


Abstract
Aim: More effective regimens are urgently needed for treatment of esophageal carcinoma; therefore, we conducted a phase I trial of a combination of docetaxel, nedaplatin, and S-1 (DGS) to determine the optimal dose in patients with advanced esophageal carcinoma. Patients and Methods: We studied 14 patients with previously untreated advanced cervical esophageal carcinoma with T3-4 tumors and/or M1 staging and esophageal carcinoma with cervical lymph node metastasis. The patients received an infusion of docetaxel at different dose levels (levels 1, 2, 3, 4: 25, 30, 35, 40 mg/m2, respectively) and an infusion of nedaplatin (40 mg/m2) on day 8 plus oral administration of S1 (80 mg/m2/day) for two consecutive weeks at two-week intervals. Results: Dose-limiting toxicities (DLTs) included febrile neutropenia and leukopenia. DLTs occurred in 2 out of 5 patients at level 4. The response rate was 78.6 (11/14)%, including a complete response rate of 35.7(5/14)%. Conclusion: The DGS regimen reported here was well tolerated and toxicities were manageable. The maximum tolerated dose was level 4, and the recommended dose was determined to be docetaxel at 35 mg/m2 with nedaplatin at 40 mg/m2 plus S1 at 80 mg/m2. We found that our regimen, administered on an outpatient basis, showed high activity and tolerance. A phase II study has been started.
Locally advanced or widespread metastatic esophageal carcinoma is difficult to treat and is often thought to progress rapidly. Quick deterioration of respiratory and nutritional states makes outpatient care impossible and leads to an extremely poor prognosis. It is necessary to establish effective and safe outpatient chemotherapy that provides survival benefits and improvements in quality of life compared with best supportive care.
Over the past several decades, patients with unresectable or inoperable esophageal disease have usually been treated with various chemotherapy strategies, and prognosis is extremely poor, with a mean survival time of less than 8.1 months with current chemotherapies used singly or in combination with 5-fluorouracil (5-FU), vindesine, mitomycin, docetaxel, paclitaxel, cisplatin, irinotecan, vinorelbine, or capecitabine (1-3).
Standard chemotherapy is fluorouracil and cisplatin combination therapy (FP), for which the median survival time is reported to be 9.2 months for responders and 5.3 months for nonresponders (4, 5). The response rates reported with FP range from 35 to 40%, whereas two-year survival rates of patients with locally advanced esophageal cancer range from 8 to 55% (mean 27%) (6-8).
To improve both local and distant tumor control in patients with esophageal carcinoma, new therapeutic combinations must be developed. Recently, favorable antitumor effects of combination therapy with fluorouracil and taxanes were reported. Many studies have shown that taxanes have significant activity in patients with locally advanced and metastatic esophageal carcinomas (9). For advanced esophageal carcinoma, a combination of docetaxel and 5-FU with concurrent radiotherapy had good efficacy (10).
Docetaxel, cisplatin, and 5-FU (DCF) have exhibited different mechanisms of activity in upper gastrointestinal malignancies. In a randomized phase III study from the V325 study group, advanced gastric or gastroesophageal junction cancer patients receiving DCF not only had statistically significantly improved overall survival and time to tumor progression, but they also had better preserved quality of life compared with patients receiving FP therapy (11, 12).
We previously reported a phase I study of DCF for advanced esophageal squamous cell carcinoma. To minimize toxicity and maximize dose intensity, we investigated a biweekly regimen. This regimen was tolerable and highly active. The response rate was 88.9%, including a complete response rate of 33.3% (13). However, hospitalization is necessary with this regimen, and cisplatin requires hydration and is thus not easily used if renal dysfunction is present.
The combination of docetaxel and S1 is highly active and well tolerated for advanced or recurrent gastric cancer (14), and synergy of this combination has been reported in vitro (15). S1 (TS1®; Taiho Pharmaceutical Co. Ltd., Tokyo, Japan) was developed by the biochemical modulation of tegafur, a 5-FU prodrug; gimeracil, a dihydropyrimidine dehydrogenase inhibitor; and oteracil, which inhibits pyrimidine phosphoribosyl transferase specifically in the gastrointestinal tract and thereby reduces the phosphorylation of 5-FU in the intestine. S1 is a well-designed oral formulation, with the dual actions of reinforcing antitumor activity and reducing gastrointestinal toxicity (16).
