


Abstract
Background: The objective of this study was to evaluate the recurrence-preventing effect of intravesical instillations of interleukin-2 (IL-2) in patients with non-muscle-invasive bladder carcinoma. In addition, this study aimed to determine the significance of immune parameters for recurrence-free interval. Patients and Methods: Twenty-six patients with non-muscle-invasive bladder carcinoma were treated with intravesical instillations of IL-2 (Proleukin®, Novartis, formerly Chiron) in doses of 9×106 IU on 5 consecutive days, beginning on the second day after transurethral resection (TUR) of tumours. CD8highCD57+ lymphocytes in peripheral blood were determined before TUR and compared with the recurrence-free interval after treatment. Results: The multivariate analysis showed that CD8highCD57+ lymphocytes had a prognostic significance in combination with number of bladder tumours, prior recurrence rate and age of patients. Conclusion: Peripheral blood CD8highCD57+ lymphocytes have prognostic significance for recurrence-free survival in patients with non-muscle-invasive bladder carcinoma after TUR and intravesical IL-2.
Non-muscle-invasive bladder tumours can be removed by transurethral resection (TUR). However, the main problem is the high recurrence rate, ranging from 15% to 61% at one year after TUR. In addition, these tumours progress within one year to muscle-invasive disease in up to 17% of patients (1).
A number of reports indicate activity of local application of interleukin-2 (IL-2) in treatment of non-muscle-invasive bladder carcinoma. Regression of bladder tumours has been observed after intralesional injections (2), instillations (3, 4) or continuous bladder perfusion (5) with IL-2. Using intravesical instillations of IL-2, Den Otter et al. achieved regression of marker lesions left in place after TUR in eight out of ten patients (6). While regression of bladder tumours after similar intravesical instillations of IL-2 was not observed by Grasso et al. (7), these authors reported a decrease in the recurrence rate.
Based on results of earlier studies with local IL-2 in patients with non-muscle-invasive bladder carcinoma, this study designed and carried out a phase II trial to evaluate the recurrence-preventing effect of intravesical instillations of IL-2 after TUR.
Non-muscle-invasive bladder carcinoma is generally regarded to be sensitive to immune reactivity: this is mainly thought to be because it is sensitive to BCG (8). It is unknown, however, whether and which immune parameters are involved in the development of non-muscle-invasive bladder carcinoma and whether they influence the length of time between TUR and tumour recurrence.
In a previous study by this group, a panel of lymphocyte subsets (CD3+, CD19+, CD16&56+, CD4+, CD8+, CD4+CD45ROhigh and CD8highCD57+) in peripheral blood of advanced renal cell carcinoma patients was analysed in an attempt to find their significance for predicting survival (9). The only lymphocyte subset that was found to be of significant importance in determining survival of advanced renal cell carcinoma patients (both untreated and treated with interferon-α) was CD8highCD57+ lymphocytes. In another study, the prognostic significance of these lymphocytes in melanoma patients treated with adjuvant interferon-α was investigated (10). Levels of CD8highCD57+ lymphocytes in peripheral blood increase during recurrences of bladder carcinoma (11). For these reasons, this study aimed to measure numbers of CD8highCD57+ lymphocytes in the peripheral blood of bladder carcinoma patients before TUR and to investigate the correlation of these values with the recurrence-free interval after intravesical treatment with IL-2.
CD8highCD57+ lymphocytes clonally expand in a variety of clinical disorders associated with chronic antigenic stimulation (12). These cells represent a terminal differentiation state of effector T lymphocyte populations which are enriched in antigen-specific T-cells and down-modulate their own cytolytic potential (13).
Patients and Methods
Patients. The phase II study protocol was approved by the Lithuanian Bioethics Committee and State Medicines Control Agency of Lithuania (trial registration: EudraCT:2004-002821-30). Consecutive patients with histologically confirmed Ta-T1/G1-G3 non-muscle-invasive bladder carcinoma (not in the prostatic urethra or in a diverticulum) were included in the trial. All patients gave written informed consent. Criteria for exclusion were the following: white blood cells <3,000/mm3 or platelets <100,000/mm3; hepatic enzymes (SGOT, SGPT, alkaline phosphatase) or creatinine >2× normal values; previous chemotherapy or radiotherapy within 3 months before treatment; previous or concurrent cancer at other sites; urinary tract infection.
