


Abstract
Background: In various tumor entities, expression of cancer stem cell (CSC) antigens has been proven to be prognostically unfavorable. However, for lung cancer, the data are scant and conflicting. Patients and Methods: The CSC antigens CD117/c-KIT, CD133 and breast cancer resistance protein-1 (BCRP1/ABCG2) were immunohistochemically analyzed in tissues from a total of 133 completely resected stage I/II non-small cell lung cancer (NSCLC) patients with a median follow-up time of 53.8 months. Their expression was related to clinicopathological characteristics, angiogenic features and prognosis. Results: Cox proportional hazards regression analysis revealed no association between CSC antigens, disease-free survival or overall survival (OS). However, in the subgroup of patients with relapse and tumors >3 cm, there was a trend towards worse OS upon expression of CD117 (hazard ratio=2.6, 95%, confidence interval=0.8-8.3, p=0.080). Except for CD133, which was overrepresented in T1 tumors (p=0.001), the CSC antigens were not linked to clinico-pathological characteristics or angiogenic features. Conclusion: In resected early-stage NSCLC, CSC antigens show no association with prognosis. However, in patients with relapse and tumors >3 cm, expression of CD117 might predict worse OS.
- Non-small cell lung cancer
- cancer stem cell antigens
- biomarkers
- prognosis
- CD133
- CD117
- BCRP1
- tissue microarrays
Lung cancer is the leading cause of cancer-related deaths worldwide. Non-small cell lung cancer (NSCLC) accounts for 80%-85% of all lung cancer cases and is curable solely by resection (1). About one third of patients with NSCLC present with a resectable stage (I-IIIA) (2). However, depending on the stage and completeness of resection, ≥50% of these patients experience disease relapse and die within five years after surgery (3). Although various clinicopathological and molecular markers that predict relapse and/or survival in NSCLC have been identified, neither neoadjuvant nor adjuvant treatment regimens have substantially improved the prognosis (3-8). Since the majority of patients experience distant relapse, micrometastatic spread of chemoresistant cells that survive (neo)adjuvant therapy was hypothesized. In recent years, so called cancer stem cells (CSC) have been detected in various tumor types. These were predominantly characterized by the expression of CD133 (9-11). In murine models of NSCLC, CD133-positive cells were highly tumorigenic, metastatic and spared by in vivo treatment with cisplatin (12). Moreover, they showed coexpression of other putative CSC antigens such as CD117/c-KIT or breast cancer resistance protein-1 (BCRP1/ABCG2) and an increased production of proangiogenic and mitogenic cytokines (13-17). In glioma, colorectal, breast and gastric cancer, expression of CD133 has been shown to poorly predict prognosis (18-21). However, in NSCLC the data are conflicting: A study of Salnikov et al. of 88 resected NSCLC demonstrated an association of CD133 with the expression of resistance-related proteins, but not with clinicopathological characteristics, patients‘ survival, expression of proangiogenic cytokines, oncogenes or the proliferative activity and apoptotic susceptibility of the tumor cells (22). Likewise, Hilbe et al. found no prognostic significance of CD133 in 63 resected NSCLC, and moreover, no significant relation to the expression of vascular endothelial growth factor receptor-2 and the microvessel density (MVD) (23). In contrast, Li et al. reported in 145 resected NSCLC stage I patients that CD133/BCRP1 double-positive cases (23%) showed an increased microvessel density, production of proangiogenic cytokines and risk of relapse, while a recent study of Woo et al. on 177 resected stage I adenocarcinomas demonstrated an increased risk of disease recurrence in those with high CD133 expression (24, 25). To shed light on these divergent findings, we analyzed a total of 133 resected early-stage NSCLC patients for the prognostic significance of the CSC antigens CD117, CD133 and BCRP1. Moreover, the expression of these antigens was related to clinicopathological characteristics and angiogenic features associated with metastasis.
Patient characteristics.
Immunohistochemical results for cancer stem cell (CSC) antigens and angiogenic features.
