


Abstract
Background: Patients suffering from advanced gastric cancer still have a poor prognosis and treatment options are limited. In our previous phase II trial (AGMT-Gastric-1), we showed that the combination of oxaliplatin and irinotecan was well tolerated and effective. The same chemotherapy regimen was now tested in combination with cetuximab in a multicenter phase II trial. Patients and Methods: Oxaliplatin at 85 mg/m2 biweekly and irinotecan at 125 mg/m2 biweekly were combined with cetuximab at 400 mg/m2 loading dose and subsequent weekly infusions of 250 mg/m2. Fifty-one patients with histologically proven unresectable and/or metastatic gastric adenocarcinoma were treated in the first line setting. The median age was 62 years. A single metastatic site was found in 24 patients, 27 patients had multiple metastatic sites. Results: Frequently reported adverse events (in more than 20% of patients) were predominantly grade 1 or 2 and included neutropenia (35%), thrombocytopenia (33%), anemia (73%), nausea (45%), diarrhea (57%), alopecia (22%), and fatigue (37%). Grade 3/4 toxicities included neutropenia in 9/1 patients., thrombocytopenia in 1/0 patients, anemia in 3/1 patients, nausea in 2/0 patients, and diarrhea in 7/2 patients. Sensory neuropathy occurred mostly as grade 1 and 2 in 37% of patients, grade 3 neurotoxicity was observed in 7 patients. Acne-like rash grades 1/2/3/4 were reported in 31%/20%/6%/2% of patients respectively. Thirteen patients discontinued the study due to neutropenia (n=5), nausea/vomiting (n=1), diarrhea (n=1), toxic colon (n=2), and allergic reaction to cetuximab at first (n=2), second (n=1) or third infusion (n=1). Thirty-five patients were assessable for response, with 1 patient (3%) showing a complete response, 21 patients (60%) a partial response, 7 patients (20%) a stable disease, and 6 patients (17%) a progressive disease respectively. The median time to progression was 24.8 weeks, median overall survival was 38.1 weeks. All patients tested had a wild type KRAS status. Conclusion: The combination of oxaliplatin and irinotecan with cetuximab is safe and its action established in advanced gastric cancer.
Chemotherapy in locally advanced or metastatic gastric cancer is still not standardized. A combination of platinum compounds with 5-fluorouracil (5-FU) or an oral 5-FU prodrug is a treatment option widely preferred (1, 2). Triple chemotherapy combinations such as 5-FU/cisplatin/docetaxel or epirubicine/cisplatin/5-FU are one of the most effective treatments but show considerable toxicity (3, 4) and are therefore not considered as a general standard.
In colorectal cancer, it was shown that a biweekly dose of at least 85 mg/m2 of oxaliplatin is superior to a lower dose, and the toxicity of irinotecan is much lower if administered fractionated into two doses. Furthermore an irinotecan dose below the maximum tolerated dose raises concerns about increased toxicity of irinotecan in gastric cancer. In our previous AGMT-Gastric-1 trial (5) the combination of oxaliplatin at 85 mg/m2 biweekly with irinotecan at 125 mg/m2 biweekly was evaluated. Analysis of 40 assessable patients showed that the biweekly outpatient combination of irinotecan with oxaliplatin was generally well tolerated. Frequently reported adverse events (more than 20%) were grade one or two and included neutropenia, thrombocytopenia, anemia, nausea, diarrhea (20% grade one, 7% grade two), alopecia, sensory neuropathy (7% grade two, no grade three) and hand-foot syndrome. Only two patients experienced grade three toxicity (anemia and reversible renal failure). Thirty-eight patients were assessable for response, with a more than 50% tumor reduction in 22 (58%) of them (5). In view of these favorable response rates and the low toxicity profile, we were encouraged to use this regimen in combination with cetuximab.
Cetuximab is a chimeric monoclonal antibody directed against the epidermal growth factor-receptor (6). This receptor plays an important role in mediating proliferation in gastric adenocarcinoma. Its overexpression is found in up to 90% of gastric adenocarcinomas and is correlated with poor prognosis (7-9). Since chemotherapy has only a minor improvement in overall survival there is an unmet need for increasing treatment efficacy. The combination of chemotherapy with a biological agent seems attractive since there is mostly a non-overlapping toxicity and a different biological mode of action. Cetuximab has lead to major response in other gastrointestinal neoplasias (10, 11) and in gastric cancer (11-15).
