 Gln/Gln: OR=0.27, 95% CI=0.06-1.15, p=0.075, Gln/Gln + Arg/Gln: OR=0.46, 95% CI=0.20-1.06, p=0.069). On the other hand, the frequency of the XRCC1 codon 194 Trp/Trp genotype tended to be higher in lymphatic invasion-positive GC (XRCC1 codon 194 Trp/Trp: OR=7.70, 95% CI=0.95-62.60, p=0.056). XRCC1 codon 194 Trp carriers (Trp/Trp + Arg/Trp) held a significantly higher risk of venous invasion (OR=3.76, 95% CI=1.05-13.51, p=0.043). A similar trend was also found for the XRCC1 codon 194 Trp/Trp genotype (OR=2.15, 95% CI=0.87-5.34, p=0.099). As shown in Table II, no significant association was found between the XRCC1 codon 399 and 194, GSTP1, GSTT1 and GSTM1 polymorphisms and staging, lymph node metastasis and peritoneal dissemination. Moreover, no association was found between the XRCC1 codon 399 and 194, GSTP1, GSTT1, and GSTM1 polymorphisms polymorphisms and the other clinico-pathological subtypes, such as Lauren's histological classification, anatomical location, liver and other distant metastasis (data not shown).
Associations between XRCC1, GSTP1, GSTT1 and GSTM1 polymorphisms and various clinicopathological subtypes of GS.
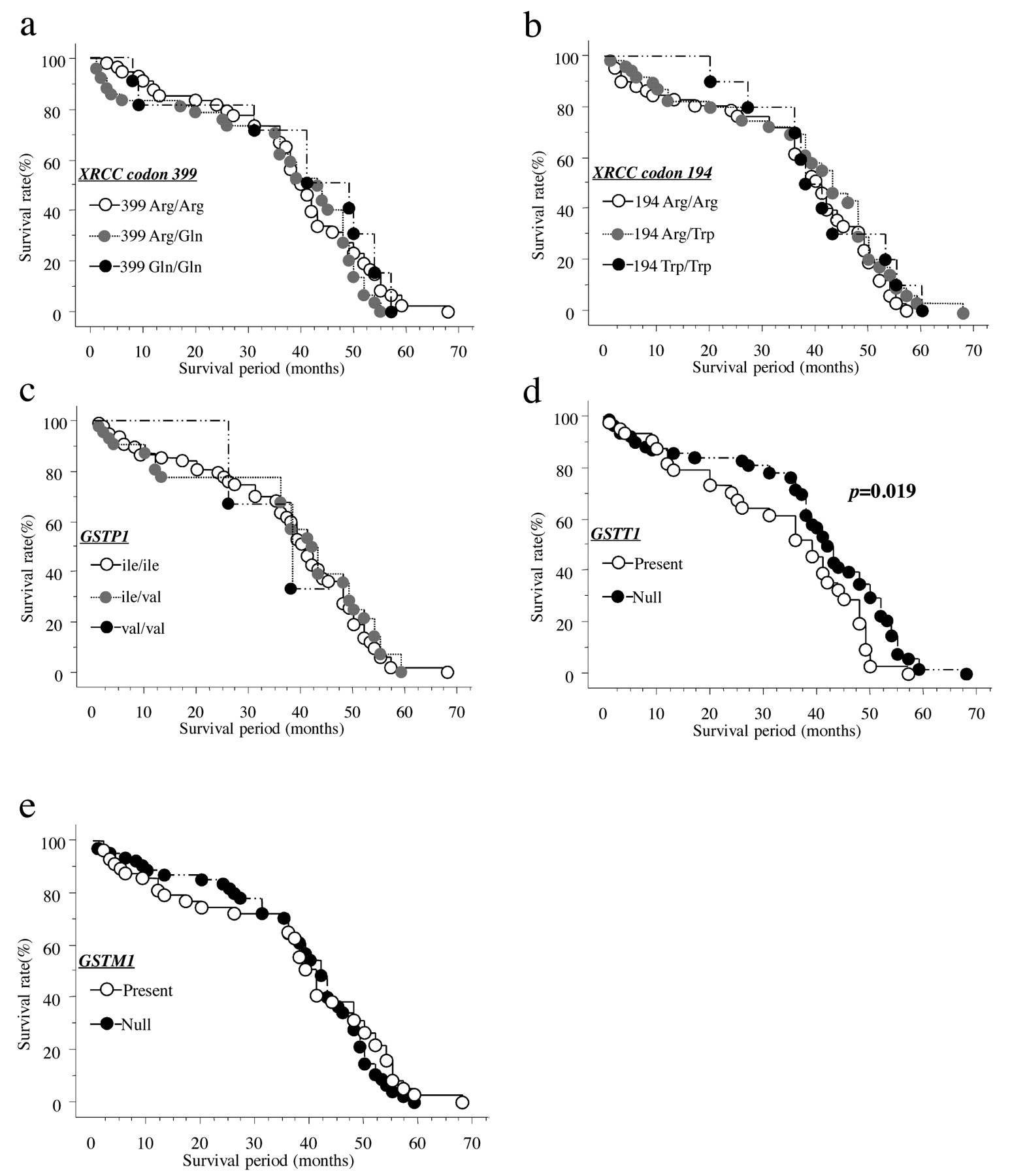
Association between survival curves estimated by the Kaplan-Meier method, and XRCC1 codon 399 and 194, GSTP1, GSTT1, and GSTM1 polymorphisms. The median follow-up period of the 128 assessed patients was 30.0 months. Among the 23 unresectable patients, TS-1-based chemotherapy was administered in 15 cases, taxane-based chemotherapy in five cases, and chemotherapy with other regimens in remaining three patients. The patients with the GSTT1 null genotype showed significantly better overall survival than the patients with GSTT1 present genotype (p=0.019: Figure 1d), while no association was found between the other genotypes (XRCC1 codons 399 and 194, GSTP1 and GSTM1) and overall survival (Figure 1 a-c, e).
