


Abstract
Background: The aim of this study was to analyze the significance of dissection of unsuspicious para-aortic lymph nodes (PAN) in patients with advanced endometrial carcinomas with intra- or extra-abdominal metastasis. Patients and Methods: We conducted a retrospective comparison of the results of PAN dissection versus non-dissection for endometrial carcinomas with macroscopic metastatic lesions beyond the uterus (without significant swelling of the regional lymph nodes, including PAN), whose lesions were completely resected. Results: Disease-free survival and overall survival did not exhibit a significant difference between the two groups. Multivariate Cox proportional hazards analysis demonstrated that PAN dissection was not an independent prognostic factor for survival. The frequency of PAN involvement at the first recurrence did not differ between the two groups. Conclusion: For advanced endometrial carcinomas with macroscopic metastatic lesions beyond the uterus, without significant swelling of regional lymph nodes, PAN dissection may be omitted without a significant adverse effect on prognosis and survival.
Uterine endometrial carcinoma, already the most common malignancy of the female pelvis, has had an apparent increasing incidence during the last three decades in the United States (1). When this carcinoma is still confined to the uterus (stage I) it has a good prognosis; however, tumors which progress beyond the uterus confer a dramatically poorer prognosis. For endometrial carcinoma cases with intermediate or high-risk factors of recurrence, a retrospective (SEPAL) cohort study has suggested that there is a therapeutic role to be gained for a combined dissection of the pelvic lymph nodes (PLN) and para-aortic nodes (PAN) (2). However, according to a retrospective study recently conducted by our group on endometrial carcinoma cases in which postoperative adjuvant chemotherapy using combined platinum, anthracycline and taxane derivatives was performed, not only was PAN dissection not associated with a better survival, but in fact, the procedure was adversely associated with significantly increased operative time and total blood loss (Okazawa et al., submitted).
For advanced endometrial carcinoma cases with intra- or extra-abdominal metastasis, a significant role for cytoreductive surgery was demonstrated (3, 4). In these studies, resection of the metastatic lesions and swollen PAN was performed with or without regard to dissection of any unswollen PAN. The survival significance of co-dissection of the unswollen PAN has, thus, remained unclear. In our present study, we performed a retrospective analysis of the survival effect of PAN dissection for advanced endometrial carcinoma cases with intra- or extra-abdominal metastasis beyond the uterus (excluding overt PLN or PAN metastasis) which received postoperative adjuvant chemotherapy using platinum and taxane (with or without anthracycline).
Patients and Methods
A retrospective comparison was conducted of the efficacy of PAN dissection for patients with endometrial carcinomas with metastatic lesions beyond the uterus (unaccompanied by significant swelling of regional lymph nodes), including PAN whose carcinoma lesions were thought to be completely resected. This study analyzed cases treated during the period 2000-2010 at the Department of Obstetrics and Gynecology of the Osaka University Hospital and the Department of Gynecology of the Osaka Medical Center for Cancer and Cardiovascular Diseases. Written informed consent was obtained from all patients before any treatment commenced. This study was approved by the Institutional Review Board and the Ethics Committee.
PAN dissection was performed under highly similar indications in both hospitals, including a myometrial invasion depth of >1/2 of total thickness and/or an atypical histology (such as grade 3 endometrioid adenocarcinoma, or a clear cell or serous papillary carcinoma), for endometrial carcinoma without intra- or extra-abdominal metastasis, irrespective of swelling of the PLN or PAN. In this study, not all cases with obvious macroscopic intra- or extra-abdominal metastasis lesions beyond the uterus, but without overt swelling of the PLN and PAN, received dissection of the PAN. Whether or not a PAN dissection was performed was left to the informed choice of the patient. The cases in which PLN dissection was not performed were excluded from analysis.
Metastasis to PAN was assessed with either a helical computerized tomography (CT) scan or magnetic resonance imaging (MRI). Adjuvant combination chemotherapy using taxane (paclitaxel) and platinum (carboplatin), with or without the anthracycline epirubicin, (TEC) or (TC), respectively, was performed. A regimen of TEC (150 mg/m2 paclitaxel, 50 mg/m2 epirubicin, and area under the curve (AUC) 4 carboplatin), based on our own phase I/II studies (5), was administered at the Osaka University Hospital every 3-4 weeks for 6 courses. For the alternative TC therapy, conducted at the Osaka Medical Center for Cancer and Cardiovascular Diseases, paclitaxel (175 mg/m2) and carboplatin (AUC=5) were administered intravenously every 3-4 weeks for 6 courses, based on published protocols (6, 7).
