


Abstract
The objective of this study was to evaluate the expression of MMP-2 and MMP-9 in sentinel lymph node and serum of breast cancer patients in order to evaluate their clinical significance and usefulness as diagnostic tumour markers. Expression of MMP-2 and MMP-9 was performed on sentinel lymph node by immunohistochemistry while gelatine zymography was used to determinate the serum expression. The association of gelatinases with clinicopathological features, were analysed. Metastatic and non-metastatic breast cancer patients and 34 healthy women were involved. Gelatinases expression were significantly higher in metastatic breast cancer in comparison to non-metastatic cancer and the control group both in the sentinel lymph node and serum. Results showed a statistically significant correlation between MMP-2 or MMP-9 and cancer familiality, MMP-9 and CA 15.3 levels, and MMP-9 and grading. This study suggests a clinical utility of these proteolytic markers in malignant tumour, growth, invasion and metastasis in breast cancer.
Breast cancer is the most common cancer affecting women in the world today. It is the leading cause of cancer-related death for women aged between 35 and 65 years worldwide. One in nine women will suffer from breast cancer during their life and in excess of 130,000 women die from breast cancer each year (1, 2).
Tumour cells have the ability to ‘move’ within the organism which they have colonised and give rise to metastases. Cancer cells can break away from the original tumour through the lymphatic system or through the blood circulatory system. The first case gives rise to lymph node metastasis, while the second case causes distant metastasis in various organs, depending on the type and site of origin of the primary tumour (3).
Distant metastases are the principal cause of death. An essential process in forming metastases is the degradation of the extracellular matrix (ECM), allowing the tumour to invade the local tissue, intravasate and extravasate the blood vessels and create new metastatic formations (4).
Lymphatic cancer cells follow the principle of sequential progression, that is, they arrive at the node nearest the tumour site and from there they invade the neighbouring lymph nodes.
The sentinel node is the first lymph node affected by metastatic cells since it is the first one receiving lymphatic drainage from the tumour. Based on the principle of sequential progression of tumour cells in lymph vessels, if the sentinel node is free of metastases it is likely that none of the lymph node compartment has been affected by the tumour (5).
Several studies have demonstrated an important role of enzymes such as matrix metalloproteinases (MMPs) in the degradation of ECM and of the components of its basement membrane (BM), facilitating the detachment of tumour cells, their crossing of tissue boundaries and their invasion into adjacent tissue compartments (6). Degradation of the connective tissue stroma and invasion of the BM are key elements in tumour invasion and metastasis. The degradation of ECM components is executed by proteolytic enzymes of various classes (7)
MMPs are a family of 23 structurally related zinc-dependent endopeptidases involved in various physiological processes such as embryogenesis, reproduction, uterine involution and angiogenesis; however several studies have reported up-regulation in the course of various malignancies including breast, colon, pancreatic and liver cancer (8-10).
In breast cancer, two MMPs, namely the 72 kDa type IV collagen (MMP-2 or gelatinase A) and 92 kDa type IV collagen (MMP-9 or gelatinase B), are particularly implicated in the process of metastasis (11, 12)
Gelatinase A and B differ from other MMPs because they have three tandem fibronectin type II repeat sequences that are thought to confer gelatin-binding properties within the amino terminus of the catalytic module that mediates gelatine binding (13). These gelatinases are secreted as latent and inactive pro-enzymes which are activated by the proteolytic cleavage and are specifically inhibited by forming a complex with a class of endogenous inhibitors termed tissue inhibitor of metalloproteinases (TIMP) or by non-specific protease inhibitors such as α2-macroglobulin. Currently four different TIMPs are known to exist: TIMP-1, -2, -3 and -4. The stoichiometric ratio between the two types of molecules is physiologically 1:1 (14).
MMP-2 and MMP-9 have been extensively studied as possible tumour markers and predictive factors of metastasis in breast cancer patients and their increased expression in the primary tumour is associated with aggressive disease and unfavourable outcome (15).
The major objective of this study was to investigate the expression of both gelatinases in the sentinel lymph node and the serum of patients affected by metastatic or non-metastatic breast cancer and to analyse the association of these markers with others parameter such as tumour size (T), lymph node involvement (N), metastasis (M), grade of differentiation (G), HER-2/Neu, oestrogen and progesterone receptor status (ER and PgR, respectively), cancer familiarity and menopausal status in order to evaluate their clinical usefulness as diagnostic tumour markers in breast cancer.
