


Abstract
Aim: The human epidermal growth factor receptor HER-2/neu (HER2) gene is a proto-oncogene involved in the signal transduction pathways leading to cell growth and differentiation. The present study focused on the clinical significance of the expression of HER2 in non-small cell lung cancer (NSCLC). Patients and Methods: Consecutive specimens of 159 adenocarcinomas and 77 squamous cell carcinomas, from patients who had been treated by complete resection of NSCLC in our department between 2003 and 2005, were studied. The HER2 expression was evaluated by immunohistochemical staining with score of membranous staining being 0=none, 1=weak, 2=10-30% cells, 3≥30% cells stained. Results: The staining scores in adenocarcinoma were 0 in 121 patients (76.1%), 1 in 16 (10.0%), 2 in 17 (10.7%), and 3 in 5 patients (3.1%). The HER2 expression scores in squamous cell carcinoma were 0 in 74 patients (96.1%), 1 in 1 (1.2%), 2 in 1 (1.2%), and 3 in 1 patient (1.2%). The postoperative 5-year survival rate of patients with adenocarcinoma according to the expression of HER2 scores 0, 1, 2 and 3 was 75.3%, 77.8%, 76.5% and 20.0%, respectively. Patients with adenocarcinoma with score 3 staining had a significantly unfavorable prognosis compared to those with staining scores of 0-2 (p=0.0216). Conclusion: HER2 overexpression (score 3) in adenocaricinoma was a significantl unfavorable prognostic factor. Since the number of NSCLC patients with HER2 overexpression was small, further investigations will be necessary to clarify the efficacy of molecular targeted therapy for this subgroup.
The human epidermal growth factor receptor HER-2/neu (HER2) gene is a proto-oncogene located on the long arm of human chromosome 17 (17q21) (1). HER2 is the second member of the epidermal growth factor receptor family, and plays an important role as a receptor tyrosine kinase (2). It is normally involved in signal transduction pathways, leading to cell growth and differentiation. Increased expression levels of HER2 have been reported in a number of malignant tumor types, and its gene amplification induces protein overexpression at the cell membrane (3, 4). Ligand-independent homodimerization or heterodimerization occurs when HER2 is overexpressed on the cell surface (5). Dimerization then stimulates the auto-phosphorylation of the intracellular tyrosine kinase domain (6). Trastuzumab is a monoclonal antibody that binds to the extracellular domain of the HER2/neu receptor, suggesting that it has a potential role for molecularly targeted cancer therapy in HER2-overexpressing cancer. Recently, Trastuzumab has been applied for the treatment of gastric and breast cancer (7, 8). However, the expression of HER2 in non-small cell lung cancer (NSCLC) has not yet been fully clarified, and its prognostic value is still controversial. The present study focused on the clinical significance of the expression of HER2 in NSCLC.
Patients and Methods
The Institutional Review Board approved this study after an informed consent was obtained from the patients for the use of the specimens and for the analysis. Consecutive specimens of 159 adenocarcinomas and 77 squamous cell carcinomas, from patients who had been treated by complete resection of NSCLC in our department between 2004 and 2007, were studied.
The preoperative assessments included chest roentgenography and computed tomography (CT) of the chest, upper abdomen and brain. Bone scintigraphy was performed to detect bone metastasis. Magnetic resonance imaging of the brain was routinely employed for the assessment of distant metastasis. Bronchoscopy was routinely performed to obtain a pathological diagnosis by transbronchial lung biopsy, and to evaluate endobronchial staging. The patients' records, including their clinical data, preoperative examination results, details of any surgeries, histopathological findings, and the tumor, node, metastasis (TNM) stages of all patients were also reviewed. The histopathological findings were classified according to the World Health Organization criteria, and the UICC TNM staging system (7th edition) was also employed (9, 10).
Postoperative systemic chemotherapy was performed for patients with stage II-III disease if the patients were able to tolerate such treatment after surgery, or unless the patients refused additional chemotherapy. Follow-up information was obtained from all patients through office visits or telephone interviews either with the patient, with a relative, or with their primary physicians. The patients were evaluated every 3 months by chest roentgenography, and chest CT scans and bone scintigraphy were performed every 6 months for the first 2 years after surgery and annually thereafter. The average period of follow-up after surgery was 48 months.
