


Abstract
Trans-arterial chemoembolization (TACE) is a promising locoregional therapy for the treatment of primary hepatic tumors and liver metastases. The aim of the study was to define the activity and outcome of using DC Bead, drug-eluting bead, a spherical embolic device capable of being loaded with irinotecan. Patients and Methods: We conducted a double institutional, single arm, phase II clinical study to evaluate TACE adopting this device in 82 patients presenting with metastatic colorectal carcinoma to the liver after failing chemotherapy. The primary endpoints were tumor shrinkage, safety, feasibility, compliance, and overall survival. RECIST criteria were used to assess responses. Quality of life (QoL) was addressed using Edmonton SAS improvement scale. Results: Out of 103 patients considered, 82 were enrolled and underwent a total of 185 treatments of TACE. The median number of TACE was 2.2 (1-4). A post-embolization syndrome was frequently observed. Adverse observed effects were: right upper quadrant pain (40%), fever (80%), nausea (27%) and increased transaminases (70%). The median follow-up was 29 months. Within one month after treatment, each patient received a computed tomograpic scan. It showed reduction of metastatic contrast enhancement in all patients. Responses were 78% at 3 months. After the first treatment, 75 out 82 patients declared an improvement of their well being lasting more than 18 weeks. The median duration of response was 6 (range 3-10) months; the median follow up was 29 (range 7-48) months. The median survival was 25 (range 6-34) months, with progression free survival at 8 (range 4-16) months. Conclusion: We suggest that TACE adopting DC Bead®, drug-eluting bead loaded with irinotecan could be proposed as palliative therapy for unresectable and chemotherapy resistant liver metastases from CRC.
Metastatic colorectal cancer (CRC) is one of the leading causes of cancer-related death worldwide. In the majority of cases, the systemic spread of this disease occurs in the liver (1, 2). Of more than 150,000 new cases of colorectal cancer reported in the United States each year, as many as 25% will have initial liver metastases and another 50% will develop liver recurrence within the next 5 years. The liver will remain the only site of metastatic disease until death in most patients. Surgical resection is the standard treatment in patients with resectable liver disease but results are disappointing (3, 4). When surgery is not feasible, chemotherapy (5-10), radiofrequency ablation (11, 12), and (TACE) are possible alternatives for achievin local control (13-22).
TACE is the administration of embolic particles mixed with chemotherapeutic drugs. It produces a shutdown of blood flow and the simultaneous release of high doses of the drug increasing the drug concentration and tumor exposure to the drug compared with standard intra-arterial infusion (2, 13, 22-25).
TACE is currently approved for the treatment of hepatocellular carcinoma but it has been investigated liver metastases (LM) from neuroendocrine tumors (15) and CRC (13, 14-22).
Different embolic formulations are available. They have different diameters and can be combined with various drugs: mitomycin-C, melphalan, cisplatin, epirubicin and irinotecan. DC Bead, drug-eluting bead, a spherical embolic device capable of loading with irinotecan, has been developed showing interesting properties (26, 27).
Clinical studies consistently reported high response rates to TACE in the treatment of LM from CRC but randomized studies are lacking and the impact of this procedure on survival is unknown (13, 14, 16-21, 28). On the other hand, this technique was shown to be associated with a variety of side-effects, and the most common of which is the postembolization syndrome. This consists of pain in the right upper quadrant (RUQP), nausea, vomiting, fever, and elevation of liver enzymes and occurs in almost every patient (29, 30). Less common complications are liver abscess, tumor rupture, acute liver failure, infarction, acute pancreatitis and acute renal failure (31-35).
From December 2005 to September 2011, we carried out this study with TACE using DC Bead, drug-eluting bead, loaded with irinotecan (DEBIRI). Our scope was to assess the safety, feasibility, tolerability, response rate and duration of response in the treatment of LM from CRC. We also studied the acute toxic effects, survival rate and quality of life (QoL) of treated patients adopting the Edmonton Symptom Assessment System (36).
