


Abstract
Background: Dermatofibrosarcoma protuberans is an uncommon skin tumour with a low to intermediate-grade of malignancy, characterized by progressive growth and a propensity for local recurrence. Patients and Methods: A retrospective study of a series of 16 consecutive patients with dermatofibrosarcoma protuberans who were treated in the host Institution over the last seven years was performed, with special emphasis on the outcome and disease-free interval, as well as recurrence rate over a mean follow-up period of 43.65 months. Results: The clinicopathological features and results were reviewed. The primary treatment consisted of wide local excision with or without radiotherapy on 13 patients with primary and 3 with recurrent disease, and all patients remained free of disease recurrence during the mean follow-up period. Conclusion: The results of this study and a review of the literature support the notion that aggressive, wide surgical resection with disease-free margins, with or without radiotherapy decreases local recurrences and offers an excellent probability of cure. The accumulated data also confirm that all patients with dermatofibrosarcoma protuberans should be followed up for an extended period, beyond the usual recommended 5-year follow-up, because late recurrences may occur.
Dermatofibrosarcoma protuberans (DFSP) is a rare cutaneous soft tissue sarcoma that was first described by Taylor in 1890 (1, 2), clinically was classified by Darier and Ferrand (3) and later named by Hoffman (4). It is a rare skin tumour that clinically often masquerades as a benign, indolent tumour, but microscopically it extends far beyond assessed clinically margins, and spreads locally in the dermis, subcutaneous tissue and muscles (5). Approximately 85-90% of all DFSPs are low-grade lesions while the rest contain a high grade fibrosarcomatous component and are considered to be intermediate-grade neoplasms (6).
The goal of this retrospective review of 16 patients who underwent wide local excision with or without radiotherapy for the treatment of DFSP tumours was to expand on the clinicopathological characterization and treatment strategy of this unusual neoplasm. Awareness of this entity is important for a prompt diagnosis and a proper management of the disease, preventing both over- and undertreatment of this low to intermediate-grade malignancy.
Materials and Methods
A retrospective chart review was performed on all patients with a history of DFSP who were treated in the host Institution from November 2001 to October 2009. All patients that were still alive were contacted for current performance status. The diagnosis of DFSP was established on 16 patients histopathologically by H&E staining and with positive CD34 immunohistochemical markers. Surgical treatment consisted of wide local excision with at least a 3-cm margin, including the underlying fascia. Adjuvant radiation therapy was given to patients with large lesions or close margins after maximal resection. The details of the radiation therapy were not analysed. A review of the medical records provided information on demographics (age, sex), tumour characteristics (location, size), treatment course, evolution (location and time of recurrence) and length of follow-up.
Results
From November 2001 to October 2009, 16 patients were diagnosed with DFSP.
A summary of the clinical data is presented in Table I. The mean patient age at time of diagnosis was 41.12 years (range, 21-59 years). Preoperative duration of symptoms was described by all patients to be long (more than 1 year). Sex distribution (9 females, 7 males) was approximately equal. The anatomical location of the tumour was on the trunk and proximal extremities in 9, on the lower extremity (Figures 1 and 2) in 2 and on the head and neck in 5. Tumour size ranged from 1 to 22.5 cm (median 3.32 cm). The majority presented clinically as a raised slowly growing firm, nodular dermal/subcutaneous mass. The median follow-up in this series was 43.65 months.
Clinical data.
A history of resection and subsequent local recurrence was found in 3 patients and all were associated with positive or very close initial surgical margins. No case gave rise to metastatic disease. Treatment in all cases was wide local excision with disease-free margins of at least 2.5 cm.
Reconstruction of the defects took place primarily in 9 cases and with split-thickness skin grafts in three patients. One patient underwent reconstruction with a pedicled Latissimus dorsi flap, while one another with a pedicled trapezius flap. In addition, a free radial forearm flap was used as a reconstructive surgical procedure in two patients. Adjuvant radiotherapy was provided in two cases with local recurrence and in one case of massively extended disease.
