


Abstract
Background: The molecular and morphological alterations of the tight junctions in ulcerative colitis (UC)-associated colorectal cancer are still poorly understood. The possible involvement of claudin-1 (CL-1), one of the major tight junctional proteins, was investigated in the tumorigenesis of UC-associated CRC. Patients and Methods: A total of 39 patients with UC underwent surgical treatment from January 2001 until October 2009 at Kurume University Hospital in Fukuoka. CRC tissue specimens were analyzed to determine whether the expression of CL-1 correlates with clinicopathological factors and to determine the role of CL-1 and β-catenin in the alteration of tight junctions during tumorigenesis. Results: The operations were 30 of elective surgery and 9 of emergency surgery. Colectomy was performed in five patients (12.8%) because of UC-associated CRC, and in another patient (2.6 %) because of high-grade dysplasia. The immunostaining pattern of the high-grade dysplasia and UC-associated CRC for CL-1 showed much stronger and more diffuse staining in comparison to the normal or UC colonic mucosa. The expression of β-catenin was also positive or up-regulated in all of the UC-associated CRC and high-grade dysplasia tissue specimens. Conclusion: These observations suggested that CL-1 plays a pivotal role in the regulation of cellular morphology and behavior in UC. We speculate that increased CL-1 expression may be involved in the early stages of transformation in UC-associated neoplasia. CL-1 protein may therefore be a good candidate for surveillance of patients with UC.
Ulcerative colitis (UC) is an inflammatory bowel disease (IBD) of unknown etiology that involves severe inflammation of the colonic mucosa (1). It has been reported that the number of UC patients are increasing every year in Japan.
Patients with IBD are at increased risk of developing colorectal cancer (CRC). Eaden et al. (2) showed cumulative risks of 2%, 8% and 18% after 10, 20 and 30 years of disease, respectively, for patients with UC. IBD-associated colorectal carcinogenesis is characterized by an inflammation-dysplasia-carcinoma sequence (3) which differs from the adenoma-carcinoma sequence in sporadic CRC. High-grade or multifocal low-grade dysplasia indicates that the entire mucosal lining of the colon, exposed to chronic inflammation, is at increased risk of developing cancer (3, 4), thereby indicating proctocolectomy. Although CRC in UC only accounts for 1% of all cases of CRC seen in the general population, it is a serious a sequel of the disease and accounts for one sixth of all deaths in UC patients. In order to prevent development of CRC, patients with IBD are advised to undergo colonic surveillance aimed at detection of dysplasia or asymptomatic early CRC at a surgically curable stage. Currently, the surveillance guidelines followed most often are those defined by the American Gastroenterological Association (AGA) (5) and the British Society for Gastroenterology (BSG) (6). These guidelines recommend commencing surveillance after 8-10 years of disease in cases of Crohn's disease or extensive UC, and after 15-20 years of disease in cases of left-sided UC. Starting surveillance before these time intervals is not recommended. However, the evidence on which this is based is poor. Some studies have assessed the time intervals between the occurrence of IBD and CRC and evaluated how often IBD-associated CRC occurred before the first surveillance colonoscopy was advised (7-9).
Tight junctions are the most apical structures of cells, and tight junction proteins (TJPs) are very important in the maintenance of normal epithelial physiology. Recent studies have shown that considerable changes in the expression of TJPs are associated with various types of cancer. Neoplastic cells frequently exhibit both structural and functional disorganization in their tight junctions. To date, the claudins (CLs) and occludin have been identified as tight junction-specific integral membrane proteins. Occludin was the first component of the tight junction strands to be identified (10). However, subsequent studies, including gene knockout analyses, have shown that tight junction strands can be formed without occludin (11). Two other transmembrane proteins, CL-1 and CL-2, have also been identified as integral components of tight junction strands (12).