Patients and Methods
Patient and sample characteristics. A total of 133 previously untreated NSCLC patients who underwent complete pulmonary resection between 2002 and 2004 at the Department of Thoracic Surgery, Thoraxklinik/University of Heidelberg were analyzed. Tissue specimens and follow-up data were obtained from the tissue bank and the lung cancer registry of the Thoraxklinik and the tissue bank of the National Center for Tumor Diseases (NCT), University of Heidelberg. Patients had provided informed consent following the guidelines of the 2008 revision of the declaration of Helsinki and the local Ethics Committee of the Medical Faculty Heidelberg. Preoperative and follow-up assessments were performed according to the guidelines published by the German Respiratory Society (6). Staging was carried out following the 2009 revision of the lung cancer staging system (26). No patient had received adjuvant treatment, whereas all patients with relapse had received radio- and/or chemotherapy. Eighty-six patients had immunohistochemical results for the entire set of antigens available and were considered for multivariate analysis. For subgroup analysis of patients with relapse, all recurrences (n=45) occurring within the total population (n=133) were considered. A detailed overview of patient characteristics is given in Table I.
Staining details.
Tissue microarrays (TMA) and immunohistochemical analyses. TMA of pulmonary resections were prepared by the tissue bank of the NCT as previously described (27). Two different tumor areas (core and invasion front each) of each patient tissue and histologically normal lung were spotted in technical duplicates. The tissue cores were 1.5 mm in diameter and arranged as mirror-imaged. Deparaffinized 2 μm tissue sections of the TMA were pretreated in antigen retrieval buffer pH 6 (DAKO, Glostrup, Denmark) to block unspecific binding. Sections for CD133 and BCRP1 staining were additionally blocked by avidin/biotin treatment. Subsequent steps were performed in an immunostaining device (DAKO Autostainer). The immunostaining protocol was based on the avidin-biotin peroxidase principle using 3-amino-9-ethylcarbazole (AEC) as chromogen and hematoxylin for counterstaining. The following primary antibodies, clones and dilutions were used: CD117 (mouse polyclonal, 1:50; DAKO), CD133 (rabbit polyclonal [ab19898], 1:100), BCRP1 (mouse clone BXP-21, 1:100; both: Abcam, Cambridge, MA, USA). For negative control, the primary antibody was omitted. The analysis was performed by two independent observers (E.H. and S.G.) and included assessment of the staining pattern (focal, diffuse), cellular localization (membranous, cytoplasmic, nuclear) and proportion of positive cells (0: negative, 1: <20%, 2: ≥20% - 40%, 3: >40%). Samples were considered positive if either diffuse expression or at least one focus with weak, but distinct staining was present in one out of four tissue cores per sample. The representativeness of the TMA was assessed by comparison with corresponding tissue sections of 20 specimens (10 adenocarcinomas, 10 squamous cell carcinomas) and presented full concordance. Due to predominantly focal expression of CD133 and BCRP1, the reliability of the TMA results was additionally analyzed in multilevel tissue sections of 20 CD133/BCRP1-negative samples derived from T2 tumors. Except for one CD133-positive focus in a single tissue section, the results showed full concordance. For analysis, the TMA was scanned at ×400 magnification using Aperio ImageScope v10.1.3.2028 software (Aperio Technologies Inc., Vista, CA, USA). The vasculature was visualized by use of a CD34 antibody (mouse clone QBend10, 1:25; DAKO). Analysis of the vascular architecture (alveolar, angiogenic) was carried out according to Reinmuth et al. (28). The MVD (low, intermediate, high) was determined according to Chalkely (29).
Statistical analyses. The follow-up was defined as the Kaplan-Meier estimate with reversed status indicator. Death censored the true but unknown observation time, censoring was interpreted as endpoint. Thus, the unobservable follow-up time of a deceased patient was interpreted as the follow-up time that potentially would have been obtained if the patient had not died. Survival time was determined from the date of first diagnosis until last follow-up or reported death. Non disease-related death was censored. The disease-free survival (DFS) was determined from the date of first diagnosis until diagnosis of relapse or disease-related death. Survival times were analyzed using the Kaplan-Meier method and the log-rank test. For multivariate analysis the Cox proportional hazard model was used. Chi-square test and Wilcoxon rank-sum test were used to evaluate the difference between groups. P<0.05 was considered statistically significant. The statistical analyses were performed using SAS® version 9.2 (SAS Institute, Cary, NC, USA).
