


Abstract
Background: This study aimed to evaluate the efficacy of docetaxel plus 5-fluorouracil and cisplatin (DCF) induction chemotherapy for locally advanced borderline-resectable T4 esophageal cancer. Patients and Methods: We retrospectively analyzed data regarding thirty patients with borderline-resectable T4 tumor who received either DCF or cisplatin plus 5-fluorouracil (FP) as induction chemotherapy. Results: The overall response rate was significantly better for the DCF group than the FP group. In the DCF group, 6/16 patients achieved a grade 2 histological post-chemotherapeutic effect after treatment, compared to 1/14 in FP group. Except for myelotoxicity, no other significant differences in toxicity were observed during induction chemotherapy between groups. The DCF regimen did not result in increased postoperative complications compared to the FP regimen. Postoperative recurrence or distant metastasis was observed in 7/10 of FP patients and 5/12 of DCF patients. Conclusion: DCF induction chemotherapy may be an option for conversion therapy of initially unresectable, locally advanced esophageal cancer.
Surgical treatment with three-field lymph node dissection has contributed to improvement in the survival rates of advanced esophageal cancer patients (1, 2). However, analyses of disease recurrence patterns after surgery alone have suggested that surgery alone was insufficient for local control, and have prompted the addition of adjuvant radiotherapy, chemotherapy, or chemoradiotherapy. The introduction of these types of multidisciplinary treatments is thought necessary to improve outcome, especially in advanced esophageal cancer.
Western and Japanese physicians have very different opinions of the roles of chemotherapy and radiotherapy in achieving local control. Based on several clinical trials assessing the effectiveness of neoadjuvant chemoradiotherapy, patients with resectable but advanced squamous cell carcinoma (SCC) of the esophagus usually receive preoperative chemoradiotherapy in Western countries. However, in Japan, there have not been any randomized controlled studies to evaluate the clinical significance of preoperative chemoradiotherapy. After the results of the Japan Clinical Oncology Group (JCOG) 9907 study were reported, neoadjuvant chemotherapy with cisplatin plus 5-fluorouracil (FP) followed by surgery emerged as a new standard treatment for clinical stage II or III esophageal cancer in Japan (3). However, patients with unequivocal T4 disease were excluded from this study, and many Japanese institutions exclude T4 disease as an indication for surgery. In patients with T4 tumors and/or M1 lymph node metastasis, chemoradiotherapy with FP is considered standard treatment (4).
At our institution, we have sometimes seen patients with locally advanced esophageal cancer suspected of invading adjacent organs, but not definitively diagnosed as T4 disease. We called these cases ‘borderline-resectable T4’ cancer. A recent controlled study at an experienced center demonstrated a 2-year survival of around 52% for patients with locally advanced SCC of the esophagus (T3-T4N0-N1) who received neoadjuvant chemoradiotherapy followed by surgery (5), in contrast to the 40% survival for similar patients receiving chemoradiotherapy alone reported in a multicenter trial by Bedenne and co-workers (6). This survival difference suggests that the addition of surgery to chemoradiotherapy for locally advanced SCC can result in improved local control and survival. Therefore, our treatment strategy for such locally advanced cancer includes surgery.
It has been recently reported that patients with SCC of the head and neck who received induction chemotherapy using docetaxel, cisplatin, and 5-fluorouracil (DCF) achieved significantly longer survival than patients who received FP induction chemotherapy (7, 8). DCF chemotherapy also significantly improved overall survival compared with FP in patients with advanced gastric or gastroesophageal adenocarcinoma (9). In addition, it has been reported that a DCF regimen was effective against locally advanced esophageal SCC (10). Therefore, since 2007, we have administered DCF as intensive induction chemotherapy with the aim of curative resection of borderline-resectable T4 tumors. The purpose of this study was to evaluate the efficacy of DCF induction therapy for locally advanced borderline-resectable esophageal cancer by determining the response rates, presence of residual tumor after surgery, histological post-chemotherapeutic effects, safety, and postoperative complications in both FP and DCF regimens. We also investigated postoperative recurrence patterns and survival outcomes.