Materials and Methods
Fifty patients with metastatic and non-metastatic breast cancer undergoing mastectomy or quadrantectomy surgery at ‘Giovanni Paolo II’ National Cancer Institute of Bari, Italy, were enrolled between 2004 and 2007. A control group comprised 34 healthy women who were asked to consent to participate in the study.
All the data obtained from medical records, after informed consent of the patients enrolled was given, were included in a database developed in Microsoft Excel (Microsoft Corp, WA, USA). Cytological and histopathological parameters considered were the following: histological diagnosis of cancer, menopausal status, cancer family, TNM, G, ER and PgR status), MIB-1, expression of HER-2/Neu and type of therapy.
The expression of gelatinase A and B in paraffin-embedded sentinel lymph nodes was evaluated using immunohistochemistry, while the serum concentrations of MMP-2 and MMP-9 were tested using zymography.
Identification of sentinel lymph nodes by perilesional lymphoscintigraphy. Colloidal particles of human albumin, measuring between 20 and 80 nanometers (Nanocol) labeled with 99mTc were used. The day before surgery for mastectomy or quadrantectomy, the solution containing the radioactive tracer (0.2 mCi 99 mTc in a volume of 0.2-0.4 saline) was inoculated with 25 G needle by injection under the skin at the breast lesion for 4 times. The patient was asked to massage the area of inoculation for several minutes in order to speed up the lymphatic drainage. Subsequently, dynamic lymphoscintigraphy was performed by gamma camera (Siemens Diacam. LabInstruments Inc., India). Scintigraphic images were acquired for about 10-20 minutes until the identification of the route of lymphatic drainage duct and its sentinel node. The anterior oblique projection at 45°C is optimal because it allows the injection site to be better distinguished from the axillary sentinel lymph node. The place of accumulation corresponding to LS was marked with a dermographic pen.
Expression of gelatinase A and B in lymph nodes by immunohistochemistry. All lymph nodes were dissected clearly and fixed in formalin. The sentinel lymph node was bisected along its major axis and embedded in paraffin. For each paraffin block obtained, 40 pairs of sections, each 4 μm-thick, were cut at 50 μm intervals. If residual tissue was left, an additional pair of sections was cut at 100 μm intervals until the lymph node had been sampled completely. One section of each pair was stained with haematoxylin and eosin. If the result of the staining was ambiguous, the parallel section was stained for cytokeratin.
Immunostaining for MMP-2 and MMP-9 was performed on the formalin-fixed tissue sections. Sections were deparaffinised and heated in a microwave oven for 10 min for unmasking using an antigen retrieval protocol (Benchmark XT; Ventana). (Medical System Inc., Tucson, Arizona, USA).
Sections were immersed in 3% hydrogen peroxide in 100% methanol for 10 min to block the endogenous peroxidase activity. All sections were incubated with primary antibody MMP-2 (clone 75-7F7 mouse monoclonal antibody; Calbiochem-Darmstadt Germany; 1:100) and MMP-9 (clone 56-2A4 monoclonal antibody; Calbiochem; 1:100) for 60 min at room temperature. Subsequently the sections were incubated with biotinylated anti-mouse (i-View DAB Detection Kit; Ventana) for 20 min and treated with peroxidase4-conjugated streptavidin for 20 min (i-View DAB Detection Kit).
The sections were then immersed into 3-amino-9-ethyl-carbazole (AEC, Tucson, AZ, USA) solution. The slides were counterstained with haematoxylin solution, dehydrated and mounted.
Between steps, the slides were washed three times with phosphate-buffered saline (PBS). PBS was used as a negative control instead of the primary antibody.
Hormone receptor expression (IHC). ER and PgR assays were performed with primary monoclonal antibodies to the receptors (anti-human oestrogen receptor α1D5; Dako Diagnostics, Denmark, and anti-human progesterone receptor 1A6; YLEM s.r.l, Rome, Italy). Cases of intraductal infiltrating carcinoma (IDC) with known reactivity for the antibody were used as positive controls. Sections 4-6 μm-thick obtained from the paraffin-embedded tissues were placed on slides, pretreated with endogeneous peroxidase and blocked with hydrogen peroxide. Then antigen retrieval was performed using a microwave at 650 W for 3 cycles of 8 minutes each and citrate buffer 1×, 0.07 M, pH 6±1. Subsequently, the slides were incubated, firstly with streptavidin-biotinylated ABC (StreptABComplex) overnight at 4°C, and then with amino-ethyl-carbazole (AEC) as chromogen. Slides were examined under light microscopy. The results were recorded as the percentage of positively stained target cells with positive samples being defined as those showing more than 10% stained tumour cell nuclei.