In a late phase II study of nedaplatin (cis-diamminegly-colatoplatinum) in patients with advanced head and neck cancer, the response rate was 37.5%, higher than that reported for cisplatin, and carboplatin (17-19). Nedaplatin is a less nephrotoxic analogue of cisplatin. Drug secretion and re-absorption in the convoluted tubules are not seen, and it is less toxic to the gastrointestinal tract mucosa than is cisplatin, which is a second-generation platinum derivative that has demonstrated potent antitumor activity against lung, testicular, esophageal, gynecological, and head and neck cancers. Platinum primarily acts as an alkylating agent, whereas docetaxel stabilizes microtubules and inhibits mitosis; therefore, a combination of docetaxel and platinum should be expected to result in additive antitumor effects and non-overlapping toxicity profiles.
A phase II study of induction chemotherapy with docetaxel and nedaplatin for oral squamous cell carcinoma showed a good response rate of 33.3% (20). Hydration is not required before or after nedaplatin administration, thus allowing use of the drug on an outpatient basis.
We therefore conducted a phase I clinical trial of the triplet combination of docetaxel, nedaplatin, and S-1 (DGS) in patients with advanced cervical esophageal carcinoma with T3-4 tumors and/or M1 staging and esophageal carcinoma with cervical lymph node metastasis. The goal of this trial was to determine the recommended dose (RD) for use in phase II trials on the basis of the maximum tolerated dose (MTD) and dose-limiting toxicity (DLT). Secondary objectives were treatment-related toxicity and efficacy.
Patients and Methods
Patient eligibility criteria. Patients eligible for the present study had to be ≥20 years of age at the time of registration and have histologically or cytologically confirmed squamous cell carcinoma (SCC) or either T3/T4 or recurrent adenocarcinoma. An Eastern Cooperative Oncology Group (ECOG) performance status of 0, 1, or 2 was required, as were a life expectancy of >12 weeks and adequate liver, bone marrow, renal, and cardiovascular function as evidenced by the following measures: serum bilirubin ≤1.5 mg/dl, neutrophil count ≥1,500/mm3, serum aspartate aminotransferase (AST) and alanine aminotransferase (ALT) levels of less than or equal to twice the upper limit of normal range, platelet count ≥100,000/mm3, hemoglobin ≥8.0 g/dl, and serum creatinine ≤1.5 mg/dl or creatinine clearance rate >60 ml/min. In addition, the latest chemotherapy treatment must have been at least 4 weeks before trial enrollment. Major exclusion criteria included the following: previous treatment with taxane therapy for recurrent disease or irradiation to major bone areas; serious concomitant malignancy; active infectious disease with fever; severe drug allergy; symptomatic peripheral neuropathy; uncontrolled diabetes mellitus, hypertension, angina pectoris, arrhythmia or congestive heart failure; and interstitial pneumonia or lung fibrosis. Prior to study entry, all patients were required to sign an informed consent form approved by the Ethical Committee of Gifu University Hospital. Ultimately, 14 patients were enrolled in the study, and all fully underwent DGS therapy.
Study design. The primary objectives of this phase I dose-escalation study were to determine the MTD and toxicity of escalating doses of docetaxel combined with a fixed dose of nedaplatin and S-1 in patients with advanced esophageal carcinoma. The secondary objective of the study was to obtain preliminary data regarding clinical response. This study of DGS was conducted at the Department of Surgical Oncology, Gifu University School of Medicine.
At least three patients were entered at each docetaxel dose level. No dose escalation for individual patients or within a dose level was permitted. All three patients at a given dose level had to complete the first two cycles of treatment without DLT before further patients were enrolled in the next dose level. If DLT did not occur, the next dose level was explored. Doses were increased in sequential groups of three patients until the MTD was established or the highest intended dose levels were reached. If any of the three patients experienced DLT, an additional three patients were treated at the same dose level. If more than three out of the six patients at a given dose level experienced DLT, that dose level was defined as the MTD. The dose level one step below the MTD was set as the RD for further evaluation in a phase II study.