The clinicopathological features of these cases, including the age of the patient, the disease histology and stage, and the number of the metastatic regions, were retrospectively reviewed utilizing their clinical records, including physical examination notes, radiological and histopathology reports, and operative records. Disease-free survival (DFS) was measured from the initial surgery to the date of the radiologic or pathologic diagnosis of recurrence, or to the date of the last follow-up, and overall survival (OS) was defined as the period from the initial surgery to the patient's disease-specific death, or to the date of the last follow-up.
Statistical analysis. MedCalc (MedCalc Software, Mariakerke, Belgium) was used for the statistical analyses. The distribution of patients' ages was analyzed by the Mann-Whitney U-test. The distribution of tumor histology and stage, number of metastatic regions and the frequency of PAN involvement at the first recurrence were all analyzed by the Fisher's exact test. DFS and OS curves were constructed using the Kaplan-Meier method and were evaluated for statistical significance by the log-rank test. Results were considered to be significant when the p-value was less than 0.05.
Results
Clinical characteristics of the cases in which PAN dissection was or was not performed. At the Osaka University Hospital and the Osaka Medical Center for Cancer and Cardiovascular Diseases, 34 endometrial carcinomas with macroscopic metastases beyond the uterus, but having no significant swelling of regional PLN or PAN, were reported to have been completely resected during the study period. Among them, systemic PAN dissection was performed in 19 cases. Distributions of age, histology, stage and number of metastatic regions were not significantly different between the cases in which PAN dissection was performed (PAN+ group) and those in which PAN dissection was not performed (PAN− group) (Table I).
Characteristics of patients treated with or without para-aortic lymph nodes (PAN) dissection. Background characteristics of the two groups were not significantly different.
TEC therapy was performed in 10 and TC treatment in 9 out of the 19 cases whose PAN was dissected, and in 7 and 8, respectively, out of the 15 cases whose PAN was not dissected. These proportions for regimens of adjuvant chemotherapy were not significantly different.
Diagnostic significance of PAN dissection. PAN metastasis was histologically diagnosed in 2 out of the 19 cases whose PAN had been found to be unswollen by helical CT or MRI. PLN metastasis was also detected in these cases. Moreover, these two cases were diagnosed as stage IVb due to upper-abdominal metastasis. There was no case in which the stage of the disease was changed after surgery.
Survival effect of PAN dissection. The DFS and OS curves of the PAN+ and PAN− dissection groups are shown in Figure 1. The median follow-up period for the two groups was 24 months (range 3-63 months) and 43 months (7-61 months), respectively. DFS and OS did not exhibit a statistically significant difference between the PAN+ and − groups (p=0.13 by the log-rank test, hazard ratio (HR)=1.959; 95% confidence interval (CI)=0.774-4.965; and p=0.17 by the log-rank test, HR=2.430; 95% CI=0.201-8.396, respectively).