Immunohistochemical staining was conducted using serial sections from the same paraffin-embedded blocks by previously described methods (11). Two-micrometer-thick sections sliced from paraffin-embedded specimens were prepared on glass slides precoated with silane. After removing the paraffin with xylene and washing the slides in a graded series of ethanol, the sections were placed in Tris-buffered saline (TBS) for 10 min. All specimens were stained with hematoxylin–eosin for the histological diagnosis. The sections were briefly immersed in citrate buffer [0.01 mol/l citric acid (pH 6.0)] and were then incubated for 10 min at 121°C in a high-pressure sterilization oven for antigen retrieval. The endogenous peroxidase activity was blocked for 10 min in a blocking solution, then the slides were placed in TBS. The sections were incubated with TBS including a 1% concentration of bovine serum albumin for 10 min to block nonspecific binding of the immuno-reagents. After washing in TBS, the sections were incubated with a mouse anti-HER2 monoclonal primary antibody (NCL-c-erbB-2-316, Novocastra Laboratories, Newcastle, UK), diluted 1:50 in phosphate-buffered saline for 60 min at room temperature. All incubations proceeded overnight at 4°C. Thereafter, immunohistochemical staining was performed by the labeled polymer method (Histofine Simple Stain MAX-PO kit, Nichirei, Tokyo, Japan) according to the manufacturer's instructions. Negative controls were included by adding PBS solution instead of the primary antibody, and positive controls for HER2 were conducted by staining known positive breast cancer samples from our pathology specimen bank. The expression levels of HER2 were considered to be positive when the cell membrane was stained brown.
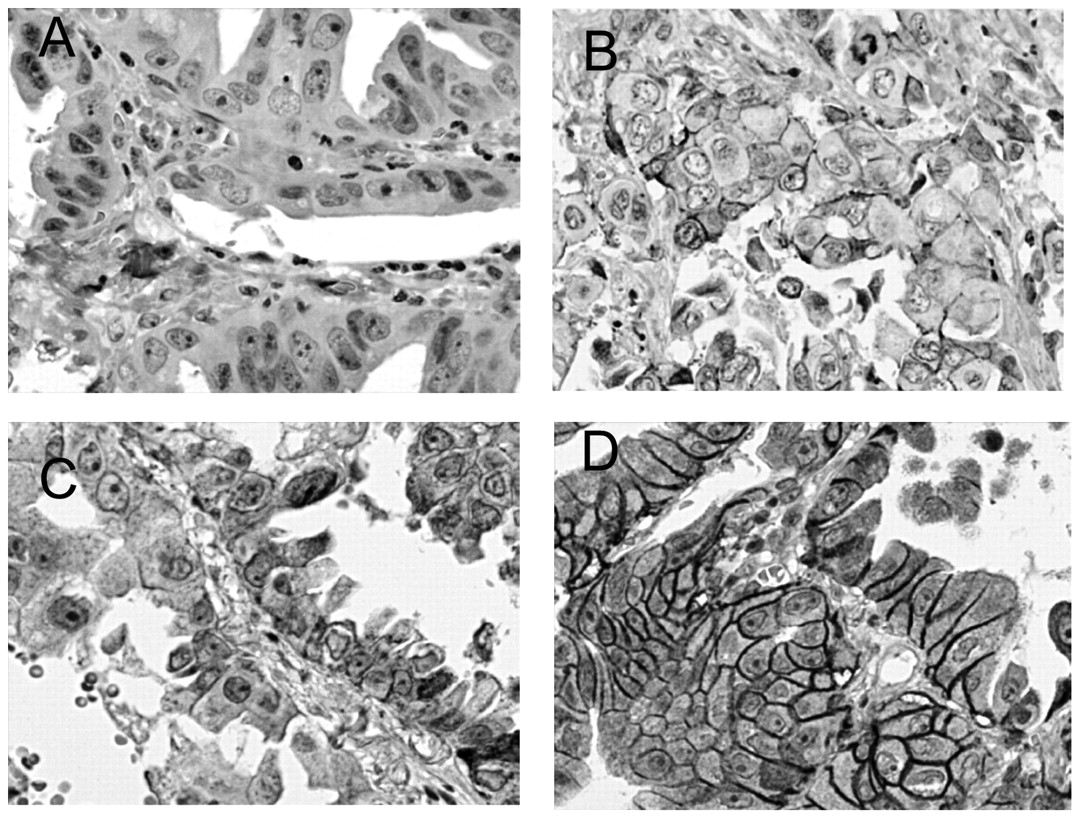
The evaluations of the immunostaining results were performed by two pathologists and scored according to ASCO guidelines (12, 13): samples were considered negative for score 0 (no membrane staining) and score 1+ (faint or barely perceptible incomplete membrane staining); equivocal for score 2+ (10-30% tumor cells with strong complete membrane staining or >10% tumour cells with moderate complete membrane staining) and positive for score 3+ (>30% tumor cells with strong complete membrane staining) (Figure 1).