Results
Patient characteristics. Data of a total of 133 previously untreated patients who underwent complete pulmonary resection for early stage NSCLC (IA-IIB) were analyzed. The median follow-up time was 53.8 months. The relapse rate was 34%, comprising 26% distant and 8% local relapses. The 1-, 2- and 3-year overall survival (OS) rates were 95%, 90% and 82%, respectively. The mean age at diagnosis was 63.7±8.2 years. The majority of patients were male (74%) and had stage I disease (65%). A total of 41% of the patients had squamous cell carcinoma, 42% adenocarcinoma, 1% large cell carcinoma, 14% pleomorph carcinoma and 2% not otherwise specified NSCLC. Overall, 86 patients were considered for multivariate analysis and showed no essential deviations from the clinicopathological characteristics of the total population (Table I).
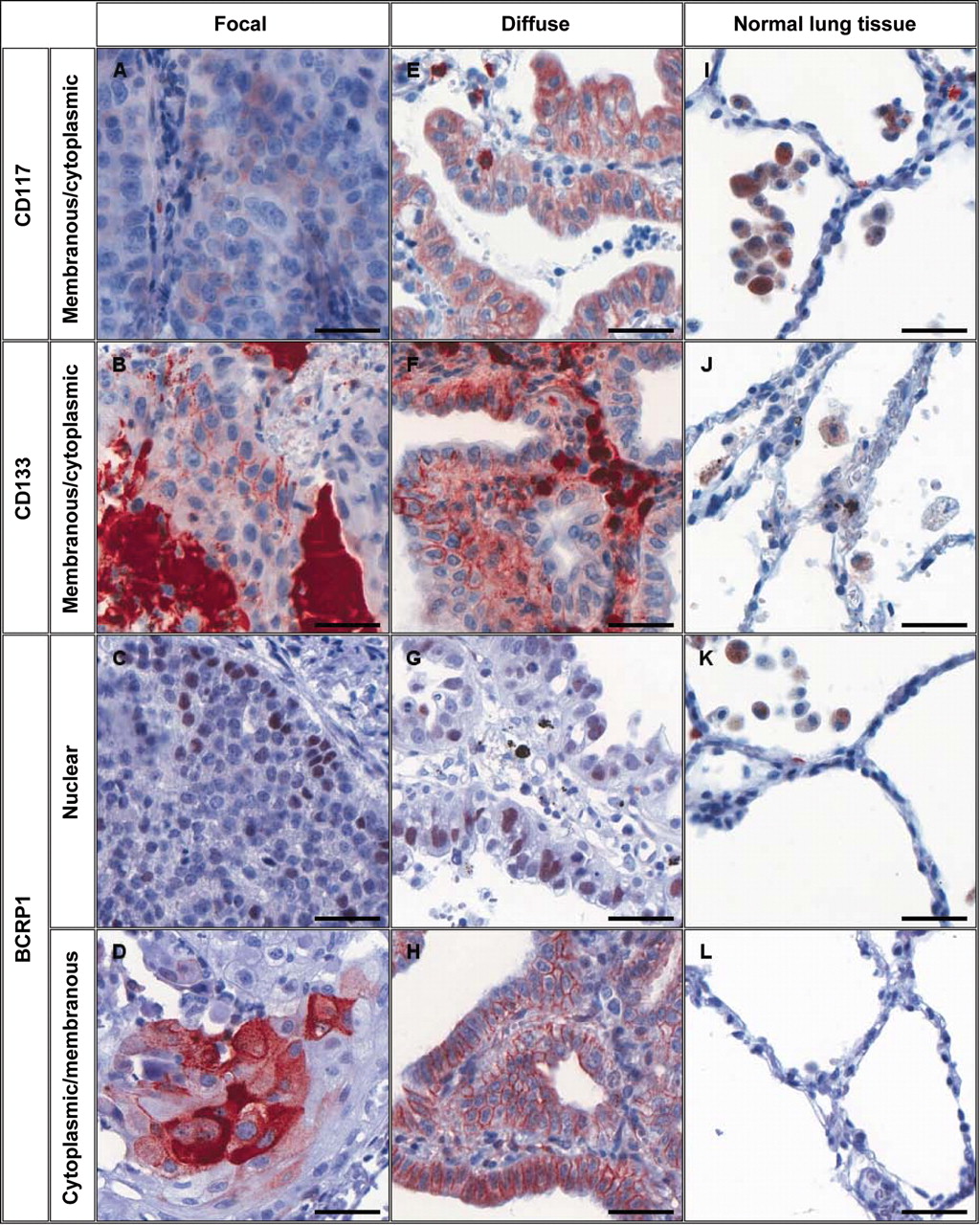
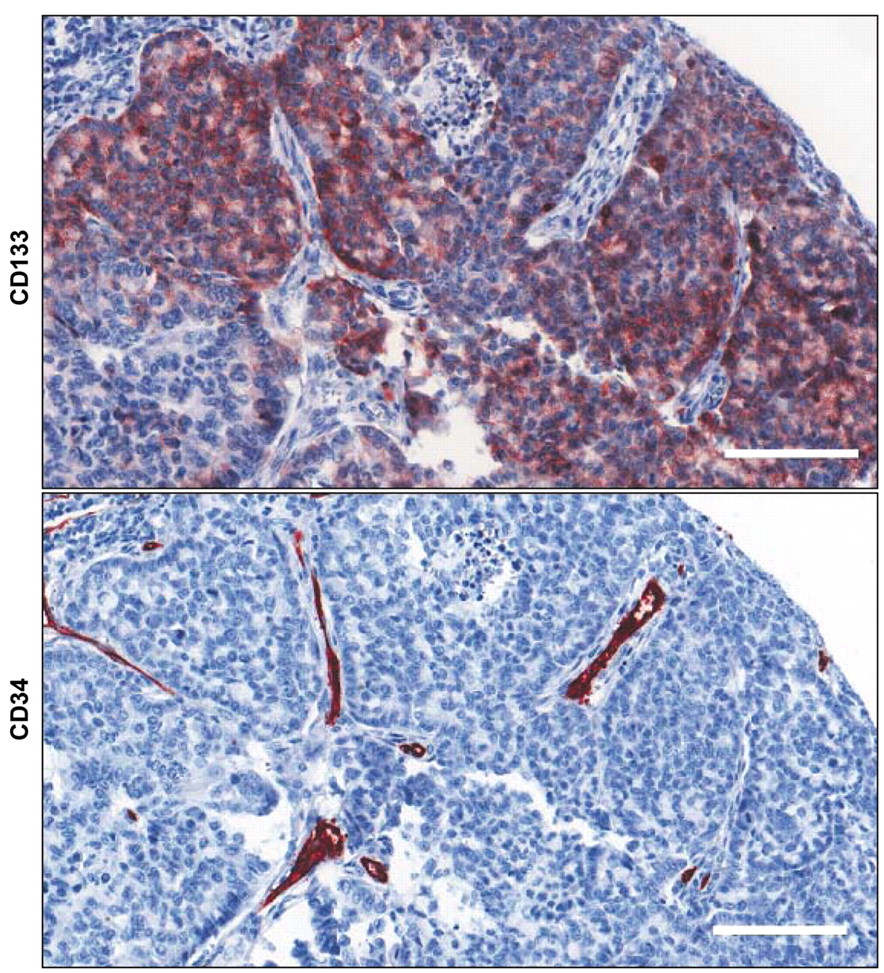
Expression of CSC antigens in NSCLC and corresponding normal lung tissue. Expression of the CSC antigens CD133, BCRP1 and CD117 was positive in 15% (13/86), 34% (29/86) and 50% (43/86) of the samples, respectively, while normal lung tissue displayed expression of these antigens in far below 1% of the epithelial cells (Table II). Samples were considered as positive if diffuse expression or at least one focus with weak, but distinct staining was present in one out of four tissue cores per sample. A total of 85% of the CD133-positive samples exhibited coexpression of BCRP1, 77% coexpression of CD117, 54% expression of all antigens and none coexpression of the endothelial marker CD34. The topological organization, proportion of positive cells and cellular localization varied substantially between the CSC antigens (Table III, Figures 1 and 2): While CD117 exhibited predominantly diffuse staining, CD133 and BCRP1 displayed mainly focal expression. In the majority of samples, CD133 and BCRP1 were expressed in ≤20% of the tumor cells, whereas CD117 stained frequently positively in >20% of the tumor cells. CD133 and CD117 exhibited membranous and sometimes cytoplasmic staining, while BCRP1 exhibited no preferential localization and additionally displayed nuclear staining.