The altered expression of some CLs has also been found in many other types of human cancer such as breast, ovarian, prostate, liver and stomach cancer (13, 14). CL expression has been shown to have a prognostic value; CL-1 in colon cancer (15-17), CL-18 in gastric cancer (18), and CL-10 in hepatocellular carcinoma(19). The differential expression of genes encoding TJPs was detected in CRC (15, 19). The up-regulated expression of CL-1 in CRC has also been reported (16, 17, 20-22). These studies suggest that the CL family, especially CL-1, thus play a causal role in the process of cellular transformation and invasion in CRC. It is important to investigate the various TJPs in CRC tissues of patients with UC for their potential clinical efficacy in the therapy and diagnosis of UC-associated CRC.
The aim of this study was to analyze the correlation between the expression of CL-1 in UC-associated CRC tissues with clinicopathological factors and to investigate its possible functions in tumorigenesis in patients with UC.
Patients and Methods
Patient and tissue samples. A total of 39 patients with UC underwent surgical treatment from January 2001 until October 2009 at Kurume University Hospital in Fukuoka. Informed consent was obtained from all of the patients before performing surgical resection, while also receiving the approval from the Institutional Review Committee for Research on Human Subjects at the Kurume University Hospital. Tumor differentiation and the degree of invasion were examined by pathologists, and histopathological classification was performed according to the General Rules for Colorectal Cancer Study (23). The clinical information on the patients is summarized in Table I. All patients underwent total colectomy, ileo-anal anastomosis and diverting ileostomy. Ileostomy was closed after confirmed anastomosis conditions after 3 to 6 months from the first operation.
Data collection. The following data were collected from patient charts: type of UC, sex, age, disease duration (months), total steroids (g), chief complaint, body mass index (BMI), operative indications, and leukocytapheresis (LCAP) therapy.
Immunohistochemistry. Immunohistochemistry was performed as described previously (16, 24). The tissue sections were stained with mono-/polyclonal antibodies (diluted at 1:100) against CL-1 (Zymed Laboratories Inc., San Francisco, CA, USA) and β-catein (Dako Cytomation, Denmark). Immunostaining was assessed as positive or negative.
Clinical information on patients and their colorectal specimens (n=39).