Treatment plan. The patients received an intravenous infusion of docetaxel at different dose levels (level 1, 25 mg/m2; level 2, 30 mg/m2; level 3, 35 mg/m2; and level 4, 40 mg/m2) and an intravenous infusion of nedaplatin (40 mg/m2) followed by 500 ml hydration on day 8 plus oral administration of S1 (80 mg/m2/day) twice daily (within 30 minutes after the morning and evening meals) for two consecutive weeks at two-week intervals (one cycle).
On day 8, patients received docetaxel diluted in 250 ml of normal saline at the assigned dose. It was infused intravenously over 2 hours. Then nedaplatin was prepared in normal saline at a dose of 40 mg/m2 and administered intravenously over 2 hours followed by 500 ml hydration. If the patient had upper digestive tract obstruction, S-1 was administered through a 6-8 Fr nasogastric tube inserted in the stomach. The dose-escalation scheme is described in Table I. The initial dose of docetaxel was 25 mg/m2 (dose level 1), and this was increased up to a maximum of 40 mg/m2 in 5-mg/m2 steps.
Dose-escalation scheme.
Supportive therapy for treatment and prophylaxis for expected side-effects were administered. All patients were premedicated with intravenous administration of 2 mg of granisetron. Hypersensitivity reactions were treated with prophylactic use of intravenous dexamethasone at 8 mg, which was infused 1 hour prior to the administration of docetaxel. Further dexamethasone was prescribed at a dose of 8 mg orally for 2 days after administration of docetaxel to reduce the risk of hypersensitivity reaction and fluid retention. Diuretics were added at the discretion of the treating physician. Additional antiemetics were recommended on subsequent days as needed.
Granulocyte colony-stimulating factor (G-CSF) was administered once a day if the neutrophil count was below 500/μl or if febrile neutropenia (fever ≥38°C and neutrophil count of <1,000/μl) were observed. G-CSF was stopped if the neutrophil count was >5,000/μl. To avoid severe mucositis, L-glutamine at 8 g was administered orally to all patients.
Patient monitoring and response criteria. Complete staging procedures for documentation of disease extent, which included assessment of ECOG performance status, medical history, and physical examination, were performed on all patients. Laboratory evaluations were obtained within one week before initiation of treatment and at the start of each treatment cycle and included the following: complete blood cell count; serum electrolytes; urea; creatinine and 24-hour creatinine clearance; bilirubin; alkaline phosphatase and transaminases; carcinoembryonic antigen (CEA), squamous cell carcinoma-related antigen (SCC), carbohydrate antigen 19-9 (CA19-9) and cytokeratin 19 fragment (CYFRA) measurements, and electrocardiogram. For baseline reference, either computed tomography (CT) or magnetic resonance imaging (MRI) and positron-emission tomography CT were performed within two weeks prior to study entry. During chemotherapy, a complete blood count was measured in all patients every week, and levels of electrolytes, serum creatinine, transaminases, alkaline phosphatase and bilirubin, and plasma urea were measured every two weeks. We used the Common Terminology Criteria for Adverse Events (v3.0) to grade the medical history, which included physical examination and toxicity assessment, every two weeks during the study. Tumor measurements were made from radiographic films or scans taken to document treatment response during therapy and were repeated at every second cycle of treatment or sooner if the patient appeared to show disease progression. We assessed tumor response according to the Response Evaluation Criteria in Solid Tumors (RECIST) guidelines (21). A barium meal study, endoscopy, ultrasonography, and CT or MRI was used to evaluate the response status of measurable lesions.
We defined complete response as complete disappearance of all clinically detectable malignant disease and partial response as a ≥30% decrease in the sum of the perpendicular diameters of all measurable lesions present for at least 4 weeks. We defined progressive disease as either a ≥20% increase in the sum of the products of measurable lesions over the smallest sum observed or as the appearance of new lesions. Stable disease did not qualify as complete response, partial response, or progressive disease.
Characteristics of patients.