Patients and Methods
Patient characteristics. From 2007 until 2008, 51 patients with inoperable locally advanced or metastatic, histological proven gastric adenocarcinoma or carcinoma of the gastro-esophageal junction (GEJ) were included. Major inclusion criteria were measurable or evaluable disease, age above 18 years, WHO performance status <3, signed informed consent, no previous palliative chemotherapy and/or immunotherapy, negative pregnancy test for women with childbearing potential, and sufficient hematological renal and hepatic function. Major exclusion criteria included pregnancy or breast-feeding, concomitant antitumoral treatment, prior adjuvant chemotherapy with oxaliplatin and/or irinotecan, prior history of chronic enteropathy, chronic diarrhea, unresolved bowel obstruction/subobstruction, or extensive abdominopelvic radiation therapy, peripheral neuropathy (NCI CTC >grade 1) and other uncontrolled serious non malignant diseases.
DNA extraction and mutation analysis. Paraffin-embedded tissue, either from tumor biopsies or from the resected primary tumors, was used to obtain genomic DNA. In order to ensure that only tumor cells were analyzed, a laser capture microdissection was performed on paraffin sections. Genomic DNA was extracted with QIAamp DNA mini kit following the manufacturer's protocol (Qiagen, Hilden, Germany). The KRAS mutation status was assessed with a quantitative polymerase chain reaction (Q-PCR) applying taqman minor groove binding probes targeting the 7 most common KRAS mutations in exon 12 (n=6) and 13 (n=1) (16). PCR conditions and taqman probes were validated on a set of cell lines harboring a known mutation status. The PCR reagents used and the assay conditions applied were the same as published recently (17). For the PCR reaction and PCR analysis, a Biorad CFX 96 thermal cycler was used (Biorad Life Science Research, Hercules, CA, USA).
Treatment. Oxaliplatin (85 mg/m2) was diluted in 5% dextrose and administered intravenously (i.v.) over two hours. Irinotecan (125 mg/m2) was diluted in 0.9% NaCl and administered i.v. over 30 min. The chemotherapy was repeated every two weeks (1 cycle=4 weeks) until disease progression or unacceptable toxicity for a maximum of six cycles. Dose modification was made according to the protocol. Concomitant medications for treatment of delayed diarrhea (onset >24 hours from the end of irinotecan infusion) were encouraged. The recommended treatment for diarrhea consisted of high doses of loperamide (4 mg for the first intake and then 2 mg every 2 h). Atropine (0.2 mg) was administered prior to irinotecan to prevent acute cholinergic syndrome.
Cetuximab was administered iv before chemotherapy and completed one hour before chemotherapy administration. The first infusion of 400 mg/m2 was administered over 120 minutes. The subsequent doses of 250 mg/m2 administered over 60 minutes were given every 7 days until disease progression or unacceptable toxicity for the maximum of 6 cycles. Pretreatment with an antihistamine was required. Vital signs were checked before, during, and after the end of the infusion. In cases of grade 1/2 rash, topical treatment was considered but cetuximab treatment was not to be changed. In cases of grade 3/4 reactions, cetuximab was to be stopped until toxicity resolved to grade 2 or less. Cetuximab was re-started at the same dose. With the second and third occurrence of grade 3 skin toxicity, cetuximab therapy was delayed for up to two consecutive weeks with concomitant dose reductions to 200 mg/m2 and 150 mg/m2, respectively. In cases of the fourth occurrence of grade 3 skin toxicity despite appropriate dose reduction cetuximab was discontinued. Chemotherapy, however, was continued unchanged as planned. Cetuximab therapy was not withheld for chemotherapy-related toxicities.
Study objectives and evaluation. The primary objective of this multicenter open-labeled phase II trial was to evaluate its safety and feasibility. Secondary objectives were objective-response rates, time to progression (TTP), and overall survival (OS). For this purpose, hematological and non-hematological toxicities were recorded according to the national cancer institute-common toxicity criteria (NCI-CTC) version 1.0. Response was evaluated according to the WHO criteria (18) every 8 weeks in patients with measurable disease.