All specimens were examined and scored by two independent investigators (M.T. and T.H.) without knowledge of the patient data, and their inter-observer concordance was over 90%. When a discrepancy was found between the two investigators, discussions were held until a consensus was reached via their simultaneous examinations using a double-headed microscope.
Statistical significance was evaluated using the chi-square test or Fisher's exact test. The Kaplan-Meier method was used to estimate the probability of survival, and survival differences were analyzed by the log-rank test. Differences were considered to be statistically significant for p-values <0.05. The data were analyzed using the StatView software package (Abacus Concepts, Inc., Berkeley, CA, USA).
Results
The hospital records of 236 consecutive patients who underwent a resection of adenocacinoma (n=159) and squamous cell carcinoma (n=77) were examined. The patients with adenocarcinoma consisted of 67 males and 54 females. Among them, 5 patients (3.1%) had high expression (score 3) of HER2. The other staining scores were 0 in 121 patients (76.1%), 1 in 16 (10.0%), and 2 in 17 (10.7%) patients. Immunostaining for HER2 was not observed in normal lung tissues or in the bronchial epithelia adjacent to the carcinoma tissues, except for mild staining in normal ciliated bronchial epithelium and bronchial mucosal glands. The patients with score 3 staining were all males. There were no significant differences in the T factor, N factor, pathological stage and use of adjuvant chemotherapy according to HER2 expression (Table I). The 5-year survival rate after surgery according to the expression of HER2 (scores 0, 1, 2 and 3) was 75.3%, 77.8%, 76.5% and 20.0%, respectively (Figure 2). The adenocarcinoma patients with a staining score of 3 showed a significantly poorer prognosis than those with staining scores of 0-2 (p=0.022). Four out of five patients with a staining score of 3 died due to recurrence of the NSCLC.
The patients with squamous cell carcinoma included 68 males and 9 females. The HER2 expression was evaluated as staining score of 0 in 74 patients (96.1%), 1 in 1 (1.2%), 2 in 1 (1.2%), and 3 in 1 (1.2%) patients (Table II). All three patients with scores of 1-3 for HER2 staining were males and positive for lymph node metastasis. The patient with score of 1 has remained well for 4 years after surgery without evidence of recurrence. The patient with a staining score of 2 died due to pneumonia 3 months after surgery. The patient with a score of 3 was alive with renal metastasis 4 years after the surgery.
Discussion
Lung cancer is one of the most prevalent types of cancer and is a leading cause of cancer-related mortality worldwide (14). NSCLC accounts for approximately 85% of lung cancer cases. The survival of stage I NSCLC patients after complete resection is reported to be 60-80% (15, 16). Lung cancer patients are often diagnosed with advanced disease due to the aggressiveness of this type of cancer. Furthermore, the outcome of patients with recurrent disease or advanced disease remains dismal (17). Although platinum-based doublet chemotherapy regimens provide longer survival compared to best supportive care, the median overall survival in patients with advanced NSCLC has only been improved to around 10-12 months (18). It is therefore necessary to establish a novel treatment strategy to improve the prognosis of NSCLC patients.

Immunohistochemical staining for HER2. A: Negative staining (score 0), B: Faint or barely perceptible incomplete membrane staining (score 1), C: 10–30% tumor cells with strong complete membrane staining or >10% tumour cells with moderate complete membrane staining (score 2), D: >30% tumor cells with strong complete membrane staining (score 3) (×200).