Treatment. Starting from the second day after TUR, patients were treated for five consecutive days with intravesical instillations containing 9×106 IU recombinant IL-2 (Proleukin®, Chiron, nowadays Novartis, Amsterdam, the Netherlands). IL-2 was diluted in 50 ml saline (0.9% NaCl) and instilled in the bladder through a catheter, which was removed after the instillation. The drug remained in the bladder for one to two hours.
FACS analysis of peripheral blood lymphocyte subsets. Prior to TUR peripheral blood samples were collected for flow cytometric analysis. The samples of peripheral blood were analysed on a FACSort® (Becton Dickinson, Heidelberg, Germany) flow cytometer with a laser tuned at 488 nm. The lymphocytes were stained with CD57-FITC/CD8-PE combination of fluorochrome-conjugated monoclonal antibodies (Becton Dickinson). Forward and side scatter were used to gate the lymphocytes. List mode files were collected for 10,000 cells from each sample. Data were acquired and analysed with Cell Quest software (Becton Dickinson). Percentages of CD8highCD57+ lymphocytes in the CD8+ subset were determined in the flow cytometric CD57-FITC/CD8-PE dot plot. CD8+ lymphocytes with high or low expression of CD8 antigen were identified as described in our previous publication (9). Absolute counts of white blood cells were determined in lysed blood with a haemocytometer and used for calculation of absolute numbers of CD8highCD57+ lymphocytes (numbers of cells/μl peripheral blood).
Patients characteristics.
Follow-up and statistics. The first follow-up cystoscopy was performed at two months after TUR. Further cystoscopies were performed at periodic follow-up visits to the urologist. All suspicious lesions were resected and examined histologically. The recurrence-free interval was measured in days from the date of TUR until the first observed recurrence. Multiple potential cut-off points of CD8highCD57+ lymphocyte values were examined using the method of Contal and O'Quigley (14). For cut-off point determination, an SAS macro provided by Mandrekar and colleagues was applied (15, 16). Multivariate analysis was performed by the Cox proportional hazards model. Statistical analyses were performed using SAS version 9.1.3 (SAS Institute, Cary, NC, USA).
Results
The characteristics of patients are shown in Table I. Twenty-six consecutive patients with histologically confirmed non-muscle-invasive bladder carcinoma were enrolled from May 2005 to June 2006. There were 5 females and 21 males with the median age of 66 years (range 43 to 92 years). Six patients had TaG1 tumours, 14 patients TaG2 tumours, 4 patients TaG3 tumours and 2 patients T1G3 tumours. Ten patients had primary non-muscle invasive bladder cancer and 16 patients had a history of the disease of 2 months – 6 years. IL-2 instillations into the bladder were well tolerated. There was no local or systemic toxicity, including febrile or flu-like episodes.