Patients and Methods
A prospective double-institutional single arm treatment study, approved by the Institutional Review Board was evaluated from December 2005 to September 2011, in which 82 patients presenting with LM from CRC were treated with DEBIRI. The study was conducted in compliance with the protocol and the principles laid down in the Declaration of Helsinki, in accordance with the ICH Harmonized Tripartite Guideline for Good Clinical Practice. Informed consent was obtained from the participants prior to evaluation, screening and treatment. The study was initiated to apply the criteria for appraising the quality of a study. We present a well-reported patient population with high quality data and quality control and with good clinically significant follow-up without loss of patients.
Patient characteristics. A total of 103 patients were considered for the study and 82 of them were finally selected. There were 29 women and 53 men, age 61.8 years (range 46-82). The diagnosis of LM, before being histologically proven, was detailed and verified with multi slice CT scan imaging or magnetic resonance imaging (MRI) of the liver. Results indicated a median liver substitution of 33% (range 25-50) at pre-interventional imaging. All patients were in good physical condition with an ECOG performance status of 0 in 40 patients, 1 in 30 and 2 in 12.
All patients had previously undergone at least two lines of systemic chemotherapy and had either developed progressive disease or had not responded to chemotherapy. The chemotherapy lines applied involved two drugs combinations between capecitabine or infusional fluorouracil (5-FU) and irinotecan or oxaliplatin, with or without the addiction of a monoclonal antibody cetuximab or bevacizumab. In all cases, the primary cancer had been treated with surgical resection, and the synchronous or metachronous LM were unresectable. The study was designed in a prospective manner and was approved by the Institutional Review Board. Informed consent was obtained from all patients.
Inclusion and exclusion criteria. The Criteria have been presented in our previous studies as per the TACE guidelines (13, 16, 17), but in brief, the diagnosis of LM from CRC resistant to chemotherapy was histologically confirmed and clearly evaluable as demonstrated by imaging. Before treatment laboratory values were monitored: white blood cell and platelet counts; hemoglobin, bilirubin, creatinine, alanine aminotransferase and aspartate aminotransferase levels; and coagulation values. Contraindications were poor performance status (ECOG ≤2), nutritional impairment, presence of neoplastic ascites, high serum total bilirubin level [>3 mg/dl [51.3 μmol/l]), poor hepatic synthesis [serum albumin level], <2.0 mg/dl- [20 g/l], and renal failure [serum creatinine level], >2 mg/dl 176.8 μmol/L]. Partial or complete thrombosis of the main portal vein was a further exclusion criteria for the procedure, as were cardiovascular and respiratory failure. To ensure adequate treatment compliance, the patients had to be in a good mental state and had to be able to provide their own consent.
Technique and imaging adopted. After the introduction of a 4-5-F pigtail catheter (Pigtail Terumo, Frankfurt/Main, Germany) through the femoral artery, an angiographic survey of the abdominal vessels was performed. With mesenteric arteriography, we checked for the presence of a right hepatic artery by using selective catheterization. A 4-5-F cobra-shaped catheter (Cobra Terumo, Frankfurt/Main, Germany) was placed in the celiac trunk and advanced beyond the gastroduodenal artery. Following insertion of a 5-F Cobra catheter, a 3-F micro catheter (Progreade Terumo, Frankfurt/Main, Germany) was then placed and selective hepatic catheterization of lobar or segmental branches afferent to the neoformed tissue was performed in all patients. DEBIRI (Biocompatibles UK, Surrey, UK) were infused slowly in 5 minutes. In order to prevent RUQP, a 5 ml infusion of 2% lidocaine was administered. In 92 out of 185 procedures, verapamil was added to control arterial spasms induced by the contact of DEBIRI with the endothelium of the vessels. Subsequently, for every treatment, 100-200 mg irinotecan preloaded in 2-4 ml DC Beads of 100-300 / 300-500 pm was administered. A total of 185 DEBIRI procedures were performed (81 TACE procedures with 2 ml of beads preloaded with 100 mgr of irinotecan and 104 with 4 ml loaded with 200 mgr of irinotecan).
Treatment planning and follow-up assessments included an enhanced and contrast-enhanced CT imaging with a multi-metector-computed-tomography of the liver within at least 24 hours in one month and again in three months from the treatment with the evaluation of the enhancement pattern of the target lesions and tumor response rates. Follow up assessment was then performed at every 3-month interval for the first and second years. Twenty-four hours after DEBIRI, tumor shrinkage and necrosis were verified adopting the spiral technique with a section thickness of 4 mm. According to our experience with DEBIRI, a recovery time of 3-8 days after chemoembolization was observed.