Representative immunostaining of cancer stem cell (CSC) antigens. The hematoxylin-stained tumor sections show focal (left column, squamous cell carcinoma) and diffuse immunostaining (middle column, adenocarcinoma) of CSC antigens. While CD117 (A, E) and CD133 (B, F) exhibit membranous and sometimes cytoplasmic staining, breast cancer resistance protein-1 (BCRP1) displays membraneous, cytoplasmic (C, G) and/or nuclear staining (D, H). Except for nonspecific staining of macrophages, normal lung epithelium contains <1% positive cells (right column). Magnification: ×200, scale bar: 50 μm.
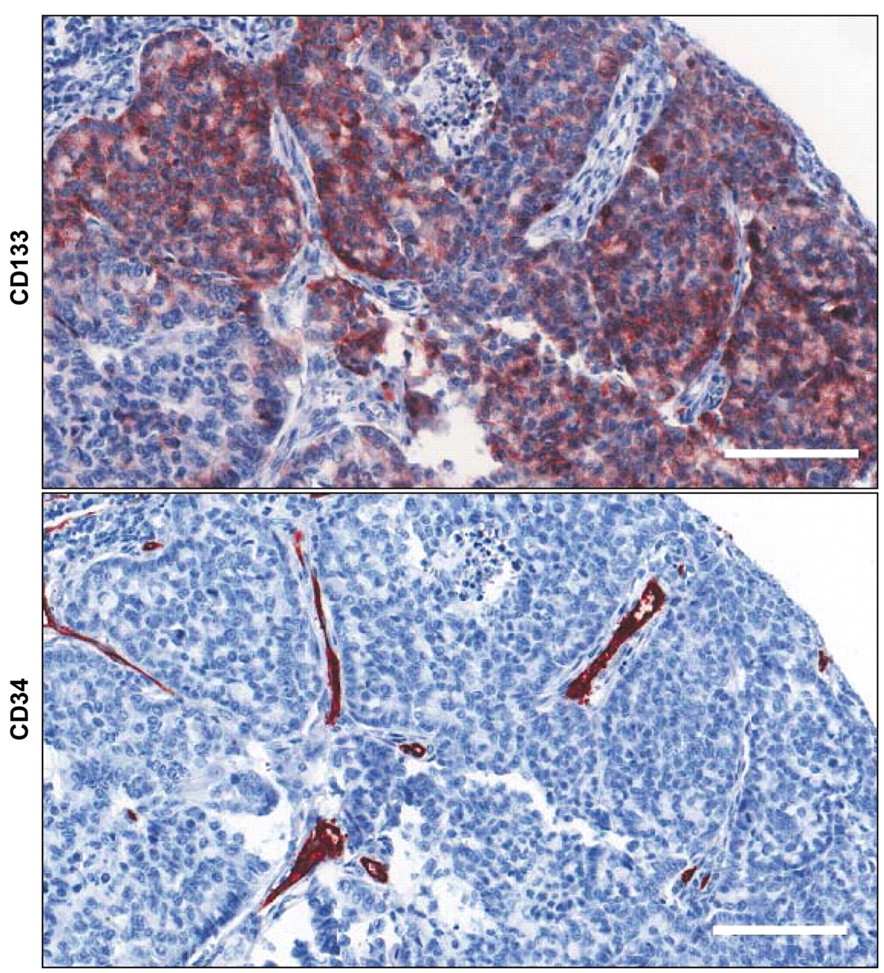
Lack of coexpression of CD133 and CD34. The hematoxylin-stained tumor sections show no coexpression of CD133 and the endothelial marker CD34. Magnification: ×200, scale bar: 50 μm.