HER–2/Neu expression (immunohistochemistry). HER-2/Neu immunostaining was performed on 3-4 μm-thick sections obtained from the paraffin-embedded tissues, using the polyclonal antibodies A0485 (Hercept Test, Dako Diagnostics) directed against the C-terminal fragment of the molecule (intra-domain) and diaminobenzidine tetrahydrochloride (DAB) as chromogen. Avidin-biotin peroxidase complex was used as standard. Cases of IDC with known reactivity for the antibody were used as positive controls. Negative control reactions were performed omitting the antibody. Using light microscopy, breast carcinoma cells that showed intense membrane staining were considered to be positive, while those that showed cytoplasmic staining in the absence of membrane staining were skipped.
Membrane immunoreactivity and staining patterns were evaluated and scored using a scale of 0 to +3 according to the scoring system outlined in Dako's Hercept Test manual. The first step in the scoring system was to ascertain whether more than 10% of the tumour cells had complete membrane positivity and, finally, the staining intensity was graded with 1 if membrane staining was absent or very weak intensity, with 2, if the membrane staining intensity was weak, or with +3, if the membrane staining intensity was strong.
Gelatinolytic zymography assay. Gelatinolytic zymography was performed as previously described (16). Briefly, patients' sera were analysed for gelatin degradation activity by 8% SDS-PAGE containing 5.8 mg/ml gelatin under non-reducing conditions. Electrophoresis was performed and, after a brief wash with water, SDS was removed from the gel by incubation with 2% Triton X-100/PBS solution. Gelatinolytic activities were developed in a buffer containing 5 mM CaCl2, 150 mM NaCl, and 50 mM Tris at 37°C for 16 h and then visualised by staining the gel with Coomassie Blue R-250. The amounts of MMP-2 and MMP-9 were quantified using scanning densitometry with an image analysis software (Image Master ID Prime; Pharmacia Biotech, UK) (16).
Statistical analyses. The data were analysed using the unpaired Student's t-test and the MannWhitney U-test. The frequency distribution of MMP-2 and MMP-9 in lymph node and serum were assessed using univariate ANOVA. Pearson's correlation analysis was performed between the two MMPs. All statistical analyses were performed by SPSS for Windows v. 9.01 (SPSS Inc., Chicago, IL, USA). Numerical data are expressed as mean±standard deviation (SD). P-values≤0.05 were considered to be statistically significant.
Results
The analysis focused on 50 patients with metastatic and non-metastatic breast carcinomas aged between 24 and 92 years (51.5±16.3 years; median 51 years) and 34 healthy women aged between 35 and 59 years (45±6.5; median 44 years). The clinicopathological characteristics of the breast cancer patients are listed in Table I.
Breast cancer patient and tumour characteristics.
Correlation between MMP-2 expression and metastatic (micro- and macro-metastasis) sentinel lymph nodes.