Quantitative and statistical analyses. The follow-up after DEBIRI was based on multidetector CT scans and MRI imaging volumetric evaluation of the treated LM. Volume measurement was performed by using the transverse images to evaluate the longest cross-sectional diameter as the length and the perpendicular diameter as the width. The longest diameter was measured on sagittal images. Tumor volume was calculated on the basis of the evaluated diameters on transverse images with the following ellipsoidal volume equation: volume=length × width × height × 0.523. To evaluate treatment success, response was defined in our study following RECIST Criteria (37, 38) as achievement of a shrinkage of the target lesions to a diameter less than 50%. Stable disease was defined as no substantial change in size. Progressive disease was defined as an increase in size of a target lesion or newly developing lesions in the liver. To better define the response we also evaluated the reduction of lesional contrast enhancement. A sample of 82 patients was proposed in order to detect the threshold objective response rate of 70%. The cumulative survival times were calculated beginning with the commencement of the first treatment by using the Kaplan-Meier method. For statistical analysis, we used the χ2 and log-rank tests. The Quality of Life (QoL) was assessed by the procedure before and after completion of the Edmonton SAS questionnaire.

82-year-old woman with a 4.5 cm colon cancer metastasis in liver. Contrast enhanced CT image showing enhancing mass in the right lobe of the liver (A). The image obtained one month after TACE shows necrosis as non-enhancing area.
Results
From December 2005 until September 2011, 82 patients were included in this study who met the inclusion criteria stated above and had documented liver progression of disease following a minimum at least two lines of chemotherapy. All patients were in a good performance status at the time of first DEBIRI treatment, with all having LM from CRC and presenting with metachonous metastases. The average sum of the total lesion sizes that were treated in this study was 12.0 cm, with a range of 6.5 to 32.0 cm.
A total of 35 patients had received at least first line infusional 5-fu and oxaliplatin (FOLFOX) and 27 patients had received capecitabine and oxaliplatin (XELOX). A separate 20 patients had received first-line FOLFOX and bevacizumab.
Fifty patients received a second line therapy: 32 patients received FOLFOXIRI, 15 FOLFOX with/without cetuximab, 3 capecitabine and oxaliplatin/irinotecan. The principal reason for referral and consideration for inclusion in the study was hepatic disease progression.
Treatment feasibility compliance and toxicity. Overall, 185 DEBIRI were administered, with a median of 2.2 (range 1 to 4) based on the extent of liver substitution and the size of liver lesions to be treated. Technically, repeated arterial selective infusion of the appropriate segments of the liver and deliver of 100% of the planned dose was achieved in all 185 treatments. Eighty-one DEBIRI with 2 ml of beads loaded with 100 mg of irinotecan and 104 with 4 ml loaded with 200 mg of irinotecan were delivered.
The majority of adverse effects were pain, nausea, vomiting and liver enzyme alterations, with a vast proportion of them being mild (grade 1-2), but 20 patients (25%) had RUQP grade 3. Immediately after treatment, no major complications such as bleeding, dyspnea or hypertension, were observed. Twenty-four hours later, the laboratory values showed increase of transaminases as 3XN (range 2-6) in 41 (50%) patients and high serum total bilirubin level (>3 mg/dl) in 8 (9%) patients. Nausea and vomiting were the first symptoms appearing within one hour after the procedure in 24 (27%) patients. RUQP appeared within 6 hours, in 34 (40%) patients.