Definition of DLT and criteria for dose modifications. The Common Terminology Criteria for Adverse Events (v3.0) was used to evaluate and score toxicity. We defined DLT to include the following: febrile grade 3 neutropenia, grade 4 neutropenia lasting >7 days, grade 3 leucopenia, grade 4 thrombocytopenia or grade 3 thrombocytopenia with bleeding tendency, or any grade 3 or 4 non-hematological toxicity other than nausea/vomiting, anorexia, diarrhea, alopecia, and general fatigue. Occurrence of hematological toxicity of ≥grade 3 resulted in delay of therapy until the platelet count was at least 100,000/mm3 and absolute neutrophils were ≥2,000/μl. Occurrence of gastrointestinal toxicity of ≥grade 3 resulted in delay of chemotherapy until the optimum dose could be tolerated. Treatment was repeated every 4 weeks or as soon as the patient had recovered from the toxicity of the previous chemotherapy. However, the patient was removed from the study if toxicity persisted for more than two weeks following the time of planned treatment. Delay in administration of the second cycle of therapy of longer than two weeks was also considered a DLT. Dose modifications for the next dose were based on the most severe toxicity observed since the previous treatment course. If DLT occurred, treatment was interrupted until toxicity resolved to ≤grade 1.
Dose-escalation scheme in relation to dose-limiting toxicity and response.
Results
Patient characteristics. Between November, 2008, and January, 2010, 14 patients were enrolled in the present study. Demographic and clinical characteristics of the study population are summarized in Table II. Four docetaxel dose levels were evaluated. A total of 72 courses of chemotherapy were administered, with the median number of courses administered per patient being 5.1 (range, 2-10). All patients had locally advanced esophageal carcinoma or metastatic lesions. Median patient age was 65.9 years (range, 40-81 years). All patients had an ECOG performance status of 0-1. Histology showed well-differentiated carcinoma in 21.4% of the patients and poorly differentiated carcinoma in 42.9%. Only two patients were hospitalized and administered S-1 by nasogastric tube until finishing their second courses. After the second course, S-1 was administered orally to these two patients in the outpatient setting. The other 12 patients were treated solely as outpatients.
Toxicity and dose-finding study. Data on the dose-escalation scheme, DLT, and response are summarized in Table III. Only ≥grade 2 toxicity data were collected and reported, and especially for neutropenia and leucopenia, only ≥grade 3 toxicity data were reported. Patient characteristics were well balanced across all dose levels. No treatment-related deaths were observed.
The level 1 dose (docetaxel 25 mg/m2) was initially administered to three patients. No patient had grade 3-4 neutropenia lasting five days with fever. Of the three patients treated at dose level 1, all had grade 2 anorexia, one had grade 2 fatigue, and one had grade 2 nausea. Twenty-four courses of chemotherapy were evaluated, and two responders were observed.
Three patients were initially enrolled at dose level 2 (docetaxel 30 mg/m2). One patient had grade 2 anemia. One patient experienced grade 2 nausea, three experienced grade 2 anorexia, and one patient experienced grade 2 hypersensitivity reaction. Fifteen courses of chemotherapy were administered at dose level 2. All three patients were responders.
At dose level 3 (docetaxel 35 mg/m2), no patients developed grade 3/4 hematologic toxicity. One patient experienced grade 2 anemia, and one patient had grade 2 thrombocytopenia. Two patients experienced grade 2 anorexia, one experienced grade 1 nausea, one had grade 1 mucositis, and one had grade 1 pericardial effusion. Sixteen courses of chemotherapy were evaluated, and two responders were observed.
At dose level 4 (docetaxel 40 mg/m2), one out of two patients developed grade 3 toxicity characterized by febrile neutropenia lasting five days with fever, so three patients were added to the cohort at this dose level. Of the five patients treated at this dose level, two had grade 3 leucopenia, two had grade 3 febrile neutropenia lasting five days with fever, one experienced grade 2 nausea, one experienced grade 2 anorexia, and one had grade 2 mucositis. The febrile neutropenia of the two patients was resolved within five days by G-CSF support. Seventeen courses of chemotherapy were evaluated. Among the five patients entered at this dose level, four responders were observed. This dose (docetaxel 40 mg/m2) was considered the MTD; therefore, the dose of docetaxel for further phase II studies was determined to be 35 mg/m2.