Patients and Methods
Patients. Data regarding 30 patients with locally advanced borderline-resectable T4 esophageal cancer, at Aichi Cancer Center Hospital between 2001 and 2010, were retrospectively analyzed in this study. Of these, 16 patients received DCF regimen and 14 patients FP regimen as induction chemotherapy, aiming at curative resection. Esophagography, endoscopy, computed tomography (CT) of the chest and abdomen, and/or 18-fluorodeoxyglucose positron-emission tomography (FDG PET)/CT fusion imaging were performed to determine both pretreatment clinical stages and treatment responses. Clinical staging was performed according to the tumor-node-metastasis (TNM) classification of the International Union Against Cancer (UICC), sixth edition (11). A tumor was considered to be borderline resectable T4 if prior induction therapy had not been performed and it also had not been unequivocally determined to be clinical T4. For each patient, the pretreatment tumor depth was estimated, and tumor resectability was determined by the multidisciplinary tumor board of our institution. Written informed consent was obtained from all patients.
Induction chemotherapy. Induction chemotherapy using the FP regimen consisted of intravenous cisplatin (80 mg/m2) on day 1, and a continuous infusion of 5-fluorouracil (800 mg/m2/day) for 5 days, given every 4 weeks for two cycles. The DCF regimen was based on our previous phase II study (12), and consisted of intravenous docetaxel (60-70 mg/m2) and cisplatin (60-70 mg/m2) on day 1, and a continuous infusion of 5-fluorouracil (750-800 mg/m2/day) for 5 days, given every 4 weeks for two cycles. Patients in the DCF group were given prophylactic antibiotics. Granulocyte colony-stimulating factor (G-CSF) was used if patients had grade 4 neutropenia or febrile neutropenia, but was not used for prophylaxis. Hematologic and nonhematologic toxicity was assessed according to National Cancer Institute Common Toxicity Criteria (NCICTC) (version 3.0) and the highest grade occurring anytime during induction chemotherapy was reported. Restaging evaluations were typically performed by CT or FDG-PET/CT fusion imaging 1-2 weeks after the completion of chemotherapy. Because few patients had measurable disease as determined by Response Evaluation Criteria in Solid Tumors (RECIST), the treatment response of each primary esophageal lesion was endoscopically evaluated, and categorized as complete response (CR), partial response (PR), stable disease (SD), or progressive disease (PD) (13). PR was defined as obvious morphological change, such as reduction or flattening of tumor or elevated lesion around the ulcer, along with healing of the ulcer floor. If a clinical response was seen, and curative resection was thus considered possible, the patient was scheduled for surgery 4-6 weeks after the last day of chemotherapy.
Surgical procedure and histopathologic response evaluation. All the patients submitted to surgery underwent a subtotal esophagectomy with regional lymphadenectomy through a right thoracotomy and laparotomy, and reconstruction was performed using the stomach via a retrosternal route with cervical anastomosis through a neck incision. Evaluations of residual tumor (R) were classified as follows: R0, no residual tumor; R1, suspicious of residual tumor or microscopic residual tumor; and R2, macroscopic residual tumor. The entire tumor bed was cut into slices containing the entire esophageal wall, and histological therapeutic effects were classified as follows: grade 3, complete disappearance of viable cancer cells in the tumor bed; grade 2, disappearance of greater than two thirds of viable cancer cells; and grade 1, disappearance of less than two thirds of viable cancer cells (14).
Statistical analysis. The Chi-square test, Fischer exact test, and Student's t-test were used to analyze the relationship between variables, using SYSTAT 12 software (Systat Software Inc., Richmond, CA USA). Progression-free survival (PFS) was calculated from the date of initial chemotherapy until disease relapse, or censored at last follow-up visit. Overall survival (OS) was calculated from the starting date of first-line chemotherapy until death from any cause, or censored at last follow-up visit. Survival data were analyzed using the Kaplan-Meier method. Comparison of survival curves was carried out using a log-rank test. Two-sided p values <0.05 were considered statistically significant.