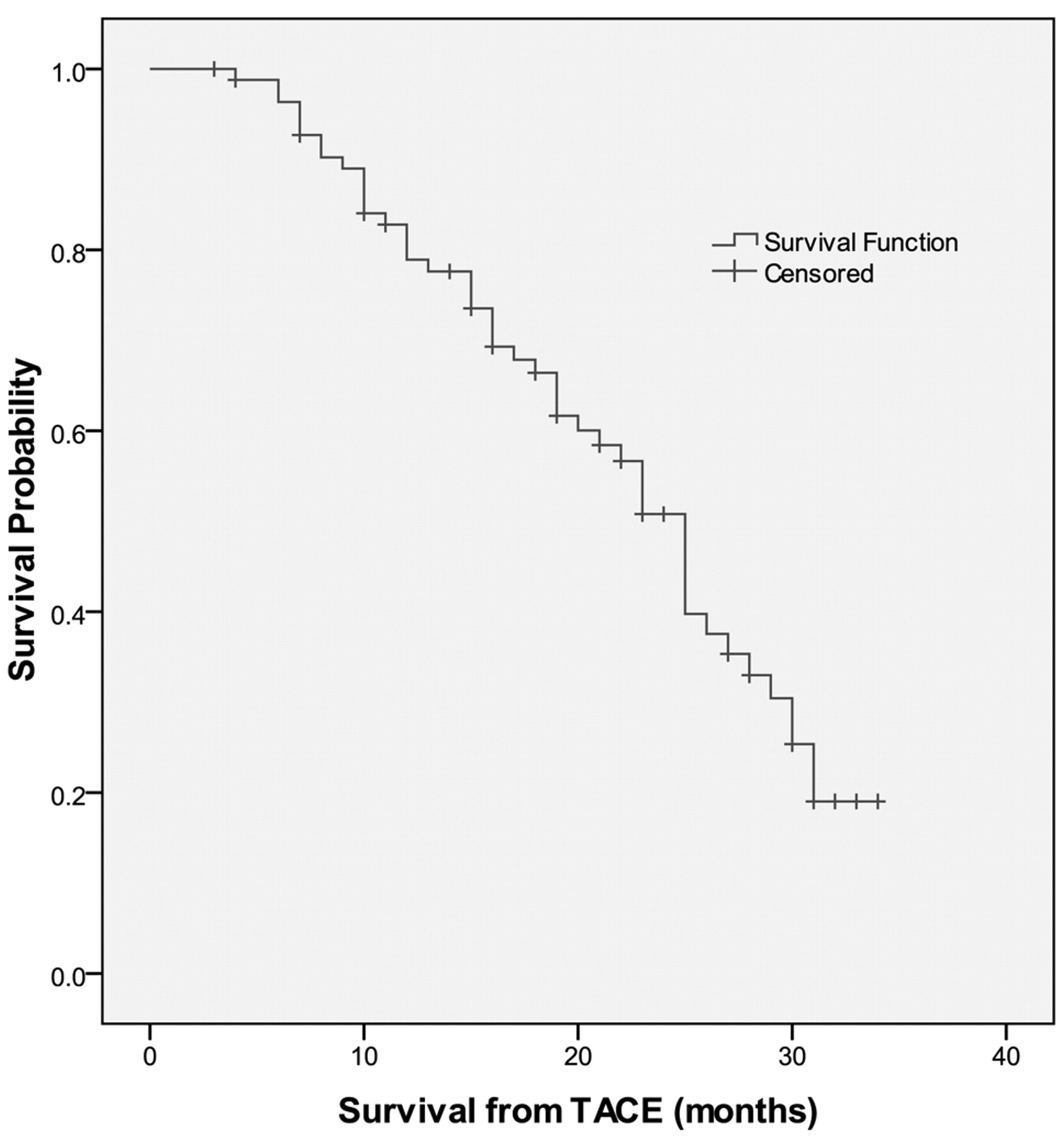
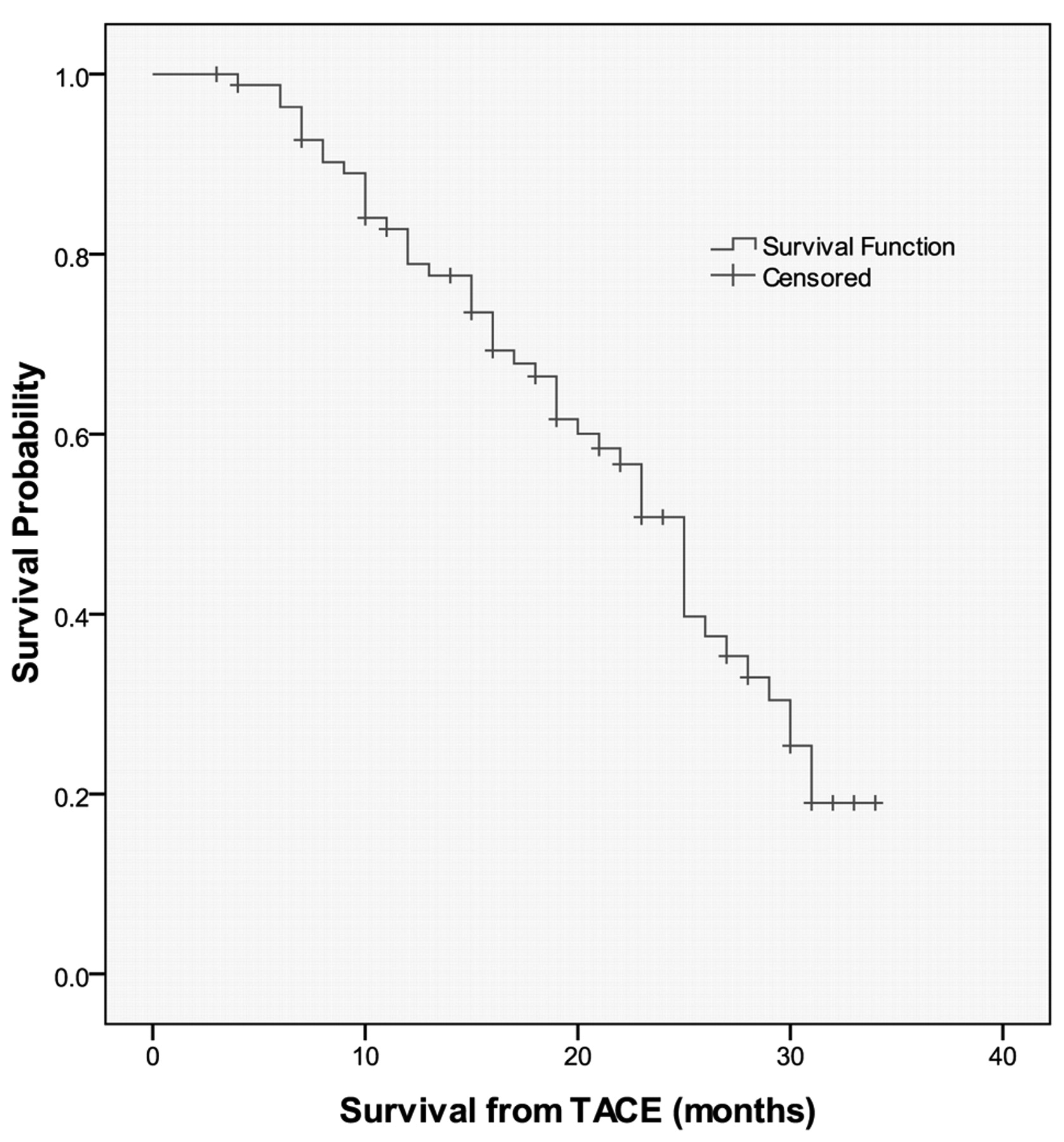
Time to death at time of initial TACE ablation. Kaplan-Meier survival curve for ali patients.
Tumor response and survival. Within one month after treatment, multidetector CT scan showed significant (from 75 to100%) reduction of metastatic contrast enhancement (Figure 1) in all patients. Therapeutic response was observed in 78% of patients at the check point of 3 months. One month after TACE, 75 out of 82 patients (90%) declared a general improvement of QoL lasting 32 weeks (range 3-39). The median survival was 25 (range 6-34) months (Figure 2). The observed time to progression was 8 (range 4-16) months (Figure 3), and the median duration of response was 6 (range 3-10) months (Figure 4). Late toxic effects were the appearance of acute pancreatitis in one patient, and another patient had a liver abscess. Both complications regressed with conservative treatment. The median follow-up was 29 (range 7-48) months. Therapeutic response (fig2) was observed in 78% of patients. At the time of monitoring 48 out of 82 patients have died: 20 due to liver progression and 28 patients due to liver progression and extra target metastases; 34 are still alive with liver disease. Two patients were treated with hepatic resection and are free of disease at 14 and 18 months.
