


Abstract
Hyperostosis is the most common skull change associated with meningioma. Five hyperostosis cases of meningioma en plaque infiltrating the skull processed without previous decalcification of the bone tissue were investigated histologically and immunohistochemically with antibodies against somatostatin receptor 2A (SSR2A). Undecalcified bone biopsies embedded in methylmethacrylate and paraffin-embedded extraosseous tumor tissues were analyzed. All five cases were well-differentiated meningotheliomatous meningiomas en plaque according to the WHO classification of tumors and revealed areas of hyperosteoidosis. Furthermore, all five meningiomas en plaque presented strong positive reactions to antibodies against SSR2A in both the intraosseous and extraosseous tumor proliferates. In summary, similar morphological changes characterized by hyperosteoidosis were observed in a small cohort of meningioma en plaque associated with expression of SSR2A and reports in the literature of the histogenesis of hyperostosis in meningioma en plaque are discussed.
Meningiomas represent about 20% of all intracranial tumors, with a clear predominance in women (1). Meningioma en plaque is characterized by an indolent growth of sheets and whorls of neoplastic infiltrate associated with hyperostosis. This term was given by Cushing and Eisenhardt (2) to differentiate these meningiomas from the more common form called meningioma en masse. In meningioma, hyperostosis is a well-known sign of tumor, and is observed in 4.5% of all types, but is more frequently present in meningioma en plaque with an occurrence of 13% to 49% (3). Primary intraosseous meningioma induces hyperostosis in 60% of cases (4). The precise mechanisms of hyperostosis and intralesional morphological changes of the bone associated with meningioma remain unclear.
The neuropeptide somatostatin plays various biological roles in the brain (5), as well as in many other parts of the body. It is a powerful inhibitor of pituitary and gastroenteric hormone secretion (6-7), while it also plays a role as a neurotransmitter/neuromodulator in the central nervous system (8). These functions are mediated through the selective activation of high affinity somatostatin receptors, which are members of the seven helix membrane-spanning receptor superfamily coupled to GTP-binding proteins (9). While the expression of somatostatin receptors in meningiomas has already been reported (10), the effects of somatostatin on these tumors are still controversial (10). Among the somatostatin receptor subtypes, somatostatin receptor 2A (SSR2A) expression has frequently been observed in meningiomas in both immunohistochemical and RT-PCR analyses (10, 12-14).
The objective of the current study was primarily to investigate the morphological changes within the bone infiltrated by meningioma en plaque and secondly, to analyze the expression of SSR2A within the intraosseous proliferating en plaque meningioma.
Patients and Methods
Study cohort. The databases of both the Institute of Pathology and the Institute of Neuropathology of the University Medical Center Hamburg-Eppendorf were searched for cases of en plaque meningioma with both methylmethacrylate-embedded undecalcified bone tissues and paraffin-embedded soft tissues without decalcification obtained from en plaque meningioma. Five cases of meningioma en plaque (Table I) diagnosed in both institutions from 2006 to 2009 were identified.
Histology and immunohistochemistry. The tissues were fixed in formalin immediately after the surgical procedure. Surgical specimens from the diploe of the skull were sectioned by means of a water-cooled diamond band saw and contact radiographed. Multiple samples from each lesion, including both the central and lateral parts of the osseous lesion, were embedded in methylmethacrylate without decalcification and stained by Goldner's trichrome staining and periodic acid-Schiff reaction. Soft tissue samples removed from tumor masses within the adjacent intracranial tissue were embedded in paraffin and stained with hematoxylin-eosin stain and with periodic acid-Schiff reaction.
Immunohistochemical analyses were performed on both bone and soft tissue samples using EMA (clone E29, Dako M0613; Glostrup, Denmark; dilution 1:50) in order to confirm the conventional histopathological diagnosis, Ki-67 (clone Mib-1, Dako M7240, dilution 1:400) in order to assess the proliferative tumor fraction, and somatostatin receptor (clone SSR2A; Gramsch Laboratories, Schwabhausen, Germany, dilution 1:1,000) antibodies. Both the staining intensity (absent, weak, moderate, strong) and the staining patterns (focal, diffuse) were recorded. Staining each sample without adding anti-human primary antibody was performed as a negative control.