Discussion
DFSP is a rare, low- to intermediate-grade mesenchymal malignant neoplasm that originates from the dermis, from which it often invades the subcutaneous tissue (7, 8), and accounts for 1% to 2% of all soft tissue sarcomas (9, 10). DFSP is characterized by an indolent, very slow but infiltrative growth pattern and in many cases its symptoms are long lasting, up to 30 years according to Lindner et al. (11). Preceding traumas are mentioned in 10-20% of cases and some tumours are found in burn and surgical scars (12). DFSPs arise as pink or violet-red plaques, while the surrounding skin may be telangiectatic (13, 14). They typically do not exhibit a nodular growth pattern until late in their course (15). Small lesions are mobile but as they enlarge they become fixed because of infiltration of the underlying fascia (13, 14). Clinically, the largest diameter in the majority of DFSPs measures less than 5 cm. The plaque stage may clinically cause confusion with scar tissue or sclerosing dermatoses such as morphea or scleroderma (16). Intermediate lesions can be confused with larger dermatofibromas while advanced lesions must be differentiated from malignant fibrous histiocytoma and fibrosarcoma (17).
DFSP typically arises on the trunk of the body and proximal extremities, followed by the distal extremities, and then head and neck with a slight male predomination (18). It usually presents in the fourth decade of life, although the age of appearance varies widely (19, 20). In the current series, the tumours had a similar age distribution to typical DFSP, with a slight female preponderance. The most common sites of presentation for DFSP in the current series were the trunk, followed by the head and neck and then extremities, but these apparent differences may reflect sampling error in this relatively small case series.
Uncommon variants of DFSP include the Bednar tumour (pigmented DFSP), myxoid, atrophic, fibrosarcomatoid, mixed granular cell and sclerosing. A congenital variant has also been described with characteristic histological markers (7, 21, 22).
Case 8, DFSP on the back with multinodular protuberant ‘phenotype’.

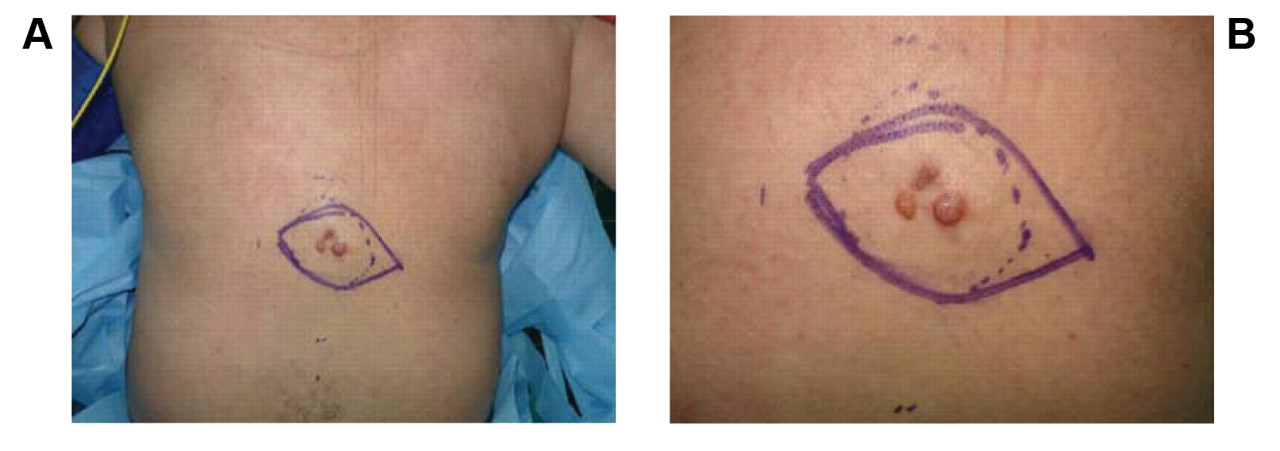
A: Case, 16 DFSP on the thigh with nodular appearance. B: Case 7, DFSP on the anterior thoracic wall with plaque-like appearance.

A: The tumor was stained positively for CD34 (×400). B: Storiform pattern infiltrating between adnexal structures. Fat is also involved by tumor cells (HE,×100).
Histologically DFSP is composed of monomorphous spindle-shaped cells arranged in a storiform pattern on a background of fibrous stroma. A honeycomb pattern of infiltration into the subcutaneous fat is also seen, while mitoses are rare, explaining the low grade malignant behavior of the tumour (6, 23). DFSP is strongly positive to staining with CD34. It is also immunoreactive to vimentin. On the contrary, it shows a light or absent reaction to CD44, which represents a useful marker for the differential diagnosis from dermatofibroma. Distinctive histological features of DFSP, as well as findings consistent with the immunohistochemichal profile of typical DFSP were present in all the cases in this series (Figure 3).