Results
Patient characteristics. Of 14 patients treated with FP regimen, 7 patients commenced FP therapy between 2001 and 2006, and the remaining patients between 2007 and 2010. All patients treated with DCF regimen commenced therapy between 2007 and 2010. Patient characteristics are presented in Table I. There were no significant differences in age, gender, or performance status (PS) between the FP and DCF patient groups. Most of the primary tumors were located in the thoracic esophagus. N1 and M1 tumors included either regional or nonregional lymph node metastasis, without distant metastasis. The histological diagnosis of all patient tumors was SCC (Table I). In one patient, although the primary lesion was superficial (T1), swelling of the left recurrent nerve lymph node (No. 106recL) was highly suspicious of invasion into the trachea, and the tumor was therefore considered to be unresectable.
Patient characteristics.
Efficacy outcomes. PR was observed in 2/14 and 9/16 of patients treated with FP and DCF, respectively. The overall response rate was significantly better in the patients undergoing DCF than in those receiving FP (10/16 vs. 2/14, p=0.0072).
Of 16 patients treated with the DCF regimen, 4 patients did not go to esophagectomy due to the following reason: upon achievement of CR to DCF therapy in both the primary lesion and lymph nodes, one patient chose subsequent chemoradio-therapy instead of surgery. Subsequent chemoradiotherapy was also performed for another three patients because their clinical response to DCF was insufficient to perform curative resection. Although one male patient treated with DCF achieved PR in the primary lesion, a new lesion occurred in an abdominal lymph node after DCF therapy. Because both the primary lesion and the new lesion in the abdominal lymph node were considered technically resectable, he underwent surgical treatment. Of 14 patients treated with the FP regimen, chemoradiotherapy instead of surgery was chosen by 4 patients because curative resection was not considered possible. Overall, R0 resection was achieved in 10/16 of patients receiving DCF and in 5/14 of patients receiving FP.
Efficacy of induction chemotherapy.
The surgical specimens were serially sectioned and examined microscopically. Histological examination of the primary lesion revealed that 6/16 of patients treated with DCF and 1/14 of patients with FP therapy achieved a grade 2 post-chemotherapeutic effect (Table II, p=0.0499).
Adverse events associated with induction chemotherapy. The worst toxicities seen during the treatment periods are listed in Table III. Grade 3 or 4 neutropenia occurred in 10/16 of patients in the DCF group and in 1/14 of patients in the FP group (p=0.0017). Despite antibiotic prophylaxis, the rate of febrile neutropenia was higher in the DCF group. The percentages of patients with grade 3 or 4 anemia and thrombocytopenia were similar in both groups. Although grade 3 oral mucositis occurred in two patients in the DCF group, there were no major differences in the incidence rates of severe nonhematologic toxicity during induction chemotherapy in the two groups. None of the patients developed treatment-related perforation of the esophageal wall, esophagobronchial fistula, mediastinal fistula, or aortic fistula. There were no treatment-related deaths in either group.
Summary of toxicity during induction chemotherapy.
Postoperative complications. The in-hospital mortality rate after surgery was 0% in both of the treatment groups. The postoperative complication rate was 4/10 in the FP group and 6/12 in the DCF group. Details of the postoperative complications are listed in Table IV. Overall, there were no remarkable differences in the postoperative complications among the two study groups (Table IV). Notably, the incidence of overall infections, including pneumonia, wound infection, and other infections, was similar in the two groups.