The frequency of treatment-related toxicities is summarized in Table IV. Grade 3 leucopenia occurred in 2 out of 14 patients, and grade 3 febrile neutropenia also occurred in 2 out of 14 patients (14.3%). Alopecia was the most frequent non-hematologic toxicity with an incidence of 13/14 of patients, followed by anorexia (9/14) and nausea (4/14). Edema (3/14) and hypersensitivity reaction (1/14), which are known toxicities attributed to docetaxel, were observed, but these side-effects were manageable and reversible. Grade 1/2 mucositis occurred in 2 out of 14 patients (14.3%). The prophylactic administration of L-glutamine may have helped to prevent mucositis. Four out of 72 courses of chemotherapy (5.6%) were delayed for one week due to myelosuppression.
Frequency of treatment-related toxicity (CTCAE Ver.3 common toxicity criteria).
Tumor response. Although the endpoint of this study was not response to therapy, patients who had completed at least two cycles of chemotherapy were evaluated for radiographical response. Five patients showed complete response: three patients received two cycles for a locally advanced esophageal cancer and underwent complete resection (histological grade 2 in one patient and grade 3 in two patients), and two patients received 6-10 cycles for metastatic esophageal cancer (lung and bone, one patient; liver, one patient). Of the six patients with partial response, three stopped therapy after receiving two cycles and underwent surgical curative resection. Three patients with partial response and two patients with stable disease for metastatic esophageal cancer maintained disease stability over 4-7 treatment cycles. One patient had documented stable disease after two cycles for locally advanced esophageal carcinoma and underwent complete resection (histological grade 1).
The response rate was 78.6%, with five patients achieving a complete response and six patients a partial response. Disease stability was observed in the remaining three patients, and no disease progression was observed. No patient discontinued study therapy due to toxicity. Responses were observed at all dose levels, indicating a wide margin of activity for this regimen.
Here, we present a case of complete response to this regimen. The patient was a 72-year-old man who underwent curative resection for advanced esophageal carcinoma (T4N3M0; stage IVa) after receiving the level 2 regimen. Endoscopy revealed an invasive, ulcerative-type cervical esophageal tumor (Figure 1). Biopsy confirmed the diagnosis of SCC. Esophagography showed a circumferential stricture (longest diameter, 55.5 mm) (Figure 2). Invasion of the bronchus by the tumor was suspected on CT (Figure 3). Ultrasonography of the neck showed a round supraclavicular lymph node 12 mm in diameter, which was considered to be a metastatic lesion. Two courses of DGS chemotherapy were undertaken in an attempt to down-stage the tumor. Grade 2 diarrhea was observed. After resolution of toxicity, a three-hole esophagectomy with cervical and mediastinal lymph adenectomy was performed. Following resection, the esophageal cancer was determined to be T0N0M0, stage 0. Histopathological examination of the resected specimen showed an excellent response to the preoperative chemotherapy (Figure 4). The supraclavicular lymph nodes showed fibrosis, strongly suggesting that lymph node metastases had also responded to chemotherapy.
Discussion
Survival time in patients with advanced esophageal cancer is unsatisfactory, and locoregional recurrence and wide metastatic spread remain common in spite of the development of operative procedures and improvement in staging modalities, surgical techniques, and perioperative management (22). Although morbidity and mortality after surgical treatment for advanced esophageal cancer have been reduced and the rate of complete resection has increased, 5-year survival after curative surgery is still only 20-36% (23). There is much evidence that effective chemotherapy for treatment of distant metastasis of esophageal cancer does not exist, and it necessary to establish chemotherapy that considers toxicity in those patients in whom global body function deteriorates during therapy. Therapy is needed that can be delivered as much as possible via the outpatient setting to maintain high quality of life and that can be achieved without the necessity of a large amount of fluid infusion or continuous intravenous administration, both of which require hospitalization.

Endoscopic findings showing an invasive, ulcerative-type cervical esophageal tumor before treatment (A); After chemotherapy (B).

Esophagographic findings showing circumferential stricture (longest diameter, 55.5 mm) before treatment (A) and after chemotherapy (B).