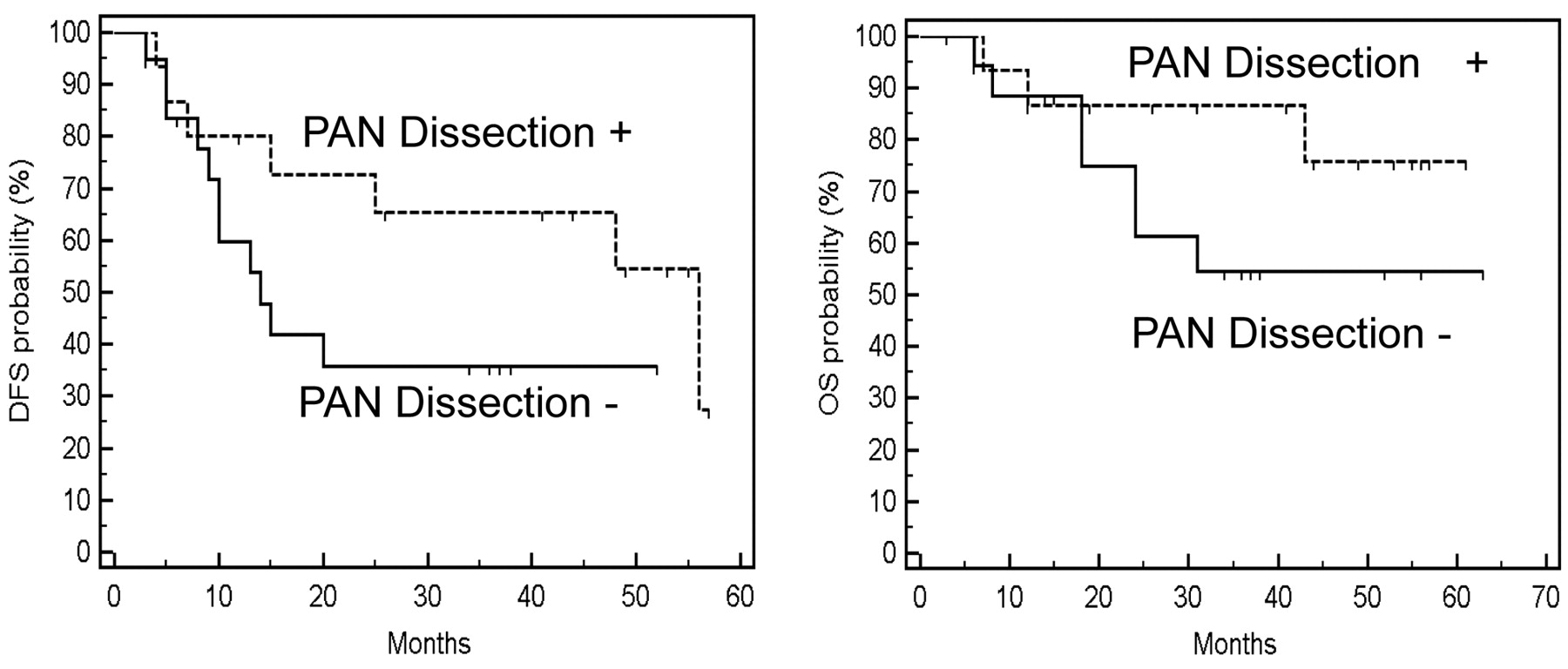
Disease-free survival (DFS) and overall survival (OS) in the patients treated with or without PAN dissection. Neither DFS nor OS demonstrated significant differences between the patients treated with or without PAN dissection (p=0.13 and p=0.17, respectively, by the log-rank test).
Multivariate analysis of clinical factors for survival effect. We utilized the multivariate Cox proportional hazards model in order to find evidence to further support our interpretation of these results, namely that the dissection of unswollen PAN does not improve survival of patients with advanced endometrial carcinoma with intra- or extra-abdominal metastasis. We found that the number of metastatic regions was an independent factor for DFS (Table II). The adjusted HR for the number of metastatic regions (1 versus ≥2, i.e., single versus multiple regions) was 3.633 (95% CI=1.126-11.716; p=0.032) for DFS. The univariate Cox proportional hazards analysis revealed that the DFS probability of cases with a single metastatic region was significantly better than that of cases with multiple metastatic regions (HR=3.506, 95% CI=1.392-8.833; p=0.016) (Figure 2). On the other hand, PAN dissection was shown not to be a significantly independent factor for either DFS or OS (Tables II and Table III).
Frequency of the first recurrence to the PAN. The frequency of PAN involvement at the first recurrence of the tumor was compared between the two treatment groups. The first recurrence at PAN was detected in 2 out of 19 PAN dissection + cases, and in 2 of the 15 PAN dissection – cases. A statistically significant difference was not detected (p=0.80 by Fisher's exact test). Moreover, in one of the two recurrent cases at PAN, pathological diagnosis of PAN metastasis had been made at the initial PAN dissection.
Discussion
For endometrial carcinoma, the therapeutic significance of PAN dissection has been an issue of great debate. In the early stages of endometrial carcinoma, several randomized studies have indicated that systematic dissection of the PLN has little therapeutic value (8, 9). However, for endometrial carcinoma cases with intermediate and high risk factors of recurrence, a retrospective SEPAL cohort study indicated there was a possible therapeutic role for a combined dissection of PLN and PAN (2). However, the adjuvant therapy was not standardized in this study; roughly one-fifth of the cases did not receive an adjuvant therapy, another fifth underwent radiation, and the others had a cisplatin-based chemotherapy.