Representative immunostaining of the vascular architecture. The hematoxylin-stained tumor sections show representative alveolar and angiogenic vascular architecture. The alveolar architecture is characterized by tumor cells filling the alveolar spaces and exploiting the pre-existing vessels of the alveolar septa, whereas the angiogenic architecture shows a disorganized microvessel pattern. Endothelial cells are visualized by CD34 immunostaining. Magnification: ×100, scale bar: 100 μm.
CSC antigens show no significant association with clinicopathological characteristics or angiogenic features. Except for CD133, positivity for which was overrepresented in T1 tumors (p=0.001), univariate analysis revealed no association between positivity for the CSC antigens and gender, grading, N and T status, the proportion of metastatic lymph nodes or age (Table IV). Moreover, none of the CSC antigens showed a relation to angiogenic features comprising the MVD and the vascular architecture (Table V, Figure 3). Angiogenic architecture itself was associated with an increased risk of relapse in univariate analysis (hazard ratio (HR)=3.5, 95% confidence interval (CI)=0.8-15.3, p=0.032), while mulitvariate analysis was non-significant (p=0.092; Table VI).
CSC antigen expression in the primary tumor is not associated with prognosis, but might predict worse survival after relapse and conservative treatment. The expression of CSC antigens was not associated with DFS or OS in our population (Table VI). However, positivity for CSC antigens indicates a drug-resistance phenotype and thus we analyzed their prognostic significance in the subgroup of patients with relapse who had undergone radio- and/or chemotherapy after recurrence. Within the median follow-up time, 45 individuals (34%) experienced relapse, out of which 37 had available immunohistochemical data for CD133 and BCRP1, and 40 for CD117. Since the number of T1 tumors in this subgroup was not sufficient for analysis, only patients with tumors >3 cm were considered. In total, 27 patients were analyzed for CD133 and 28 patients for BCRP1 and CD117. While expression of CD133 (p=0.445) and BCRP1 (p=0.611) showed no association with OS (data not shown), patients with CD117-positive tumors displayed a trend towards an increased risk of disease-related mortality (HR=2.6, 95% CI=0.8-8.2, p=0.080; Figure 4).
Discussion
The prognostic significance of CSC antigens has been presented in various tumor types, whereas the data for NSCLC are conflicting (18-25). Two Asian studies of 145 and 177 resected stage I patients demonstrated a relation of CD133/BCRP1 or CD133 expression to prognosis, while two European studies of 63 and 88 Caucasian patients with stage I-III disease failed to demonstrate such correlation (22-25). We analyzed a total of 133 Caucasian patients with stage I/II disease for the prognostic significance of the CSC antigens CD133, BCRP1 and CD117. In line with previous studies in Caucasian patients, we found no association between CSC antigens and DFS or OS (22, 23). Various reasons might explain these divergent findings between Asian and European studies: First of all, the Asian studies comprised exclusively patients with stage I disease and in the case of Woo et al. single histology (adenocarcinoma) cases, while the European studies analyzed patients with stage I-III disease and cases of various histologies (22-25). Moreover, the European studies included predominantly males, whereas the gender distribution of at least one Asian study was balanced (22, 23, 25). Among these features, particularly the stage is an established and strong prognostic factor in resected NSCLC that might have hampered significant findings in the European studies (3). Moreover, ethnical aspects have to be considered. Systematic comparisons of Asian and European NSCLC patients indicated considerable molecular differences between these groups (30). Finally, technical differences have also to be regarded. The studies used various antibodies and cut-off points for CD133 ranging from distinct proportions of positive cells to mere qualitative aspects (22-25). In contrast to Woo et al., the antibody used in the current analysis was directed against an intracellular peptide epitope of CD133 and not a glycosylated extracellular domain which might be subject to environmental degradation and distort the staining results (31, 32). An analysis in leukemia cells indicated, moreover, that different CD133 epitopes might also recognize different subsets of cells and thus potentially contribute to divergent study results (33). In any event, all studies using the intracellular peptide-directed antibody failed to demonstrate a prognostic significance of isolated CD133 expression (22, 24).