HER2 gene amplification and protein overexpression were first identified in around 30% of breast carcinoma, and were subsequently similarly demonstrated in various tumor types including gastric cancer (4, 19). However, HER2 overexpression (score 3 or positive during a fluorescence in situ hybridization analysis) was observed in only 2-5% of patients with NSCLC (20). The majority of HER2-positive tumors have an immunohistochemistry score of 2+, and FISH positivity is uncommon in NSCLC (21). Perera et al. found that a high percentage (67%) of human adenosquamous lung carcinomas had increased membranous HER2 staining, which was significantly higher than in adenocarcinomas, squamous cell carcinomas, or large cell carcinomas of the lung (22).
Recent studies have indicated that HER2 has prognostic implications in gastric and breast cancer, where HER2 overexpression is associated with a poor survival (23, 24). In NSCLC, several studies have previously investigated the prognostic significance of HER2 overexpression. Nakamura et al. showed a significant, unfavorable prognostic effect of HER-2 overexpression in NSCLC in a meta-analysis (25). However, their study cautioned readers about the interpretation of the results because several studies that found no significant difference were excluded because of their eligibility criteria. Conflicting results have been reported concerning HER2 overexpression and the survival of NSCLC patients. Pelosi et al. reported that there was a lack of prognostic implication for HER2 abnormalities in surgically resected stage I NSCLC cases (26). In addition, Tomizawa et al. showed that gene mutations of HER2 were not associated with the prognosis of NSCLC patients who underwent surgical resection (27).
HER2 expression in adenocarcinoma of the lung.
HER2 expression in squamous cell carcinoma of the lung

The overall survival curves of patients according to the expression of HER2. Adenocarcinoma patients with staining scores of 3 had a significantly poorer prognosis than those with scores of 0-2 (p=0.022).
The determination of HER2 status serves as a critical predictive test for treatment with the monoclonal antibody, trastuzumab (Herceptin, Genentech/Roche, Basel, Switzerland), and the tyrosine kinase inhibitor, lapatinib (Tykerb, GlaxoSmithKline, Brentford, UK). Trastuzumab, in combination with standard chemotherapy, displays efficacy against HER2 gene-amplified/protein-overexpressing primary and metastatic breast cancer, and recent studies have shown that this also holds ground for gastric cancer (7, 28). Molecular-targeted therapy against HER2 therefore has the potential to be used to treat patients with HER2-positive NSCLC. A randomized phase II trial of gemcitabine–cisplatin with or without trastuzumab demonstrated that NSCLC patients with HER2/neu overexpression (3+) detected in an immunohistochemical analysis had a better survival when treated with trastuzumab-based therapy than the overall population of NSCLC patients. (29).
Recently, a number of cancer types have been reported to be addicted to specific tyrosine kinases. The well-known oncogene addiction in NSCLC includes HER2 amplification and epidermal growth factor receptor (EGFR) mutation (30). NSCLC characterized by oncogene addiction to the EGFR pathway displays dramatic responses to reversible tyrosine kinase inhibitors. A HER2-overexpressing NSCLC cell line was also responsive to growth inhibition by lapatinib, which is a dual tyrosine kinase inhibitor of EGFR and human HER2 (31). These findings are consistent with the clinical results of therapy with lapatinib in patients with HER2-overexpressing breast cancer. HER2 drives the rapid development of adenosquamous lung tumors in mice that are sensitive to an irreversible EGFR and HER2 kinase inhibitor (BIBW2992) and rapamycin combination therapy (22). The most promising HER2-targeted strategy will likely prove to be combinatorial approaches using an EGFR tyrosine kinase inhibitor together with HER2 dimerization inhibitors (32).
In the present study, the overexpression (score 3) of HER2 was identified in 3.1% and 1.2% of patients with adenocarcinoma and squamous cell cancer of the lung, respectively. We found an unfavorable prognosis for the patients with adenocaricinoma who had HER2 overexpression (staining score 3), whereas no clinically significant differences were observed for patients with a HER2 staining score of 1 or 2. However, since the number of patients with a staining score of 3 was small, further investigations are necessary to clarify the efficacy of molecular targeted therapy for this subgroup of patients.
Acknowledgements
This study was supported in part by a Grant-in-Aid from the Ministry of Education, Culture, Sports, Science, and Technology, Japan. The Authors thank Ms. Yukiko Koyanagi for her excellent technical assistance.
- Received October 18, 2011.
- Revision received November 12, 2011.
- Accepted November 15, 2011.
- Copyright© 2011 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}