Kaplan-Meier recurrence-free survival curve of 26 study patients with non-muscle-invasive bladder carcinoma treated with TUR followed by 5 daily intravesical instillations of IL-2.

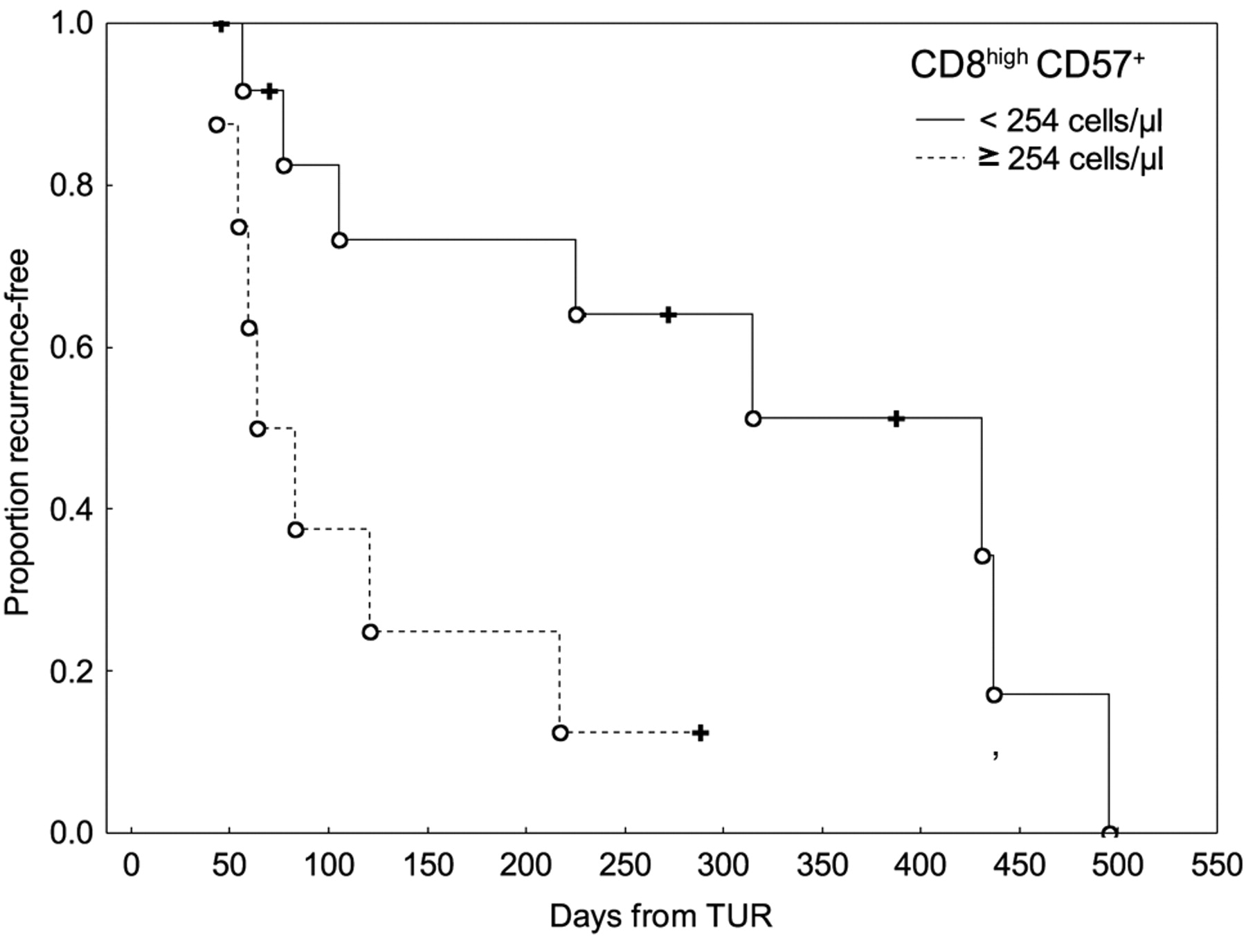
Kaplan-Meier recurrence-free survival curves of patients with non-muscle-invasive bladder carcinoma with <254 (n=13) or ≥254 (n=8) CD8high57+ lymphocytes/μl in peripheral blood prior to treatment (p=0.1408). Patients were treated with TUR followed by 5 daily intravesical instillations of IL-2.
Multivariate analysis of time to first recurrence in bladder carcinoma patients after TUR and IL-2 instillations.
The Kaplan-Meier curve of recurrence-free survival of 26 study patients is shown in Figure 1. The median recurrence-free survival of all IL-2-treated patients with non-muscle invasive bladder cancer was 201 days. The shortest recurrence-free interval was 43 days, whereas the last recurrence was observed at 509 days after TUR. Seven patients still had no recurrence at a mean follow-up of 272 days.
Twenty-one out of 26 patients were evaluable for CD8highCD57+ lymphocyte counts in peripheral blood before TUR. The recurrence-free survival of IL-2-treated bladder carcinoma patients according to CD8highCD57+ lymphocyte count in peripheral blood is shown in Figure 2. The median recurrence-free interval of patients with <254 CD8highCD57+ lymphocytes/μl was 324 days compared to 64 days of patients with ≥254 CD8highCD57+ lymphocytes/μl.
To determine the relative prognostic importance of CD8highCD57+ lymphocyte count, this variable was entered into multivariate analysis in combination with tumour grade (G1, G2, G3), number of tumours (multiple versus single), prior recurrence rate/year (>1 recurrence/year or primary versus≤1 recurrence/year), age and gender of patients. No statistically significant cut-off was found for values of CD8highCD57+ lymphocytes that would categorize patients into subgroups with different hazard ratio for recurrence (p=0.1408). Thus, CD8highCD57+ lymphocytes were entered into multivariate analysis as a continuous variable. Table II shows that the CD8highCD57+ lymphocyte count has a prognostic significance for recurrence-free interval in combination with three clinical and demographic factors: number of tumours, prior recurrence rate and age of patients. Tumour grade and gender did not fit into the model with statistical significance.