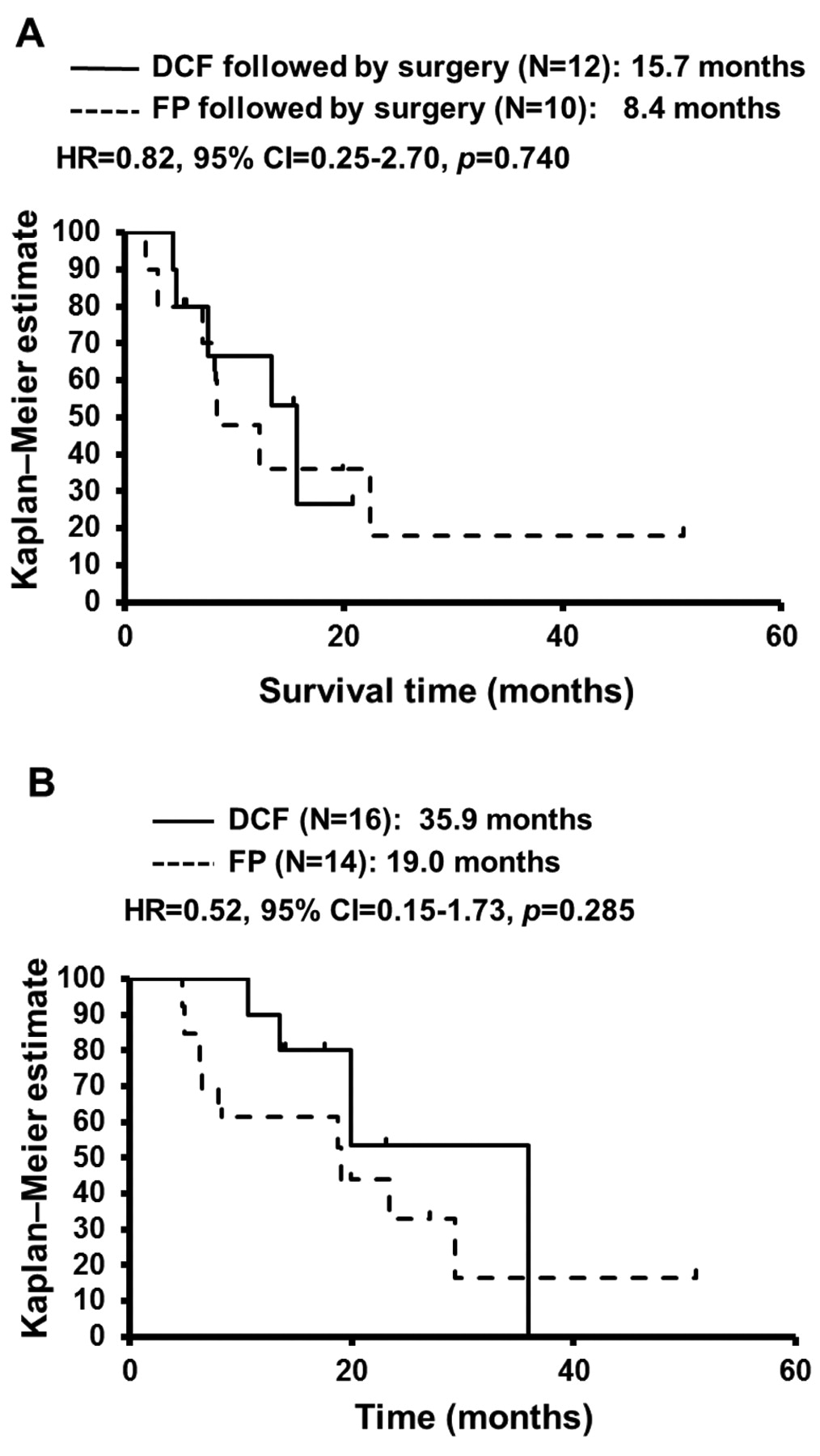
Survival. PFS was analyzed for 22 patients who underwent induction chemotherapy followed by surgery. The median PFS for the DCF group was 15.7 months, which was longer than that for the FP group (8.4 months); however, the difference was not significant (p=0.740; Figure 1A). OS was analyzed for all patients who underwent induction chemotherapy regardless of surgery. The OS for the DCF group was also longer compared to that of the FP group (35.9 months vs. 19.0 months); however, the difference was not significant (p=0.285; Figure 1B). The 1-year survival rate in the DCF group was 90.0%, which was superior to 1-year survival in the FP group (58.3%, Figure 1B).