Results
Operative indication for UC. Table II shows the operative indication of UC at our university. The operations were 30 of elective surgery and 9 of emergency surgery. Twenty-four patients underwent colectomy because of resistance to medical therapy, one patient had severe colitis, six patients had uncontrolled bleeding, and two patients had toxic mega colon. Colectomy was performed in five patients because of UC-associated CRC and in another patient because of high-grade dysplasia.
The clinical data for the six patients who underwent colectomy are summarized in Table III. Five out of six patients were men. Their mean age was 45.5 years, BMI was 18.4, total steroid was 16.9 g, and duration of disease was 124.5 months. Concerning the UC disease type, four patients had total colitis, and two patients had left-sided colitis.
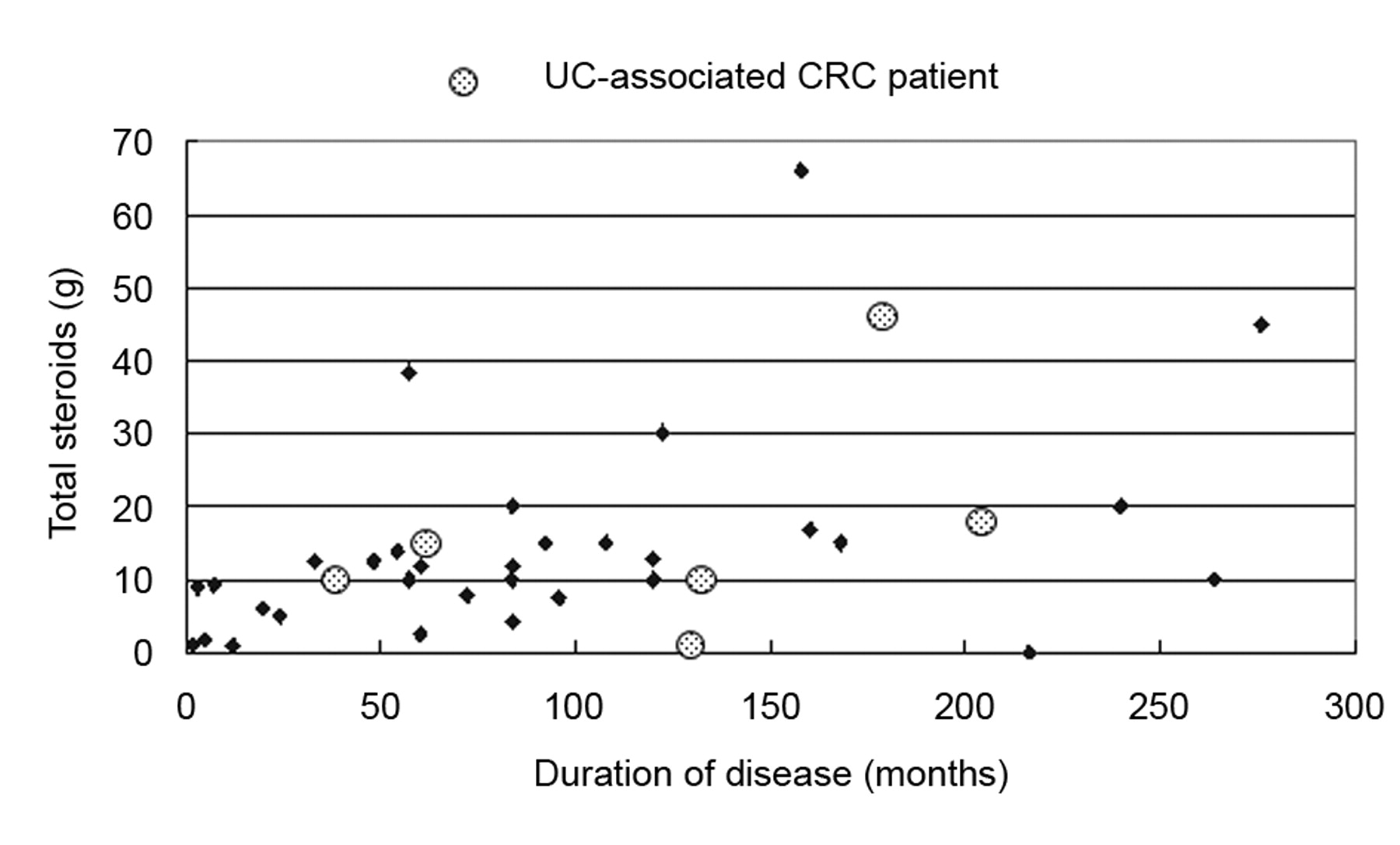
Correlation between the total steroid received and the duration of disease. We investigated the correlation between total steroid use and the duration of disease, as shown in Figure 1. No significant correlation was detected. Surprisingly in the UC-associated CRC group, five out of six patients had received more than 10 g total steroids, and four out of six patients had survived over 120 months.
Operative and histological findings. Figure 2A shows intraoperative findings. The patient was a 43-year-old Japanese male who had been diagnosed with UC. He has continued to receive treatment with steroids, LCAP etc. for UC for 18 years. The UC-associated CRC was found in the sigmoid colon, and several regional lymph nodes were obviously swollen. The surgical specimen is shown in Figure 2B. There was tumor in the sigmoid colon which was scirrhous carcinoma. The histopathological findings were of poorly differentiated adenocarcinoma, venous invasion: 3, lymphatic invasion: 3, depth of carcinoma: subserosa, lymph node metastasis: 3+, stage IV. The patient underwent surgical procedures (total colostomy, lymph node dissection, ileostomy and ileo-anal canal anastomosis). Six months after surgical treatment, the patient died due to UC-associated CRC.

Correlation between the total steroid use (g) and the duration of disease (months) in the study cases (n=39).

A: Typical operative findings found during total colectomy. The colitic tumor was located in the sigmoid colon, and several regional lymph nodes were clearly swollen. B: The surgical specimen is also that shown in (A). The tumor was found to be scirrhous carcinoma.