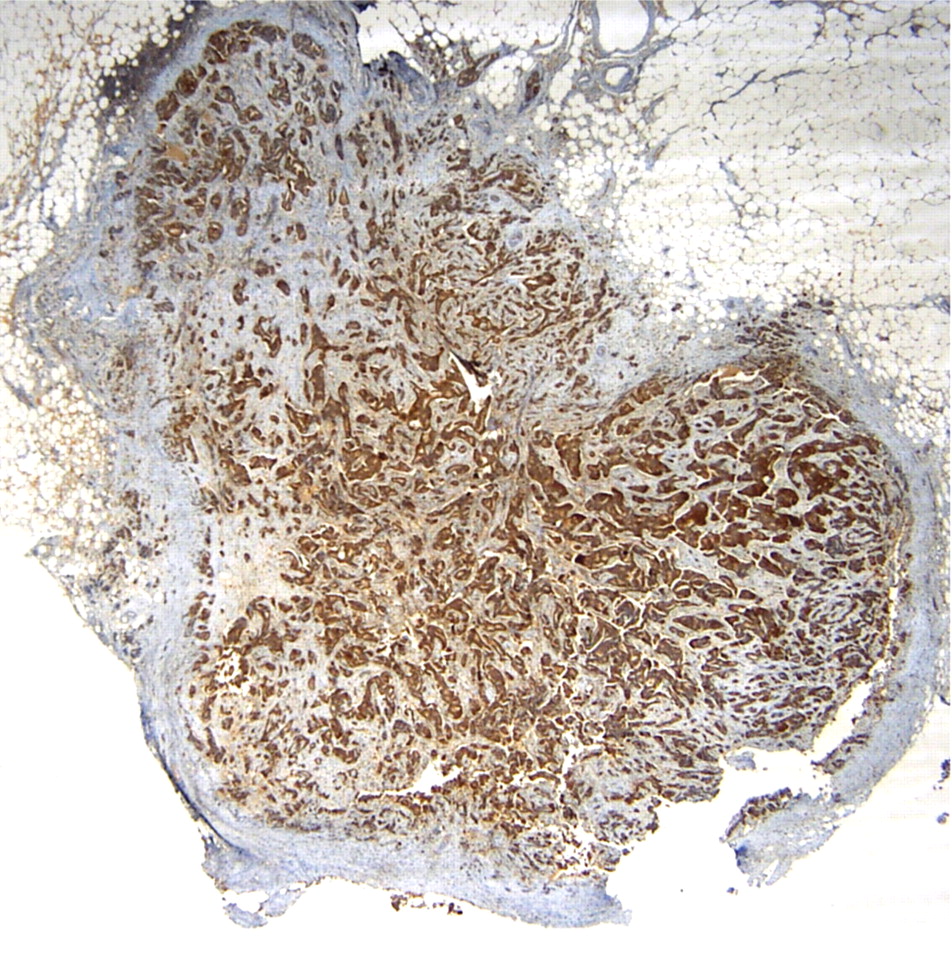
Among the 50 cases, 30 sentinel lymph nodes were non-metastatic and 20 were metastatic. Among the metastatic cases, 5 presented micrometastases (<0.2-2 mm) and 15 macrometastases (>2 mm), as shown in Table II. The immunoexpression for both gelatinases was negative in the non-metastatic sentinel lymph nodes and in the micrometastases (score − − −) while a strong positivity was highlighted in the macrometastases. This resulted in a statistically significant correlation between gelatinase expression in micro- and macrometastasis by the t-test (p<0.01). In the subgroup of macrometastasis, MMP-2 was negative in only 1 case (score − − −), slightly expressed in 5 cases (score ++−) and intensely expressed in 9 cases (score +++) (Figure 1). MMP-9 was negative in only 4 cases; all the samples in which there was strong expression of MMP-2 positivity there was also strong intensity for MMP-9 (data not shown). The immunoexpression of both MMPs was also assessed in 10 sentinel lymph nodes N0, used as negative control, which showed a modest cytoplasmic positivity in the histiocytes of the breast tissue only.
Correlation between serum levels of MMP-2 and MMP-9 and clinicopathological characteristics of breast carcinoma. P-values ≤ 0.05 were considered to be statistically significant. n.s: Not statistically significant.
Concerning the MMP-2 and MMP-9 serum expression performed by zymography, analysis of the results showed higher concentrations of MMP-2 and MMP-9 in patients diagnosed with or without metastatic breast cancer compared to the group of healthy women.
Specifically, the mean serum MMP-2 concentration was 8333±2982 b.i. (median: 8217 b.i) in patients with breast cancer, while it was 5950±1222 b.i. (median: 5867 b.i.) in the control group. This difference was statistically significant (p<0.01).

Sentinel lymph node with massive metastases of ductal breast carcinoma. Strong cytoplasmic immunostaining for MMP-2 (×5).

Scatter plot of the concentrations of gelatinase A (axis Y) and B (axis X) from preoperative serum (unit: b.i) of the 50 patients examined. The line represents the the two gelatinases are independent variables.
MMP-9 had higher concentration levels in patients with breast cancer (3519±2045 b.i., median 3135 b.i.) than in healthy volunteers (3340±1980 b.i., median 2975 b.i). Also in this case the difference was statistically significant (p=0.05).
In the subgroup of 20 patients with micro- or macro-metastatic sentinel lymph nodes, the serum expression of MMP-2 was higher than in the subgroup of 30 patients with non-metastatic sentinel lymph nodes (8974 b.i. vs. 6542 b.i., respectively;); however, the difference between these two groups was not statistically significant. The serum levels of both gelatinases were then analysed for correlation showing that correlation with a number of clinicopathological and biochemical parameters including tumour size, grade, the presence of positive lymph nodes, ER and PgR status, HER-2/Neu CA 15.3 levels, familiality of cancer and menopausal status as shown in Table III.