Postoperative complications.
Patterns of postoperative recurrence. At the time of analysis, the recurrence rates after surgery were 7/10 in the FP group and 5/12 in the DCF group (p=0.1839). There were 7 patients with distant metastases in the FP group. The sites of distant metastases included the bone (N=1), lung (N=2), abdominal lymph node (N=2), and cervical lymph nodes (N=1); and one patient had recurrences in the bone, adrenal gland, and an abdominal lymph node. In another patient, recurrence in an abdominal lymph node was followed by liver metastasis. There were five patients in the DCF group with distant metastasis, and one patient with both locoregional and distant metastasis. The sites of distant metastases included abdominal lymph node (N=1), chest wall (N=1), and muscle (N=1); and, notably, bone metastases (N=5) were observed in all DCF patients who had recurrences.
Discussion
The prognosis of esophageal cancer patients with locally advanced SCC remains poor (15). Because of the high rate of postoperative complications, attention has shifted to neoadjuvant treatment. In the JCOG 9907 study, preoperative chemotherapy with FP was found to be superior to postoperative FP for OS in patients with resectable (non-T4), clinical stage II or III esophageal cancer (3). Based on this result, the standard treatment strategy for unequivocal T3 disease is preoperative chemotherapy with FP followed by radical surgery. However, local recurrence is commonly observed among the patterns of postoperative recurrence in patients receiving preoperative chemotherapy, even after three-field lymphadenectomy. In a meta-analysis of clinical trials of neoadjuvant chemotherapy, Gebski et al. demonstrated that there was no significant preoperative chemotherapy effect