Results
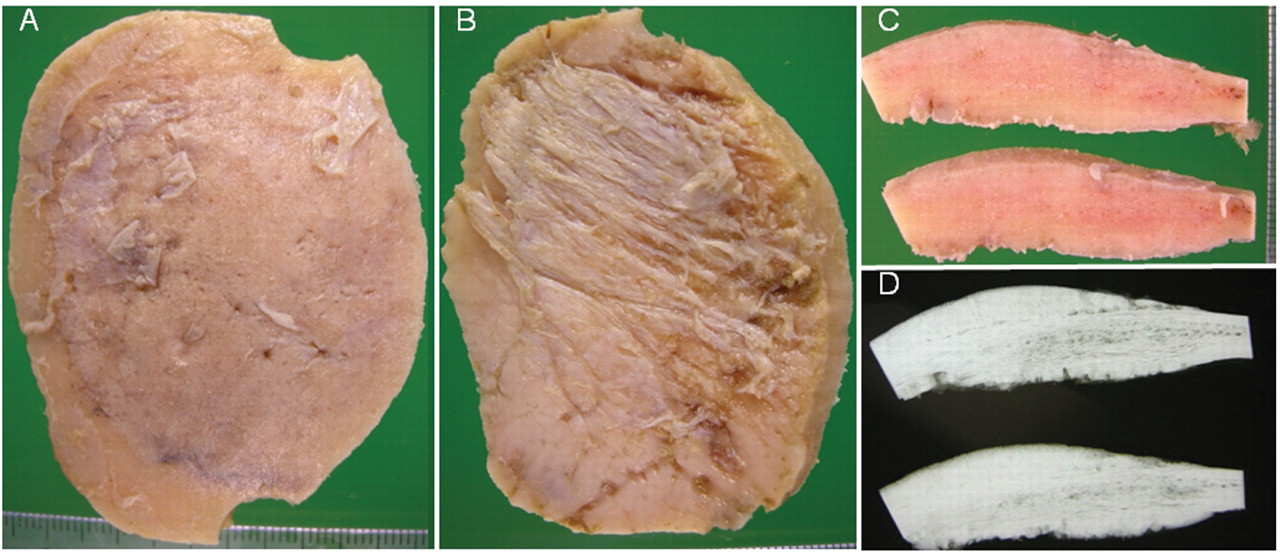
The surgically removed osseous specimens showed a circular swollen diploe with a discrete granular or folded outer surface (Figure 1A) and irregular ingrown fibrous tissues and fragmented adherent dura on the inner surface (Figure 1B). A flat thickening of the diploe was seen on the cutting plane (Figure 1C). In the contact radiography, dense mineralized periosteal new bone formation was apparent on both surfaces of the diploe, associated with discrete irregular remodeling of both the cortical and cancellous bone of the skull (Figure 1D). A focal radiolucent line between the cortex and the newly formed periosteal mineralized bone tissue was also apparent.