The combination adjuvant chemotherapy of platinum, taxane and anthracycline has recently come to be regarded as the gold standard for treatment of advanced or recurrent endometrial carcinomas (10-12). Our own previous study showed that PAN dissection was not associated with any better survival in endometrial carcinoma cases in which a postoperative adjuvant chemotherapy using platinum, anthracycline and a taxane derivative was performed. On the contrary, PAN dissection was associated with adverse effects that included increases in both operative times and total blood loss (Okazawa et al., submitted). Still, for more advanced cases of endometrial carcinoma, those with intra- or extra-abdominal metastasis, the significant role of cytoreductive surgery of any visible lesions for increased survivability has been clearly demonstrated (3, 4).
Multivariate Cox proportional hazards analysis for disease-free survival (DFS). The adjusted hazard ratio (HR) for the number of metastatic regions being ≥2 was significantly higher than that for the number of metastatic regions being <2 (adjusted HR=3.633, 95% CI=1.126-11.716, p=0.032).
Multivariate Cox proportional hazards analysis for overall survival (OS). None of the variables investigated exhibited independent prognostic significance for OS.
Based on these conflicting findings, the prognostic and therapeutic significance of dissection of unswollen PAN for advanced endometrial carcinoma cases with intra- or extra-abdominal metastasis is of great interest to us. First, diagnostic significance was analyzed. In cases in which PAN dissection was performed, there were two cases in which PAN metastasis was pathologically diagnosed. However, in these cases, metastases of the PLN and upper abdomen were also detected and up-staging due to PAN metastasis was not required after PAN dissection. These results imply that diagnostic value of PAN dissection may not be significant. Next, a retrospective comparison of advanced endometrial cases which progressed beyond the uterus (without regional lymph nodes swelling) was conducted. Whether or not a PAN dissection was performed was left to the informed choice of the patients. Those cases whose malignancies were obviously not completely removed by surgery were excluded from the analysis. The clinical characteristics of the patients who received PAN dissection and those who did not receive PAN dissection are shown in Table I. All the patients underwent postoperative adjuvant with either TEC or TC therapy. The proportions of these two regimens were not different significantly in the two groups.

Disease-free survival (DFS) by the number of metastatic regions. DFS of the patients with two or more metastatic regions was significantly worse than that of the cases with a single metastatic region (p=0.016 by the log-rank test).
The therapeutic effect of PAN dissection was analyzed. The DFS and OS of the PAN+ group tended to be better than those of the PAN− group, but this improvement did not rise to the level of statistical significance (Figure 1). The multivariate Cox proportional hazards model demonstrated that the number of metastatic regions was an independent factor for DFS; however, PAN dissection was not shown to be a significantly independent factor for either DFS or OS (Tables II and III). These results show that the status of progression of the disease was more important than PAN dissection, implying that dissection of unswollen PAN does not improve survival of patients with advanced disease with macroscopic intra- or extra-abdominal metastasis without regional lymph node swelling.
It might be argued that dissection of even unswollen PAN may be helpful for accurate surgical staging. However, in our study, a PAN metastasis was histologically diagnosed in only 2 out of the 19 cases whose PAN had been determined to be unswollen by helical CT or MRI, and in these cases, due to co-metastasis to other distant sites, the stage of the disease was not further upgraded. Moreover, we found that the frequency of PAN involvement at the first recurrence of the tumor was similar in the PAN+ and PAN− groups. These results may imply that PAN dissection at the initial surgery does not prevent the first recurrence of PAN in these cases.
In this retrospective study, we show that PAN dissection was not an independent prognostic factor for advanced endometrial carcinoma with macroscopic intra- or extra-abdominal metastasis without regional lymph node swelling, in which adjuvant combination TEC or TC chemotherapy was used. These results imply that routine PAN dissection may be objectively omitted for advanced endometrial cases which have progressed beyond the uterus without regional lymph node swelling. Further prospective studies to analyze the significance of PAN dissection are still required.
Acknowledgements
The Authors would like to thank Dr. G. S. Buzard, US CDCP, for his constructive editing of our manuscript.
Footnotes
-
↵* These Authors contributed equally to this work.
-
This article is freely accessible online.
-
Conflict of Interest Statement
None of the Authors has any conflict of interest to declare.
- Received October 13, 2011.
- Revision received November 14, 2011.
- Accepted November 15, 2011.
- Copyright© 2011 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}