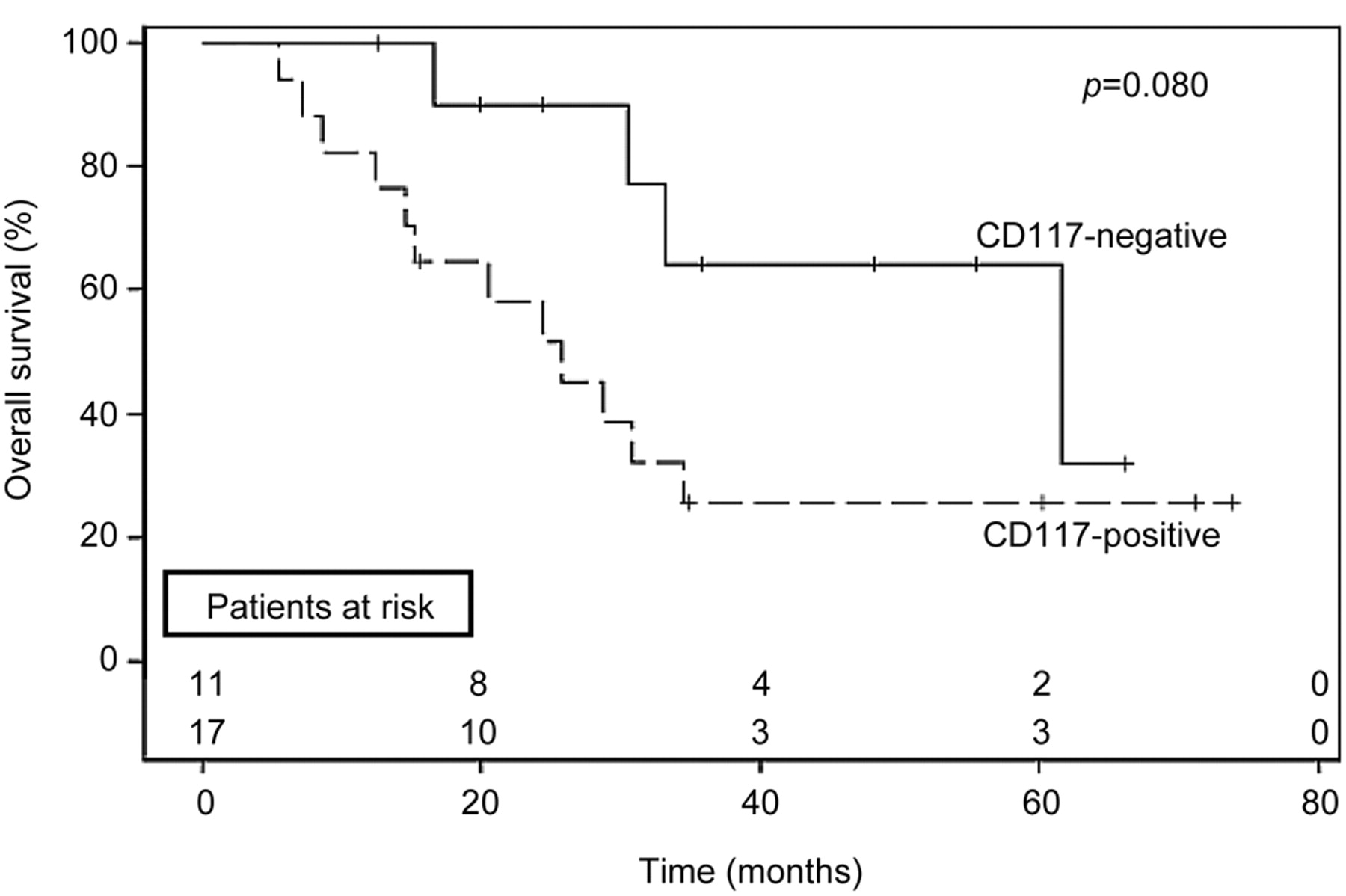
Prognostic significance of primordial CD117 expression in patients with NSCLC relapse. The survival curve (Kaplan-Meier estimate) shows a trend towards worse survival in patients with relapse, whose primordial tumor was >3cm and displayed expression of CD117. All such patients had received radio- and/or chemotherapy after recurrence. The numbers above the x-axis represent the patients at risk at the respective time point (upper row: patients with CD117-negative tumors). +, Censored patients.
Cancer stem cell antigens and clinico-pathological characteristics.
Cancer stem cell antigens and angiogenic features.