Results
Patients (n=51) with histologically proven unresectable and/or metastatic gastric adenocarcinoma and no previous palliative chemotherapy or immunotherapy were treated in seven centers. The median age was 62 years (range 19-79 years), male to female ratio was 30 to 21. Twenty-five patients had a performance status (PS) of 0 and 26 patients presented in a PS of 1 or 2. A single metastatic site was observed in 24 patients, 27 patients presented with multiple metastatic sites. Liver metastases were found in 15 patients, lung metastases in 4 patients, lymph node metastases in 16 patients and other metastatic sites in 9 patients. Lactate dehydrogenase was a median of 197 mg/dl (range 122-1756 mg/dl).
Maximum toxicity per patient (51 assessable patients).
Best objective response (35 assessable patients) to combination therapy.
Frequently reported NCI-CTC grade one or two adverse events included neutropenia (35% of patients), thrombo-cytopenia (33%), anemia (73%), nausea (45%), diarrhea (57%), neurotoxicity (37%), fatigue (37%), and alopecia (22%). NCI-CTC grade 3 and 4 toxicities included neutropenia in 20%, anemia in 8%, thrombocytopenia in 2%, nausea in 4%, and diarrhea in 18%. Neurotoxicity grade 3 was observed in 14% of patients (Table I).
Dose intensity was 92.5% for oxaliplatin, 94.7% for irinotecan, and 94.9% for cetuximab respectively.
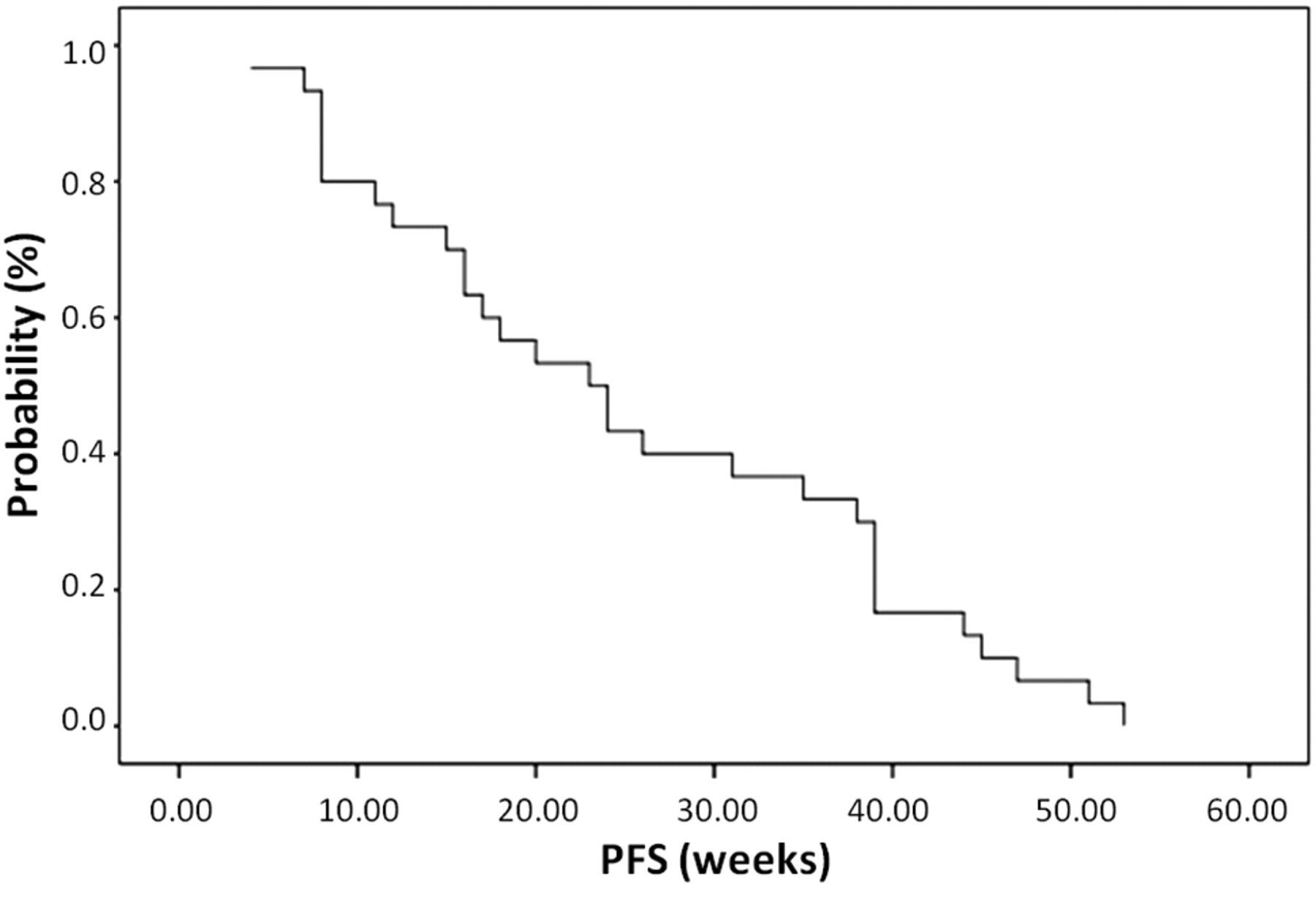
Thirteen patients went off-study due to neutropenia (n=5), nausea/vomiting (n=1), diarrhea (n=1), toxic colon (n=2), and allergic reaction to cetuximab at first (n=2), second (n=1) or third infusion (n=1). Evaluation of response was possible in 35 patients with one (3%) showing a complete remission (CR), and the majority of patients (60%) showing a partial remission (PR) (Table II). Median time to progression (Figure 1) was 24.8 weeks (n=29), median OS (Figure 2) was 38.1 weeks (n=32).