Kaplan-Meier curves for the time to progression for all patients.
Discussion
Our study shows that DEBIRI induced an overall response rate of 78% and a control rate of LM of 8 months in heavily pretreated patients compared with an estimated response rate of less than 15% for further lines of chemotherapy (39). This treatment also demonstrated a prolonged time of survival with a median of 25 months. All patients failed previous chemotherapy and had ongoing liver progression of disease. The data presented are the continuing experience of DEBIRI to which our group has already demonstrated the potential benefit in recalcitrant LM (13, 16, 17, 22).
In recent years it has been shown that metastatic CRC is a disease that can remain confined to the liver for long periods and that an important proportion of patients will not develop metastatic lesions outside the liver. Consistent with this observation, surgical removal of the metastatic lesion can improve survival. Moreover, it has been demonstrated that if it is possible to remove the entire lesion and achieve an R0 resection, with no macroscopic or microscopic residuals, a proportion of patients ranging from 20% lo 40% will not experience disease relapse thus making metastatic CRC limited to the liver a curable disease.
Chemotherapy is still the preferred established treatment in patients with unresectable LM from CRC. Up-front schedules combining either oxaliplatin or irinotecan with 5Fu and folinic acid offers a response rate of 31% to 62% (5-10). A median of progression free-survival from 7 to 9 months and a median overall survival from 14 to 21.5 months in randomized studies were reported (5-10). It is well known that second line chemotherapy combining oxaliplatin or irinotecan with 5-Fu and folinic acid after failed first-line therapy is far less active, with overall response rates ranging from 4% to 21% and a median progression free survival from 2.5 to 4.8 months (39). Recently the combination of biologic agents, such as bevacizumab and cetuximab, have demonstred interesting activity, even in patients with chemotherapy-resistant LM from CRC (8-10). Overall response rates of 23% and a median time to progression of 4.1 months have been observed, while the overall survival was reported to be 8.6 months (8,10).

Kaplan-Meier curves for the time to progression for all patients.
Considering that our research was obtained during the wide increased application of these biologic agents, our results suggest that DEBIRI is a viable option in patients failing oxaliplatin and irinotecan-based chemotherapy. The evidence of response rates in 78% of these patients highlights the fact that the ability to administer a directed amount of cytotoxic agent to LM can theoretically lead to improvement in response rates and potentially increase survival.
The type of toxicity observed was substantially acceptable and demonstrated good compliance in pretreated patients. All planned DEBIRI treatments presented the most common side effects such as nausea, vomiting, and pain. We verified signs of hepatic necrosis that were transient in all patients.
Conclusion
We conclude that DEBIRI is a feasible and promising approach to therapy of LM from CRC after the failure of chemotherapy and biologic agents. It is considered that this treatment could be proposed to increase the proportion of patients who can undergo surgical R0 resections or, in advanced cases, allow protracted local control of liver disease. In both cases, it is reasonable to speculate there should be an impact on overall survival, although no randomized studies have demonstrated this.
It is also important to state that, with the exception of cetuximab-irinotecan combinations in cetuximab-naive patients, no standard third-line treatments are available for LM from CRC. In this regard we, believe that the high proportion of responses obtained deserves great attention and remind, based on standard treatment guidelines and evidence-based medicine, best supportive care would be the optimal treatment choice for the majority of the patients enrolled in our trial.
However, only randomized studies will clarify if DEBIRI can achieve a survival benefit in patients with metastasis of CRC limited to the liver and if this technique is cost-effective compared to standard chemotherapeutic treatments.
- Received October 24, 2011.
- Revision received November 21, 2011.
- Accepted November 22, 2011.
- Copyright© 2011 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Comparison of Response and Outcomes of Drug-eluting Bead Chemoembolization (DEB-TACE) Versus Radioembolization (TARE) for Patients With Colorectal Cancer Liver Metastases
- Hepatic Arterial Infusion of Polyethylene Glycol Drug-eluting Beads for Primary and Metastatic Liver Cancer Therapy
- Chemoembolization in Colorectal Liver Metastases: The Rebirth