on all-cause mortality in patients with SCC (hazard ratio 0.88; p= 0.12) (16). Furthermore, subgroup analysis of the JCOG 9907 study revealed that the survival benefit of neoadjuvant chemotherapy in stage III disease was less than the benefit in stage II disease. Although development of more intensive preoperative therapy is needed for local tumor control of advanced esophageal cancer in order to improve survival, there is no consensus on whether chemotherapy or chemoradiotherapy should be performed as preoperative treatment.
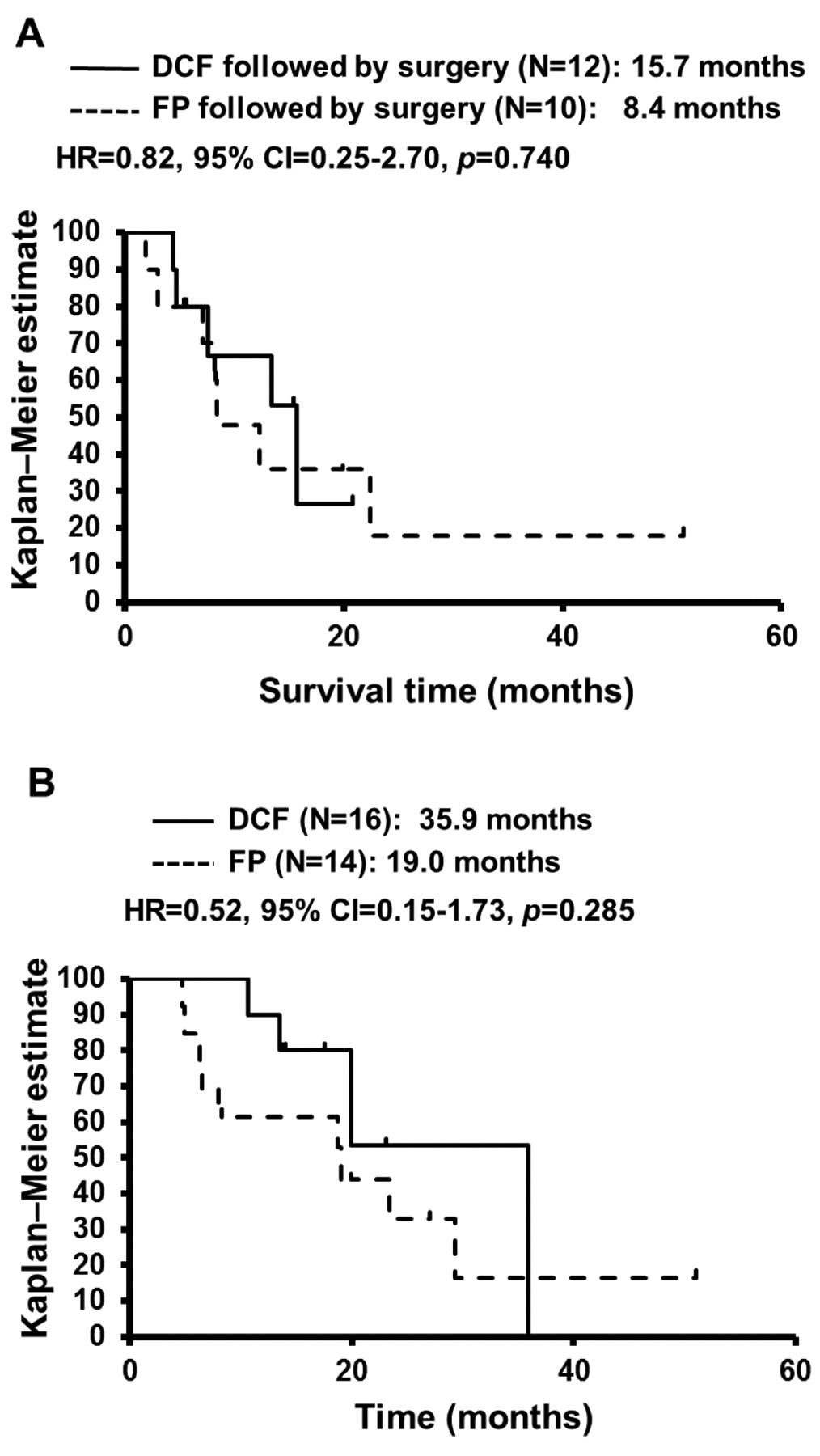
Kaplan-Meier plot showing progression-free survival (A) and overall survival (B) in the docetaxel plus 5-fluorouracil and cisplatin (DCF) and cisplatin plus 5-fluorouracil (FP) induction chemotherapy groups.
Preoperative chemoradiotherapy with FP is expected to be a promising, new standard preoperative therapy for esophageal cancer. Indeed, in Western countries, many patients with stage II or III SCC have received neoadjuvant chemoradiotherapy followed by surgery. Stahl et al. reported that chemoradiotherapy (40 Gy) followed by surgery improves local tumor control in patients with locally advanced esophageal SCC (17). However, treatment-related mortality was significantly increased in the group undergoing chemoradiotherapy followed by surgery compared to the group undergoing chemoradiotherapy alone (12.8% vs. 3.5%, respectively; p=0.03). Thus, there remains concern regarding the potential risks of surgery after chemoradiotherapy. Most randomized controlled studies of neoadjuvant chemoradiotherapy have included surgery alone as the control arm, and these studies failed to demonstrate significant improvement in survival, particularly among patients with histologic subtypes of SCC (18-22).