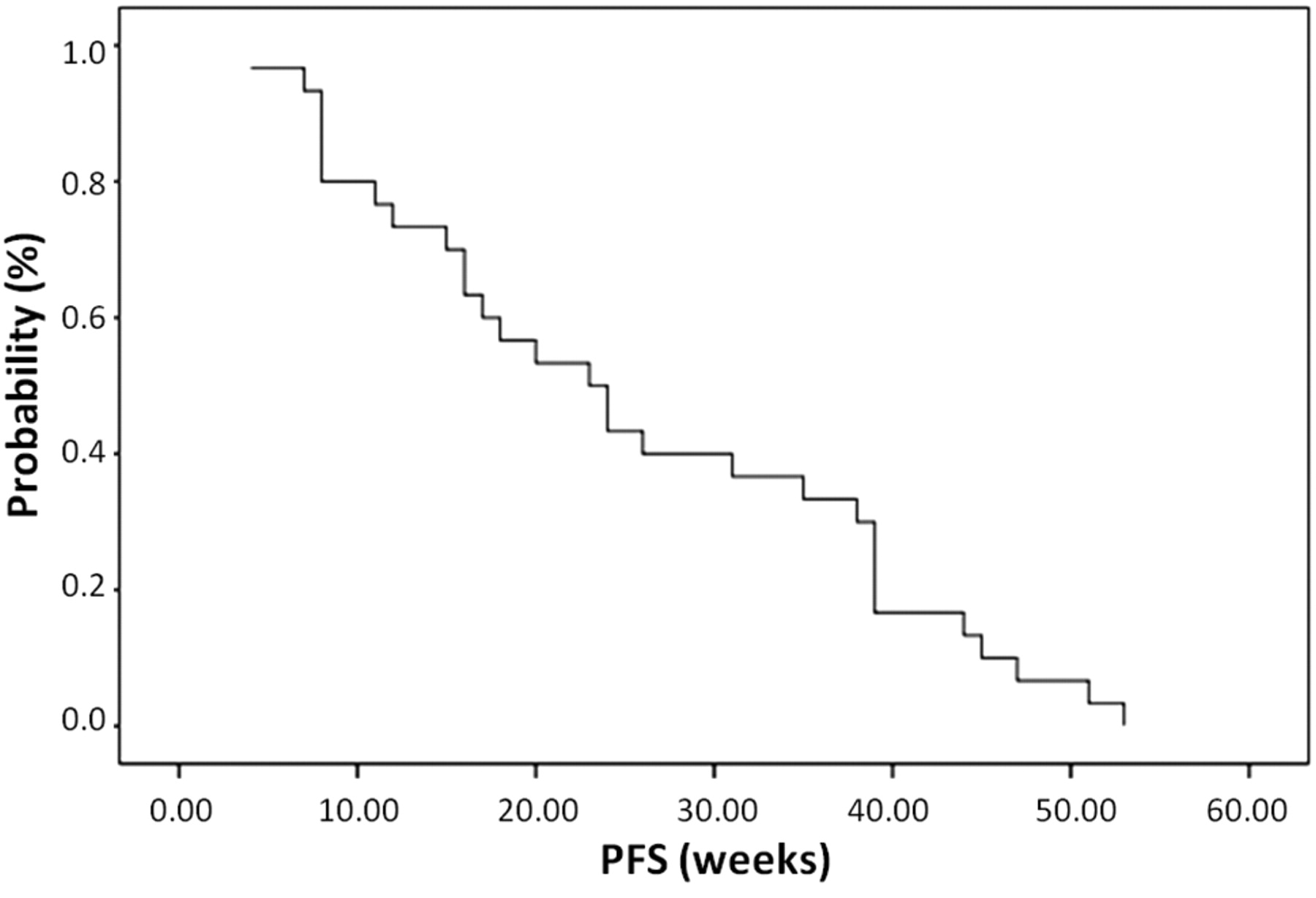
Progression free survival (PFS).