Discussion
XRCC1 codon 194 Trp carriers (Trp/Trp + Arg/Trp) held a significantly higher risk of venous invasion and a similar trend was also found for the XRCC1 codon 194 Trp/Trp genotype with both venous and lymphatic invasion. These associations indicated that different GC subtypes may have different genetic backgrounds and the XRCC1 codon 194 genotype may lead to distinct biological behavior such as venous invasion-positive phenotypes. The XRCC1 codon 194 Trp allele may thus be associated with more aggressive pathological phenotypes in GC. On the other hand, no association was found between the other polymorphisms and the GC characteristics, except for a weak association between the XRCC1 codon 399 Gln/Gln and Arg/Gln genotypes with reduced risk of lymphatic invasion-positive GC, suggesting a weak effect of these polymorphisms on biological behavior in GC. Inconsistent results have been observed regarding the XRCC1 194 Arg and 399 Gln alleles in relation to GC. Lee et al. (14) reported that the haplotype combining XRCC1 194 Trp, 280 Arg and 399 Arg was associated with a significant reduction in GC risk in Korea, while Huang et al. (16) showed an association between the greatest smoking-associated GC risk and the 399 Arg/Arg genotype, but not the 194 genotypes in Poland. The 194 Arg/Arg genotype was associated with a significantly increased risk for cardiac GC in China (13), while another study in North Central China showed that the XRCC1 399 Gln allele was associated with reduced risk of cardiac GC and the 194 genotype alone was not associated with cardiac GC (15). More recently, Capellá et al. (29) showed that the XRCC1 399 Gln allele was associated with increased risk of severe gastric atrophy, but association was not observed for the 194 genotypes. These discrepancies may be due to population stratification and different characteristics of the patients, or to the XRCC1 polymorphism being linked to the real disease-causing variant(s). Together with the current result, it is clear the XRCC1 genotype may have differing effects on GC susceptibility and progression in different populations, and anatomical locations (cardia and non cardia), reflecting the diversity of the environmental or etiological factors.