In this study, we retrospectively investigated if DCF was a more powerful preoperative chemotherapy agent than FP for the treatment of patients with locally advanced esophageal cancer, which were suspected of invading adjacent organs, but were not unequivocal T4 lesions (i.e., borderline-resectable T4 disease). This is a patient subgroup for which we hypothesized that preoperative intensive chemotherapy could contribute to conversion of the lesion to curative resectability, which could lead to improved survival outcomes. Because patients with unequivocal T4 tumors have poor survival outcomes after surgical treatment and are usually treated in the palliative setting with FP or nedaplatin plus 5-fluorouracil with concurrent radiotherapy (4, 23, 24), we excluded unequivocal T4 patients from our analysis. Our results demonstrated that the overall response rate and R0 resection rate were better in patients receiving DCF than in patients receiving FP. One patient treated with DCF achieved complete response.
Histopathological findings in resected specimens revealed more favorable post-chemotherapeutic effects in DCF patients than in FP patients. These findings suggest that DCF induction chemotherapy for advanced esophageal cancer may be a promising preoperative option for local tumor control and may result in a high rate of curative resection. The Medical Research Council Oesophageal Cancer Working Group (MRC) found a 60% R0 resection rate among patients treated with neoadjuvant FP compared with a 54% rate in patients treated with surgery alone, which led to improved overall survival (p<0.0001) (25). Furthermore, it was reported that pathologic response after neoadjuvant therapy is associated with survival in patients with esophageal cancer (26). These findings suggest that pathologic response to neoadjuvant therapy and R0 resection are the major determinants of survival. Our survival analysis indicated that the 1-year survival rate in the DCF group was 90.0%, which is superior to that seen in the FP group, and this DCF result is also superior to survival in patients with unequivocal T4 disease (4). The addition of docetaxel to cisplatin plus 5-fluorouracil may further improve pathologic response and subsequently improve survival in patients with advanced esophageal cancer.
As expected, the DCF regimen induced more leucopenia and neutropenia than FP, but did not lead to more frequent infectious complications. The myelotoxicity seen in the DCF group was consistent with that seen in other studies (7, 8), and was manageable probably because patients received prophylactic antibiotics. No significant differences in nonhematologic toxicity were observed during induction chemotherapy. Furthermore, the DCF regimen did not increase the risk of postoperative complications compared to the FP regimen. This result suggests that esophagectomy after DCF therapy is as safe as after FP therapy.
However, 5/12 patients receiving DCF followed by surgery experienced distant failure within 24 months after surgery. Therefore, we cannot conclude that preoperative DCF chemotherapy is able to provide local tumor control and also to prevent distant failure. Furthermore, the present analysis lacks the statistical power to demonstrate a significant survival benefit of the DCF regimen, because this is a single-institution retrospective study based on a small patient group and short observation period. To achieve better survival after DCF, it may be necessary to determine the predictive factors for tumor recurrence, in order to prevent the occurrence of distant metastasis, as well as to provide locoregional control.
In conclusion, induction chemotherapy using a DCF regimen may be an effective preoperative treatment that allows subsequent curative surgery for locally advanced borderline-resectable T4 esophageal cancer. However, it is still controversial whether preoperative chemotherapy or chemoradiotherapy should be performed. Our observations should be confirmed by longer follow-up and larger sample size. Therapeutic strategies for controlling distant metastasis, as well as locoregional lesions need additional consideration.
Footnotes
-
Conflict of Interest Statement
None declared.
- Received July 13, 2011.
- Revision received August 17, 2011.
- Accepted August 18, 2011.
- Copyright© 2011 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- Strategy Treatment of cT4b Esophageal Squamous Cell Carcinoma Using Docetaxel, Cisplatin, and 5-Fluorouracil
- Neoadjuvant Chemotherapy Versus Chemoradiotherapy for Patients with Esophageal Squamous Cell Carcinoma
- Adverse Prognostic Factors of Advanced Esophageal Cancer in Patients Undergoing Induction Therapy with Docetaxel, Cisplatin and 5-Fluorouracil
- Early Response of Esophageal Cancer to Neoadjuvant Chemotherapy with Docetaxel-Cisplatin-5-Fluorouracil Represents Sensitivity: A Phase II Study