More than 90% of DFSP are characterized by a reciprocal chromosomal translocation, t(17;22)(q22;q13), or more frequently, a supernumerary ring chromosome composed of hybrid material derived from t(17;22). This rearrangement leads to constitutive activation of the platelet-derived growth factor as a result of deregulated ligand expression (24).
The main feature of DFSP is the horizontal spread of the tumour by creating neoplastic projections to all directions, like pseudopodia, resulting in the ejection of neoplastic cells up to 3 cm peripherally to the main tumour. This histological behaviour results in the high recurrence rate, as a result of satellite neoplastic cell populations that may be left in situ, during resection (13, 25).
According to Gayner et al. (26), excisional microscopic negative border less than 2 cm represents the main predisposing factor of recurrence. Bowne et al. (25) established as negative prognostic factors for recurrence of DFSP the age older than 50 years, resection close to positive microscopic margins, fibrosarcomatous variant, high mitotic rates and increased cellularity. In addition, it is also well accepted that the number of recurrences up to the last excision represents a negative prognostic factor for the possibility of future recurrence.
DFSP has a tendency for local recurrence of up to 25% and most recurrences tend to develop within 3 years, after resection. Late recurrences, even after 15 years, have been also reported (18, 27, 28). Metastasis may occur through the bloodstream to the lungs or less commonly via the lymphatics to regional lymph nodes (29, 30). Recent study by Fiore et al. (15) confirms that most cases of DFSP, including recurrent disease, can be managed with wide-excision surgery, providing a crude incidence of recurrence in the entire population 3% at 5 years and 4.2% at 10 years and a crude incidence of distant metastasis of 1.7% at both 5 and 10 years. The prognosis of DFSP is generally excellent if completely excised with clear margins (15).
In the current series, no patient relapsed within the mean follow-up time of 43.65 months. On the other hand however, in 2 cases there was a history of excision and recurrence after more than 10 years.
Excision of DFSP is usually performed at the stage of solitary nodulous growth. Because of its harmless general appearance, an inadequate excision of microscopic extensions which are located lateral to the tumour or deeper than it, may take place (12). The pattern of growth which is primarily lateral or radial spread may become deep or vertical in longstanding or recurrent tumours. The first resection is of major importance, since tumour spread after an inadequate first resection may lead to uncontrollable local growth (10).
Most authors suggest a margin of 2.5 to 3 cm of normal tissue from the gross tumour boundary, with a three-dimensional resection (en bloc removal) that includes skin, subcutaneous tissue and the underlying investing fascia, achieving negative microscopic margins (15, 31, 32). An alternative option represents Mohs micrographic surgery, designed for tumours with extensive subclinical skin involvement. Recurrence rates with this surgical potentially tissue-sparing option of 0% to 6.6% have been reported in several series (5, 19, 30). DuBay et al. (20) introduced a multidisciplinary combination approach with DFSP as an efficacious treatment strategy, in order to optimize patient care.
DFSP is considered to be a radiosensitive tumour. Consequently, radiation therapy can be recommended as adjuvant therapy in cases with positive margins or close margins after maximal resection, in case of a large lesion excised with negative margins, in case of recurrent lesion or in case that achievement of wide margins would result in a functional or cosmetic deficit (1, 24, 33).
Recently, imatinib a potent selective inhibitor of the platelet-derived growth factor receptor has been reported to induce complete or partial remissions in most patients with advanced DFSP, and is approved for treatment of adult patients with unresectable, recurrent and/or metastatic DFSP who are not eligible for surgery (34).
In summary, DFSP is a distinct oncological entity which often presents a diagnostic challenge. The proper identification and diagnosis is clinically important. The cornerstone of DFSP management consists of complete surgical resection with negative margins (26). The Authors' experience recommends as a frontline treatment wide excision of the tumour with at least 5 cm of surrounding tissue, extending deeply to histopathological disease-free anatomic tissue, in order to improve prognosis over time. In addition, the authors recommend close follow-up for cancer surveillance for an extended period, as late recurrences may occur.
- Received April 20, 2010.
- Revision received May 22, 2010.
- Accepted May 28, 2010.
- Copyright© 2010 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}