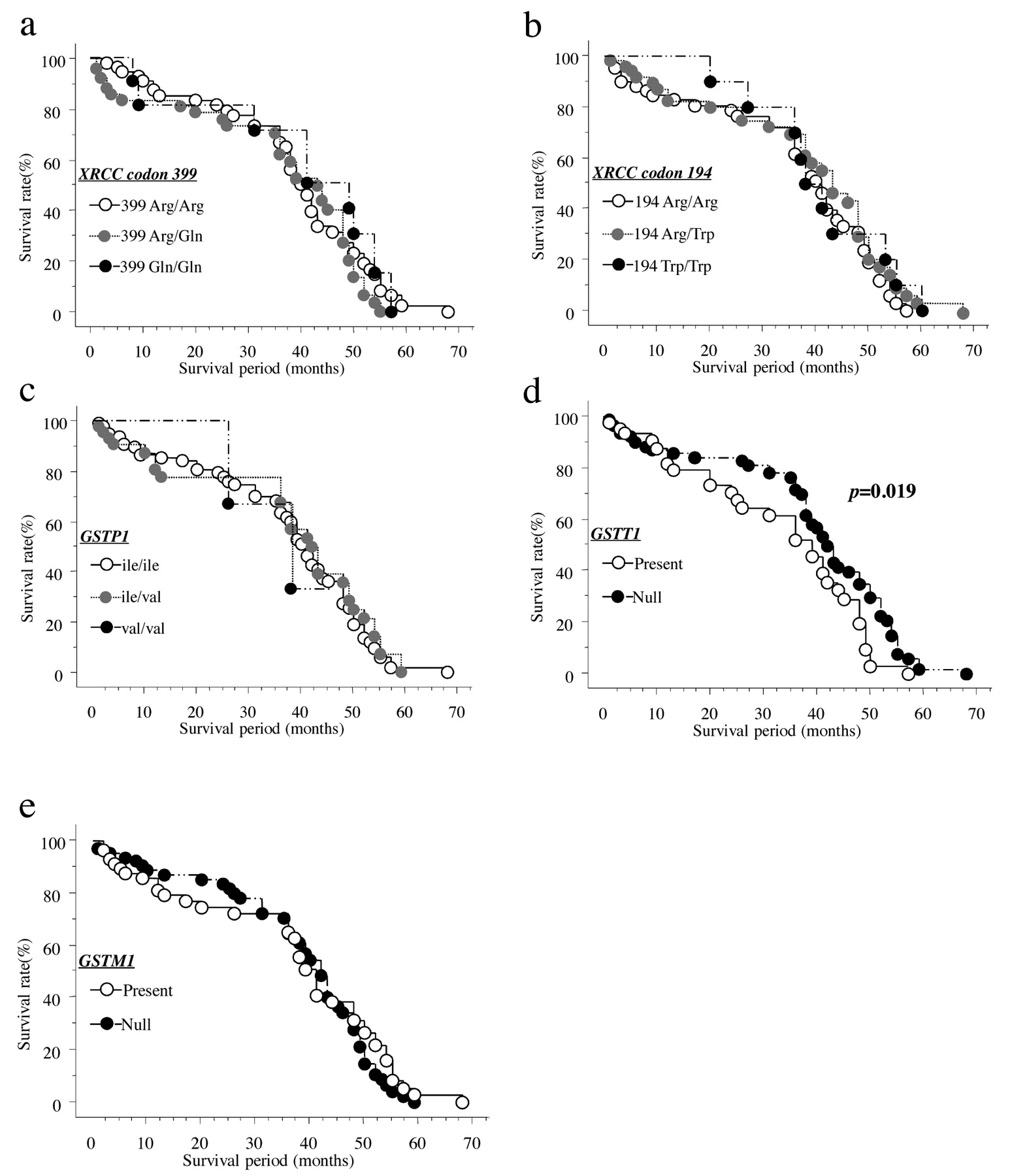
Association between survival curves estimated by Kaplan-Meier method, with different XRCC1 codons 399 and 194, GSTP1, GSTT1 and GSTM1 genotypes (n=128). Statistical analysis was performed by the log-rank test.
The patients with the GSTT1 null genotype showed significantly better overall survival than the patients with the GSTT1 present genotype. The deletion genotype in GSTT1 has also been shown to be associated with poorer prognosis in GC (25). However, in this study, the low enzymatic activity, GSTT1 null-genotype was associated with rather superior overall survival. Three speculative explanations for the association between the null genotype and improved survival are possible. First, GSTT1 may have a role in metabolizing certain substances which have a protective effect against cancer, and the null genotype may increase the concentration of these substances and, thus, may be associated with superior overall survival. Second, this polymorphism may be in linkage disequilibrium with other polymorphisms elsewhere in the GSTT1 gene, which influence the overall survival in GC patients, demonstrating biologically relevant variability. Finally, this polymorphism may be in linkage disequilibrium with a genetic variation of another gene located near the GSTT1 gene that is related to overall survival in GC patients.
Since, the effect of the GSTT1 polymorphisms in GC were confirmed by a recent meta-analysis, especially in the Asian population (24), and studies investigating the association between GST polymorphisms and overall survival in GC have been relatively rare, a longitudinal study will be needed, with larger, and ethnically diverse cohorts to confirm the present results.
In summary, XRCC1 codon 194 Trp presence is correlated with a higher risk of venous invasion in GC patients. Furthermore, the GSTT1 null genotype is significantly associated with better survival in GC patients. GC may have different biological behavior in individual tumors, and this may lead to various clinical phenotypical prognoses. Furthermore, genetic differences between the patients in the presence of malignant tumor may also affect the outcome. Thus, it may be necessary to place greater emphasis on the heterogeneity within a tumor, as well as host genetic differences. The potential usefulness of XRCC1 and GSTT1 polymorphisms as molecular markers for physicians to conduct more appropriate clinical management of GC is demonstrated.
- Received November 1, 2010.
- Revision received January 27, 2011.
- Accepted January 25, 2011.
- Copyright© 2011 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.