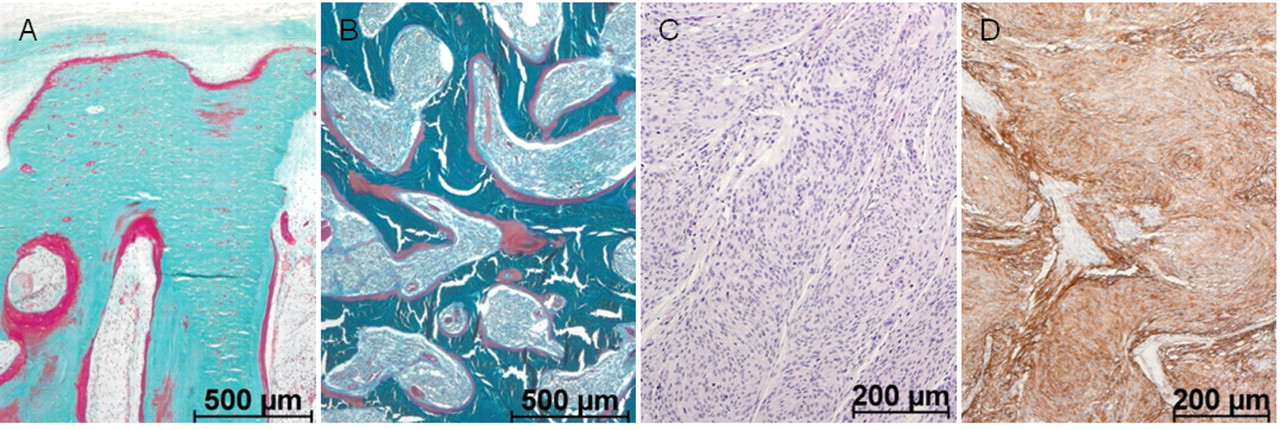
Histologically (Table II), multifocal intraosseous meningothelial neoplastic infiltration was apparent throughout the macroscopically thickened bone including the newly formed periosteal bone (Figure 2A), cortical and cancellous (Figure 2B) osseous tissue. A focal superficial spread of tumor proliferations arranged in sheets and whorls was found on the inner surface of the removed bone. Multifocal widening of osteoid and so-called buried osteoid (14) were found in each case (Table II). In three cases, deep resorption lacunae occupied by enlarged osteoclasts were recognized. Interestingly, none of the study cases presented psammoma bodies. All the cases were diagnosed as meningothelial meningioma according to the WHO classification (Figure 2C) associated with osseous infiltration and hyperostosis. The mitotic activity was less than four mitotic figures in ten high-power fields in all cases. Cellular atypia and tumor necrosis were not present.
Immunohistochemically, each tumor revealed moderate to strong positive reaction with antibodies against EMA and SSR2A (Table II, Figure 2D). The proliferative activity ranged from 4.2 to 9.1% as determined by the Ki-67 labeling index (Table II).
Meningioma en plaque. Study group demographics.
Discussion
Several common histopathological characteristics were observed in the study cohort. All the cases presented with infiltration of all three layers of the calvarium (16) and with new periosteal bone formation on both the inner and outer bone surfaces. In agreement with Kim and coauthors (17), focal patches of non-neoplastic dura were found on the inner surface of the corticalis which was discontinuously overgrown by the tumor and presented radiographically as a radiolucent line. While each case from the study cohort showed distinct areas of hyperosteoidosis consistent with oncogenic osteomalacia, psammomatous calcifications were not present. Interestingly, three cases also presented with pathological bone resorption similar to the morphological findings in secondary hyperparathyroidism.
One of the most surprising outcomes of the current study was the observation of focal hyperosteoidosis similar to oncogenic osteomalacia associated with a strong reaction of the intraosseous tumor infiltrate with antibodies against the SSR2A. While immunohistochemistry on methyl-methacrylate-embedded bone tissue is not performed routinely; for the purposes of the present study, both the osseous and extraosseous soft parts of the tumors were analyzed simultaneously. Clearly, the bone-infiltrating meningioma tissue exhibited the same strong SSR2A reactivity as found in the extraosseous tumor proliferation. Even though immunohistochemistry on paraffin-embedded tissues is preferable, reliable staining results were achieved in all the methylmethacrylate-embedded specimens. While SSR2A reactivity has frequently been observed in higher grade meningiomas, seven out of thirteen grade 1 tumors have also been reported to show positive results (18).