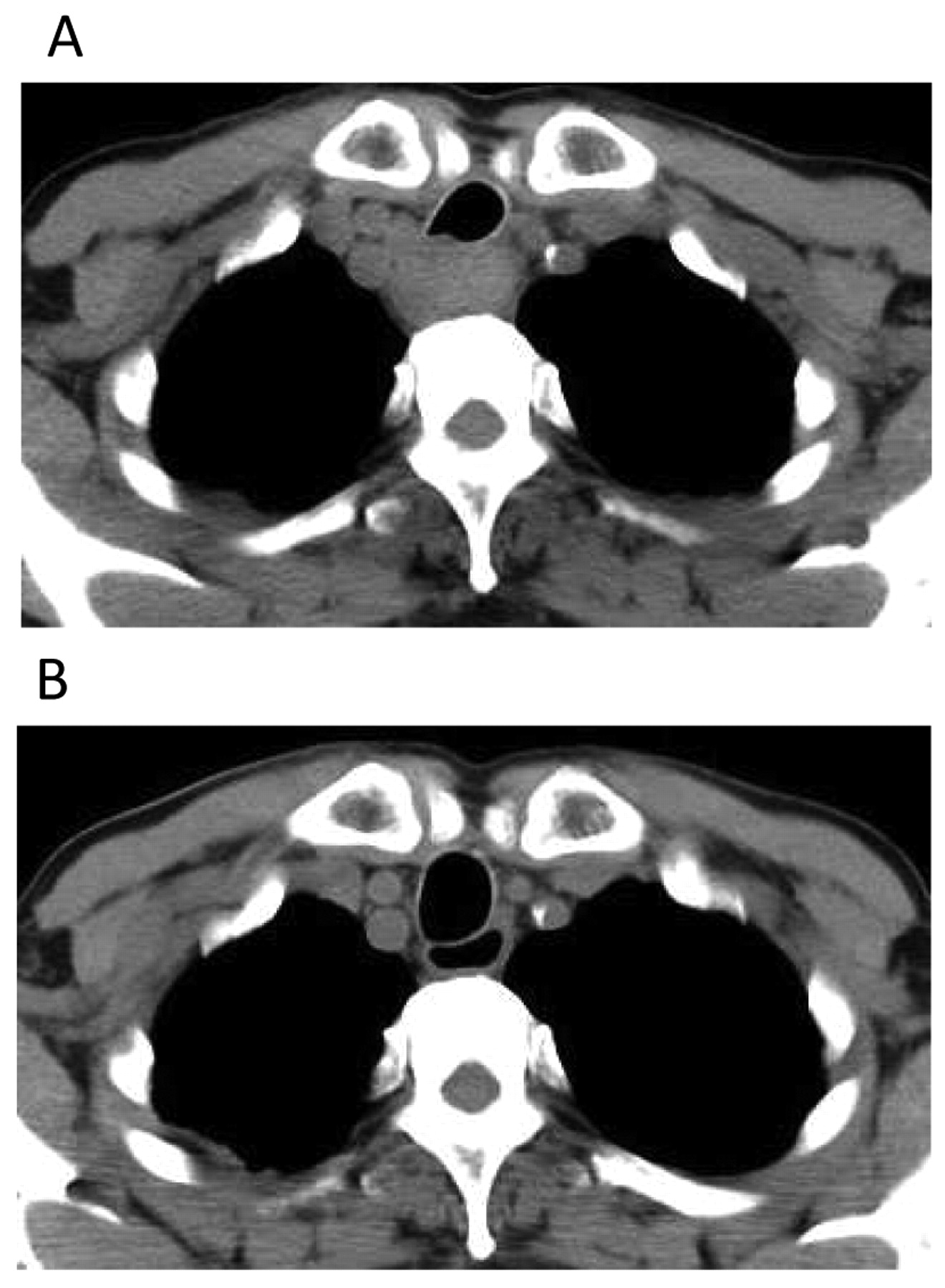
A: Invasion of the bronchus by tumor was suspected on computed tomography (CT) before treatment. B: After chemotherapy.

Histophathological examination of the resected specimen showed an excellent response to the pre-operative chemotherapy.
Thus, the present study was designed to establish a safe and tolerable dose of docetaxel when administered in combination with fixed doses of nedaplatin and S-1. Docetaxel (Taxotere; Sanofi-Aventis, Paris, France) is a semi-synthetic taxoid derived from the European yew, Taxus baccata. The taxanes enhance polymerization of tubulin into stable microtubule formation and inhibit their tubulin depolymerization by blocking the cell cycle in metaphase, anaphase and interphase (24). The synergistic effects of nedaplatin and fluorouracil have been reported in vivo (25), and S-1 is also expected to enhance the antitumor effect of nedaplatin.