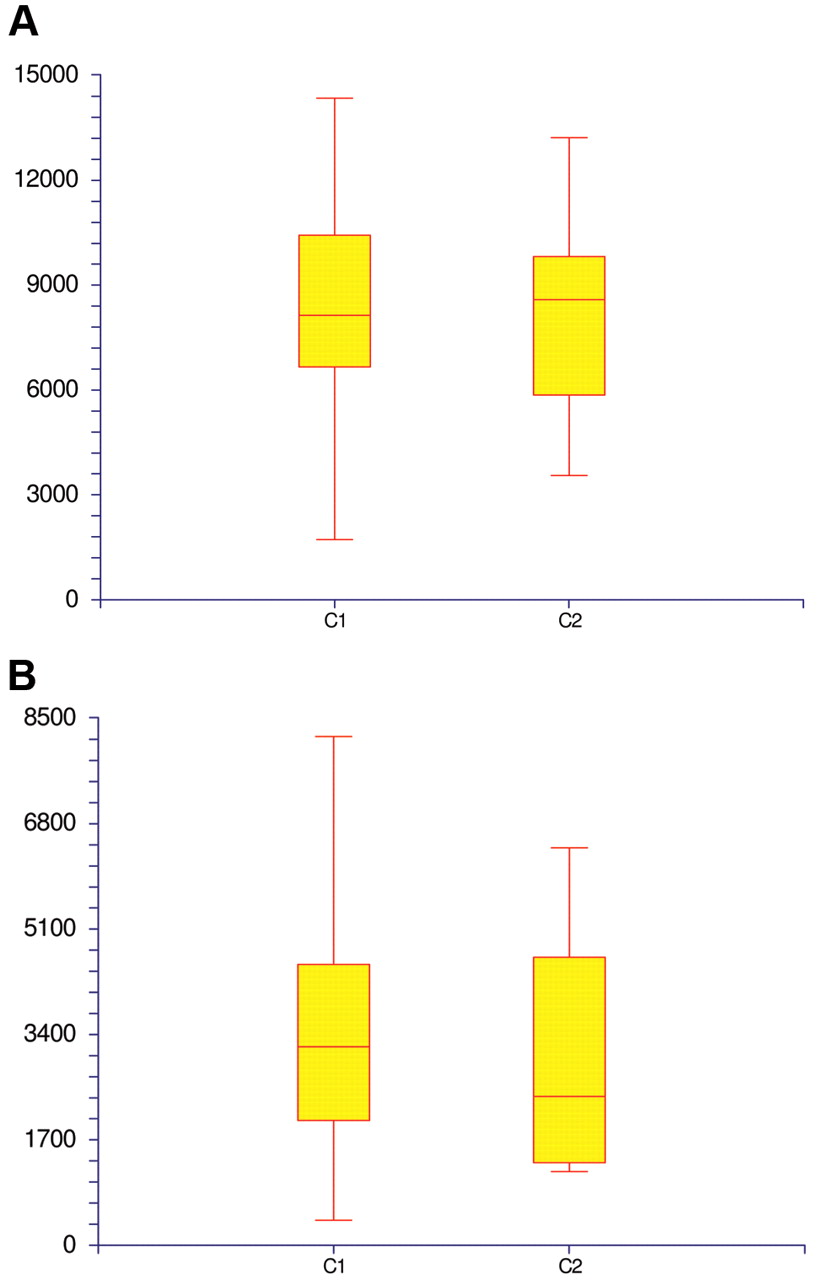
A: Univariate ANOVA: Frequency distribution of sentinel lymph node (SL) expression of MMP-2 (score 0, +3)(x) and preoperative serum MMP-2 levels (y) (median: 8217 b.i.) in 50 breast cancer patients. C1: negative SL; C2: positive SL. B: Frequency distribution of SL expression of MMP-9 (score 0, +3)(x) and preoperative serum MMP-9 levels (median: 3135 b.i) (y) in 50 breast cancer patients. C1: negative SL; C2: positive SL.