The osseous hyperostosis associated with meningioma en plaque has traditionally been characterized by indolent growth (19) and sclerotic changes of the adjacent bone (19). Although several distinct patterns of osseous changes in meningioma en plaque have been defined radiographically (16), histopathological analyses of bone-infiltrating meningioma are quite rare. According to the literature (3, 20-24), the tumors seem to be differentiated in a similar manner to the usual meningiomas of meningothelial type, but, morphological changes of the bone tissue infiltrated by the meningioma have not previously been analyzed. Earlier studies of the radiographical features (16, 21) of osseous characteristics of meningioma en plaque primarily focused on both the location and pattern of osseous changes. Histopathological analyses have clearly demonstrated intraosseous infiltration of the tumor in areas of characteristic hyperostosis (3, 20-23). Nonetheless, the histogenesis of osseous changes associated with this particular tumor remains uncertain. While Freedman and Forster believed that bone growth in cranial hyperostosis associated with meningioma was a function of the tumor cells (25), most other authors (17, 26-27) agreed with Cushing's conclusion that the tumor stimulates osteoblastic activity resulting in the hyperostosis (28). Kim and coauthors (16) suggested that the new bone growth probably resulted from periosteal stimulation via invasion by the tumor. More recently, Heick and coauthors (29) postulated that differences in neoplastic humoral mechanisms, particularly in the enzymatic activity of hyperostosing and non-hyperostosing types of meningioma were causative. Based on the present results, it can be speculated that local hormonal regulation of bone metabolism associated with intraosseous tumor infiltration might possibly contribute to formation of the characteristic hyperostosis related to meningioma en plaque. Interestingly, it has recently been shown that another neuropeptide serotonin importantly influences bone metabolism (30-34). Although serotonin is synthesized by two distinct genes centrally and peripherally (35) without crossing the blood–brain barrier, the pharmacological inhibition of gut-derived serotonin synthesis seems to be potentially useful in the therapy of osteoporosis (31).

Meningioma en plaque (gross findings and contact radiographs of the specimen). Macroscopically, (A) the outer bone surface, granular but smooth with pink coloration; (B) the inner surface, somewhat irregular with ingrown tumor and fragmented dura. (C) Cut surface, the bone tissue within the hyperostosis associated with meningioma en plaque more uniform (mid portions) compared with the lamellar structure of the diploe of the neighboring calvarium (lateral portions). (D) Contact radiographically, similarly dense mineralization within the newly formed periosteal bone proliferation and remodeled diploe with tumor infiltration (mid portions). When compared with the outer surface, the inner one appeared rough and more irregular. Focal radiolucent line between the periosteal new bone formation and original corticalis is apparent.
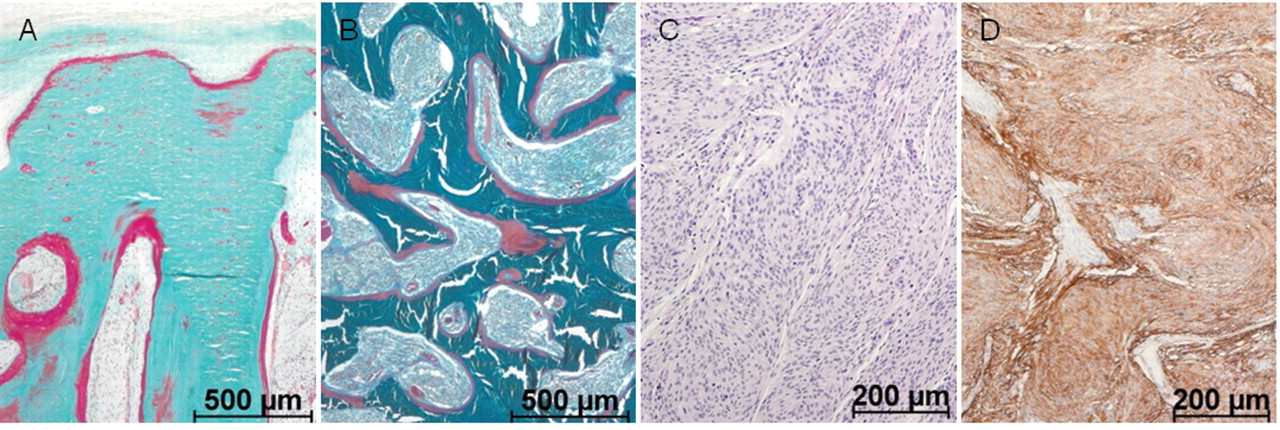
Meningioma en plaque (histopathology). (A) New periosteal bone formation (green trabeculae represent mineralized bone), formed by superficially fused mineralized spiculae with superficial osteoid seams (red parts of trabeculae represent non-mineralized osteoid tissue) next to meningothelial tumor infiltration of the intertrabecular tissue as well as within the Haversian canals. (B) Cancellous bone, irregularly remodeled and densely infiltrated by the tumor. Multifocal broad areas of non-mineralized osteoid on the trabecular surface (A/B: embedded in methylmethacrylate without decalcification, stain: Goldner trichrome, original magnification: ×50). (C) The paraffin-embedded tumor displayed typical meningothelial spindle cells without atypia (hematoxylin-eosin, original magnification: ×100). (D) Each paraffin-embedded tumor showed positive immunohistochemical reactions against the SSR2A antibody (original magnification: ×100).