The intervals at which these three medicines can be administered has been a problem. Cisplatin showed the best activity when given 8 days after the start of daily uracil-tegafur-cisplatin administration (26). Therefore, Koizumi et al. reported that they administered cisplain on day 8 of a 21-day consecutive S-1 administration in patients with gastric cancer (27). Docetaxel offers favorable outcomes, although it has adverse hematological toxicity. Neutropenia occurs approximately 8-10 days after administration but recovers rapidly (28, 29).
On the basis of these reports and to minimize toxicity and maximize dose intensity, we elected to investigate a regimen of an infusion of docetaxel and fixed dose of nedaplatin (40 mg/m2) on day 8 plus oral administration of a fixed dose of S1 (80 mg/m2/day) for two consecutive weeks at two-week intervals. In the present study, 72 courses of chemotherapy were administered in total to the 14 patients, and responses were observed at all dose levels. No treatment-related deaths were observed. Toxicity of docetaxel was encountered at all dose levels, indicating that the pharmacokinetics of this drug may vary in different individuals.
The median white blood cell and platelet count nadirs occurred on day 18 (range 9 to 20 days), with a median hematological recovery observed by day 24. Neutropenic fever requiring hospitalization was observed in two patients. One patient had grade 2 anemia that did not require blood transfusion, and no thrombocytopenia ≥grade 3 was seen.
The incidence of docetaxel-specific toxicities, such as acute hypersensitivity reactions and neurotoxicity, was relatively low and did not appear to be a major clinical problem, so a reduction in dose was generally not required. Fluid retention manifesting as peripheral edema, pleural effusion, or ascites was cumulative in incidence and severity. Three patients had grade 2 edema that required diuretics.
Patients receiving more than 50 mg/m2 of cisplatin may suffer nausea and vomiting (30). Few patients experience these side-effects with nedaplatin, and they can be well controlled by administration of granisetron and dexamethasone. Grade 1/2 alopecia was observed in 13/14 patients in the present study. Of note, no patient in our study experienced grade 3 or 4 mucositis, likely due to the great care paid to daily oral supplementation with L-glutamine, which contributed to the low toxicity profile of this regimen.
Finally, all seven patients with locally advanced esophageal carcinoma underwent radical surgical resection, no postoperative mortality. Pathologically confirmed complete response was documented in two patients. Toxicities associated with this regimen did not interfere with planned radical surgery.
Locoregional disease control was achieved in 12/14 and distant disease control was achieved in 10/14 of the patients in the present study. The results emerging from this phase I study are particularly encouraging. We want to strongly emphasize that we were able to administer DGS combination therapy in the outpatient setting to all but the two patients with digestive obstruction. Eventually, however, these two patients were also able to take all drugs orally, and we were able to administer the third course of therapy to these patients in an outpatient setting.
In the present study, 11 patients were diagnosed as having SCC, whereas most esophageal carcinomas in Western populations are diagnosed as adenocarcinoma (31). Responses of the three patients diagnosed as having esophageal adenocarcinoma in this study were one complete, one partial, and one stable disease. This DGS regimen appeared to be effective for adenocarcinoma.
In conclusion, the recommended DGS combination dose in the present study was determined to be docetaxel at 35 mg/m2 with nedaplatin at 40 mg/m2 on day 8 plus oral administration of S1 (80 mg/m2/day) for two consecutive weeks at two-week intervals. Our regimen showed high activation and tolerance. It not only could be offered as a candidate component of new standard regimens for treating advanced esophageal carcinoma but may also be acceptable as a second-line regimen, even in cases of deteriorated renal function induced by several chemotherapies. Furthermore, the merit of this regimen to the patients and their families is that it can be administered in an outpatient setting. A phase II study has already begun. Further clinical trials of this combination therapy should be pursued in the treatment of advanced esophageal carcinoma.
- Received September 4, 2011.
- Revision received October 20, 2011.
- Accepted October 25, 2011.
- Copyright© 2011 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Radiomics Features Using Dual-energy CT for Lymph Nodes After Preoperative Chemotherapy for Esophageal Cancer
- Comparative clinical studies of primary chemoradiotherapy versus S-1 and nedaplatin chemotherapy against stage IVb oesophageal squamous cell carcinoma: a multicentre open-label randomised controlled trial