The t-test showed that the serum concentration of MMP-9 was higher in breast cancer patients with G3 than in those with G2 or G1 disease, with a direct significant correlation (p=0.05). A direct correlation was observed between the high serum levels of MMP-9 and CA 15.3 (p=0.01). A statistically significant correlation between MMP-2 and MMP-9 serum levels and oncology familiality was also found (p=0.04 and p=0.02, respectively). No correlation, instead, was found between serum and tissue expression of either gelatinase and the remaining clinicopathological parameters considered.
In addition, the Pearson's correlation analysis showed that MMP-2 and MMP-9 are two independent variables (Figure 2).
Finally, Figures 3 (part A and part B), show the frequency distribution between the MMP-2 and MMP-9 expressions in sentinel lymph nodes and the serum of the 50 breast cancer patients, using univariate ANOVA.
Discussion
Animal tissues are formed by cells and the ECM where proteins, polysaccharides and fibrotic components are present in various proportions (17). The role of ECM is to maintain the adhesion between cells and, through adhesion receptors, to transmit signals. ECM components are the interstitial matrix and the basement membrane (18).
It has been observed that the ECM of a tumour and the stromal cells within the tumour play an important role in tumour progression (19). Among the various proteolytic enzymes present in human tissues and associated with tumour invasion, metalloproteinase family members are of prime importance because of their ability to degrade all the components of interstitial and basement membrane material allowing the cells to penetrate and infiltrate tissues surrounding.
In particular, MMPs have long attracted research interest due to their possible use as molecular markers and therapeutic targets (4). In the present study, gelatinase A and B expression was observed in the sera and the sentinel lymph nodes of breast cancer patients. The sentinel lymph node is the first to receive lymphatic drainage from a particular area of an organ and therefore it is the first to receive metastatic deposits from a tumour (20, 21).
Regarding this observation, we wished assessed the expression of two gelatinases in both the sentinel node and in the serum of patients with breast cancer, finding that in both cases there is an overexpression compared to healthy controls). These data are important considering two aspects. The first one is diagnostic or prognostic, since these markers, as demonstrated by several authors, could be used both to diagnose breast cancer early, of course confirmed by other imaging examinations such as ultrasound, mammography, mammotome, or in prognosis of disease progression and metastasis. The second aspect is clinical, because the overexpression of MMP-2 and MMP-9 in the sentinel lymph node may predict axillary lymph node involvement and thus avoid their surgical removal, ensuring a good quality of life for the patient after intervention by eliminating the related symptoms (pain, swelling, difficulty using the limb).
The results of the present study showed higher levels of both gelatinases in macrometastatic sentinel lymph nodes with respect to micrometastatic and non-metastatic lymph nodes and higher levels of MMP-2 and MMP-9 in the serum of patients with metastatic and non-metastatic breast cancer patients with respect to healthy controls. These results are in accordance with literature findings (22).
In addition, this study revealed a direct and statistically significant correlation between higher serum levels of MMP-9 and CA 15.3 in patients with metastatic breast cancer with respect to healthy controls in accordance with our previously published results (23) and between higher expression of MMP-9 and G3 in accordance to Köhrmann et al. (24).
This is the first study which assessed the correlation between the expression of MMP-2 and -9 in the serum and sentinel lymph node of using two methods, namely immunohistochemistry for tissue assay and zymography for the assessment of serum. This approach was adopted because the MMP level in tissue is about 50 times lower those that found in bodily fluids and MMPs are often located in a small part of the original tissue and cannot be assayed due to the dilution of total tissue extract. The determination of MMP levels was therefore optimised using immunohistochemistry. The two gelatinases are more easily detectable, for example, in serum because they are released after their secretion by tumour. In fact, several different authors have shown that their serum levels are increased in several types of cancer (25).
Serum levels of both gelatinases are not indicators of tumour size but seem to be related to other tumour characteristics such as its invasiveness and high malignant potential (26). Many authors have noted that increased serum levels of both gelatinases are positively correlated with a high incidence of metastasis, having, thus, prognostic value (27-28). High serum levels of MMP-9 are associated with rapid disease progression, poor survival and metastasis (29).
In conclusion, this study suggested a significant clinical utility of both gelatinases in growth, invasion and metastasis in breast cancer both from the clinical point of view, when considering their increased expression in the first lymph node involved in the metastatic process and from a biological standpoint, since the high serum concentration of these enzymes can predict a poor prognosis, survival and an unfavourable clinical course.
- Received June 7, 2010.
- Revision received June 23, 2010.
- Accepted July 1, 2010.
- Copyright© 2010 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.