Discussion
The median time to first recurrence of 201 days (6.6 months) in this study is similar to that of 5 months reported in patients with superficial bladder carcinoma who did not receive intravesical treatment after TUR (17). Thus, despite the fact that this study does not have a proper control group, it is concluded that it is unlikely that intravesical instillations of IL-2, as used in this study, can clinically significantly prolong the median time to first recurrence in unselected non-muscle-invasive bladder carcinoma patients.
This apparent lack of antitumour effect of intravesical IL-2 instillations is rather unexpected in regard to the impressive therapeutic results of Den Otter et al. (6). A few differences between these two studies might explain the seemingly contradictory results. First, in the present study, three-fold higher doses of IL-2 were used and 0.1% human serum albumin was not added to the solution. Thus, pharmacology and bioavailability of IL-2 may have been different in the two studies. Second, in the study of Den Otter et al. (6) the marker lesion was left in the urinary bladder after incomplete TUR. The marker lesion may have had tumour-associated antigens which may have been necessary for the development of tumour-specific immunity (18).
Although in this study it was not possible to demonstrate a therapeutic effect of IL-2, the results show that the time to first recurrence is strongly related to pre-treatment immune parameter values, namely CD8highCD57+ lymphocyte count in peripheral blood.
The probability of recurrence in patients with non-muscle-invasive bladder carcinoma depends on a number of clinical, pathologic and demographic factors, the most important of them being prior recurrence rate, number of tumours, tumour size, T category and grade (1). Therefore, a multivariate analysis was performed to determine the relative prognostic significance CD8highCD57+ lymphocyte count. Grade, number of tumours, prior recurrence rate, gender and age of patients were entered into the analysis. The great majority of patients in our study had tumours of Ta category (only 2 out of 26 patients had T1 tumours), the data on the size of tumours were not available.
CD8highCD57+ lymphocyte count showed a prognostic significance for recurrence-free interval in combination with number of tumours, prior recurrence rate and age of patients. Thus, immune parameters may be important in combination with clinical and demographic factors in predicting the recurrences in patients with non-muscle-invasive bladder carcinoma. It has been shown that tumour infiltration by CD8+ lymphocytes has prognostic significance for survival in muscle-invasive urothelial carcinoma (19). Our results show that subsets of CD8+ lymphocytes in peripheral blood may also carry prognostic information.
The present study was a phase II study not including a control group of patients not reated with IL-2. Thus, the question remains open whether the observed relationship between CD8highCD57+ lymphocyte count and the recurrence-free interval is related to treatment with IL-2 or to the natural course of bladder carcinoma. However, some evidence suggests that high counts of CD8highCD57+ lymphocytes may impede the effect of IL-2 therapy. Expression of CD57+ antigen on CD8+ T lymphocytes reduces their proliferate response to IL-2 considerably (20). Moreover, CD8highCD57+ lymphocytes may also exert a suppressive action on other T lymphocyte subsets (21). Thus, anergic/suppressive properties of CD8highCD57+ lymphocytes may explain why high counts of these lymphocytes are associated with short recurrence-free interval of IL-2-treated non-muscle-invasive bladder carcinoma patients.
In conclusion, the results of this study show that peripheral blood CD8highCD57+ lymphocytes may have prognostic significance for recurrence-free survival in patients with non-muscle-invasive bladder carcinoma after TUR and intravesical instillations of IL-2. This evidence adds to the growing body of data indicating the utility of CD57 expression in T lymphocytes to evaluate the immune status of cancer patients (9, 10, 11, 22, 23). Although it was not possible to demonstrate a therapeutic affect of IL-2 on the whole population of unselected patients, it cannot be excluded that intravesical IL-2 may have prevented tumour recurrences in a subset of patients with low levels of CD8highCD57+ lymphocytes in peripheral blood.
Acknowledgements
The study was supported by a grant from the Lithuanian State Science and Studies Foundation and by a grant from SNFK, Amsterdam, the Netherlands.
- Received December 31, 2010.
- Revision received January 25, 2011.
- Accepted January 25, 2011.
- Copyright© 2011 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- High Numbers of Circulating CD57+ NK Cells Associate with Resistance to HER2-Specific Therapeutic Antibodies in HER2+ Primary Breast Cancer
- Role of Marker Lesion when Applying Intravesical Instillations of IL-2 for Non-muscle-invasive Bladder Cancer Comparison of the Therapeutic Effects in Two Pilot Studies
- Prediction of Response in Cancer Immunotherapy