Meningioma en plaque. Morphological characteristics.
The exact molecular and/or biochemical mechanisms of intralesional hyperosteoidosis in the meningioma en plaque remain to be explored. In the current study, SSR2A immunohistochemical results of the intraosseous infiltrating meningioma en plaque were positive, which has already been reported in both extraosseous meningiomas and in some other neoplasms associated with oncogenic osteomalacia (36-37). This morphological observation has several potential diagnostic and therapeutic implications. Firstly, the usefulness of somatostatin analogue (111In-DTPA-d-Phe1)-octreotide scintigraphy for the visualization of meningiomas (38-39) and meningioma en plaque in particular (40) has been demonstrated. Moreover, octreotide scintigraphy allows differentiation between meningiomas and neurinomas or neurofibromas and other tumors (41-42) as well as the identification of multiple intracranial lesions (38). Furthermore, scintigraphy seems to be valuable in both the identification of invasive tumors and postoperative differentiation between recurrent meningiomas and scar tissue (38). It is also interesting to note that octreotide scintigraphy has been successfully used in diagnosing the soft and bone tissue tumors associated with oncogenic osteomalacia (43-50). However, the therapeutic impact of octreotide on tumors associated with oncogenic osteomalacia remains questionable (37, 48, 51-53).
Several important limitations to the current study are recognized. First, as bone biopsies were only taken from tumor-infiltrated calvarial lesions, it cannot be concluded whether generalized oncogenic osteomalacia was also present. To investigate the possible presence of systemic oncogenic osteomalacia, more complex clinical (renal functions, nutrition), radiographical (bone marrow density) and laboratory tests (calcium, phosphate, vitamin D, parathormone) are necessary. Similarly, data on serum somatostatin was unavailable. None of these parameters could be addressed retrospectively. Moreover, pathological fractures were not reported in the clinical records. To the best of our knowledge, tumor recurrence was not observed at later follow-up. The other essential limitation was undoubtedly the small study cohort. In fact, the vast majority of bony material sent to neuropathological laboratories is traditionally processed after decalcification of the bony surgical specimens. The undecalcified processing methods of mineralized tissues are mostly accessible only in histopathological laboratories specializing in bone pathology. Thus, only five meningotheliomatous meningiomas en plaque diagnosed in both institutions within the last four years with adequately processed tissues were identified.
To summarize, five cases of meningioma en plaque associated with intralesional features similar to oncogenic osteomalacia and new periosteal reactive bone formation are presented and the potential biological and clinical implications possibly linked to the observed expression of SSR2A are discussed.
Footnotes
-
↵* J. Matschke and J. Addo contributed equally to this work. This work is part of the promotion thesis of J. Addo.
-
Disclosure/Conflict of Interest
We declare that we have no conflict of interests (either financial or personal). This work has not been published or presented (oral, print or online) elsewhere in whole or in part.
- Received October 30, 2010.
- Revision received January 4, 2011.
- Accepted January 5, 2011.
- Copyright© 2011 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.