Overall survival (OS).
Grade 1 acne-like rashes were observed in 31% of patients, grade 2 in 20%, grade three in 6% and grade 4 in 2% of patients, respectively. Twenty-one patients developed a rash. Response to chemo/immunotherapy was reported in 86% (18/21) of these patients. Out of 29 patients with response to therapy, 18 patients developed a rash.
A total of 21 patients were evaluable for KRAS mutation analysis. PCR results from eight patients were not included since there was a variation of Ct values equal or greater than 2 for the same sample. For the remaining 13 patients, all patients (100%) had a wild-type KRAS status.
Discussion
Based on the results of our previously performed phase II trial in patients with advanced gastric cancer (5), we chose the biweekly regimen of oxaliplatin (85 mg/m2) and irinotecan (125 mg/m2) as a chemotherapy backbone for the present phase II trial. Due to the low toxicity rate of this outpatient regimen, we considered our protocol an ideal combination partner for cetuximab. In addition, synergistic effects of cetuximab combined with irinotecan are reported (19). Preclinical data also suggest a positive interaction between cetuximab and oxaliplatin (12, 14, 15, 20).
In the present study, the biweekly regimen of oxaliplatin/irinotecan combined with weekly cetuximab was well tolerated, although toxicity was somewhat higher if compared to our historic control. This was also reflected by premature treatment termination of 13 patients due to toxicity. The prophylactic application of steroids in 4 out of the 13 patients would probably have abolished premature termination. Five further patients were withdrawn from the protocol by the investigators due to severe neutropenia. The use of growth factors was not explicitly mandated in this protocol. A more rigorous toxicity management seems to be necessary for the drug combination investigated. Nevertheless, the toxicity of our protocol seems comparable to that of regimens of other phase II trials with cetuximab in gastric cancer (11, 12, 14, 15) and we therefore consider our protocol safe and feasible.
Due to the small number of patients in this phase II trial, the response to cetuximab therapy and skin rash did not correlate significantly. However, a certain trend towards a higher response rate in patients with rash was found.
Retrospective and prospective analyses of KRAS mutational status and response to anti-EGFR antibody treatment in colorectal cancer showed a negative correlation of response in patients with KRAS mutation (21). In gastric cancer patients', however, mutation of KRAS is a very rare event (11, 15). In fact, a PCR analysis for the presence of KRAS mutation status in a subset of our patients showed that all of the patients assayed (13/13) had a wild-type sequence. Other predictive markers are therefore warranted to better detect the population of patients responding to cetuximab treatment. Further translational research is currently being performed on our patient cohort.
The study population showed poor prognostic features, with 51% of the patients presented with a PS of 1 or 2 and all patients had metastatic disease. With respect to these adverse features, a disease control rate (CR+PR+SD) of 83% is encouraging and well in line with other trials investigating cetuximab combinations in first-line treatment of gastric cancer.
In conclusion, the combination of oxaliplatin and irinotecan with cetuximab is safe with an established activity for advanced gastric cancer. Predictive markers to better determine the number of responding patients are necessary for gastric cancer.
Acknowledgements
The Authors acknowledge financial and logistic support of the Verein für Tumorforschung Innsbruck. This work was supported by unrestricted grants from Merck GesmbH, Pfizer Austria and Sanofi Aventis to the AGMT.
Footnotes
-
This article is freely accessible online.
- Received September 15, 2011.
- Revision received November 15, 2011.
- Accepted November 16, 2011.
- Copyright© 2011 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}