Irrespective of these clinicopathological and technical differences between the studies, those patients who have a high risk of disease-related death will benefit most from prognostic prediction, but also will have a clear profit from adjuvant therapy. Such patients are represented in the stage II/III group that includes, moreover, about 40% of the newly diagnosed NSCLC cases (26). For this patient group, data of Salnikov et al. and our results provide strong evidence that the CSC antigens CD133, BCRP1 and CD117 possess no prognostic significance.
Multivariate analysis.
In contrast to previous studies, we also performed a subgroup analysis of patients with disease relapse who had received radio- and/or chemotherapy after recurrence. Since CSC antigens characterize primarily drug-resistant cells, their expression might rather play a role in the prognosis of radio- and/or chemotherapy-treated patients than in resected individuals (12, 17, 22). In those patients, expression of CD117 tended to be associated with worse survival. The data for CD133 and BCRP1, however, might not have been sufficient for analysis, particularly since the expression of CD133 was associated with a T1 status, but the subgroup study considered only patients with tumors >3 cm. The weak association between CD117 and survival might be a matter of interest for subsequent analyses in larger collectives of radio- and/or chemotherapy-treated patients. Recent in vitro data demonstrated efficient elimination of CD117 positive, drug-resistant NSCLC cells by the c-KIT tyrosine kinase inhibitor imatinib (13).
In this study we used a tissue microarray for immunohistochemical analyses. This reduces technical variability between the samples and allows high throughput-analysis. Nevertheless, it also presents a special challenge to the representativeness of the results, particularly in focally expressed antigens such as BCRP1 and CD133. Recent data on the validation of TMA in lung cancer and mesothelioma demonstrated that 3-4 tissue cores per sample with a diameter of 0.6 mm at least are sufficient to produce reliable results, even for antigens with local variability (p53, Ki 67) (34-36). We used four 1.5 mm tissue cores per sample derived from two different tumor areas (core and invasion front each), and moreover, spotted in duplicates. Additionally, the TMA results of 20 samples were compared to their corresponding tissue sections and showed full concordance. Since CD133 and BCRP1 displayed predominantly focal expression and CD133 was furthermore associated with a T1 status, we additionally assessed corresponding multilevel tissue sections of 20 CD133/BCRP1 negative T2 tumors to exclude a preferential detection of these predominantly focally expressed antigens in small tumors. Except for one case that exhibited a small CD133-positive cell focus in a single tissue section, we found full concordance with the TMA. This indicates an acceptable representativeness of the TMA in the current analysis.
Altogether, this study demonstrated no prognostic significance of the CSC antigens CD133, BCRP1 and CD117 in a collective of 133 Caucasian patients with early-stage NSCLC. In an unselected population, these antigens appear not to be recommendable for the prediction of relapse, DFS or OS after pulmonary resection. The weak association emerging between CD117 and OS in the subgroup of patients with relapse suggests a potential significance of CSC antigens in the prognosis of radio- and/or chemotherapy-treated individuals and might be a matter of interest for subseqent analyses in larger collectives.
Acknowledgements
The Authors thank Mrs. Christa Stolp, at the Tissue Bank and Lung Cancer Registry, Thoraxklinik/University of Heidelberg, and Mrs. Bettina Walter, at the Tissue Bank, National Center for Tumor Diseases, University of Heidelberg, for preparation of tissue samples (C.S.), TMA and immunohistochemical staining (B.W.).
This work was supported in parts by an annual joint grant of the German Cancer Research Center and the Thoraxklinik/University of Heidelberg (S.G.) and by the Tissue Bank of the National Center for Tumor Diseases (NCT), University of Heidelberg.
Footnotes
-
Conflict of Interest
None declared.
- Received October 16, 2011.
- Revision received November 13, 2011.
- Accepted November 15, 2011.
- Copyright© 2011 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- The roles of CD133 expression in the patients with non-small cell lung cancer
- Lack of Prognostic Significance of Neuroendocrine Differentiation and Stem Cell Antigen Co-Expression in Resected Early-stage Non-small Cell Lung Cancer
- Are we Missing the Target? - Cancer Stem Cells and Drug Resistance in Non-small Cell Lung Cancer