Hematoxylin-eosin (top) and immunostaining of CL-1 (middle) and β-catenin (bottom) in UC mucosa (left) and UC-associated CRC tissue (right) of a patients with UC-associated CRC.
Expression of CL-1 and β-catenin protein in human normal and neoplastic clonic tissue specimens. Immunostaining was used to confirm changes in the distribution pattern of CL-1 and β-catenin (Figure 3). In the normal colonic mucosa, all the epithelial cells expressed CL-1 along the cell membrane, but not in the cytoplasm.
Figure 3 demonstrates that the expression of CL-1 protein was up-regulated in CRC tissues in comparison to the normal mucosa with UC. An increase in the expression of CL-1 protein was observed in six out of six UC-associated CRC and high-grade dysplasia samples in comparison to the normal and UC mucosa. The immunostaining pattern of the high-grade dysplasia and UC-associated CRC tissues for CL-1 was much stronger and more diffuse in comparison to the normal or UC colonic mucosa. The expression of β-catenin was also positive or up-regulated in all of the UC-associated CRC and high-grade dysplasia tissue specimens.
Operative indication for UC patients (n=39).
Clinical information of patients with UC-associated CRC (n=6).
Discussion
This study demonstrated that CL-1 was up-regulated in high-grade dysplasia and UC-associated CRC tissues in patients with UC. On the other hand, β-catenin transcriptional activity is elevated in neoplastic tissues in UC and this may contribute to increased CL-1 expression. These observations suggested that CL-1 plays a pivotal role in the regulation of the cellular morphology and behavior in tissue from UC-associated CRC. We speculate that increased CL-1 expression may be involved in the early stages of transformation in IBD-associated neoplasia. CL-1 protein may therefore be a good candidate for surveillance of patients with UC.
Patients with longstanding UC and Crohn's disease have an increased risk of developing CRC (25-28). The mechanisms underlying this susceptibility are not well understood, and the molecular events that contribute to this phenotype are ill-defined. This severe complication of IBD generally develops in longstanding disease. The risk appears to be related to the cumulative effect of chronic inflammation and correlates directly with the extent and duration of disease, as well as with the severity of inflammatory activity. However, the detection of early CRC is often difficult in patients with UC because there is inflammation in the background mucosa and it predominantly represents flat-type ill-delineated lesions. Therefore, UC-associated CRC is often detected at an advanced stage and is associated with a very poor prognosis. One approach to overcome this difficulty is to use the presence of dysplasia, which is considered to be a precancerous lesion in UC-associated CRC, as a surrogate marker for early detection. However, identification of dysplasia using endoscopy requires greater skill than detection of cancer itself because of its rare occurrence and apparently normal-looking appearance.
Consensus guidelines recommend 30-40 biopsies; colonoscopy can be quite cumbersome to perform (5, 6). The technique of colonoscopy should involve 4 quadrant random biopsies at 10 cm increments throughout the colon in addition to target biopsies of suspiciously abnormal mucosa. However, it is very hard to take the recommended number of biopsies during colonoscopy. In a recent study, overall, the mean number of biopsies taken was found to be 24 (9). A finding of indefinite dysplasia should prompt accelerated surveillance, with a repeat examination after 3 to 6 months. Despite improvements in optical resolution of modern endoscopes, colonoscopy is less sensitive for detecting precancerous dysplasia in UC.
Several of the molecular alterations that contribute to sporadic CRC are also found in UC-associated CRC, including loss of adenomatous polyposis coli (APC) and p53 tumor suppressor gene function. However, the timing and sequence in which these genetic mutations occur differs from those of sporadic CRC. While the description of an inflammation-dysplasia-carcinoma sequence facilitates our understanding of the molecular alteration involved in UC-associated CRC, it is important to recognize that this process does not necessary occur in a systematic sequential progression from inflammation to indefinite dysplasia to high-grade dysplasia and ultimately to carcinoma. With regard to the genetic abnormality of UC-associated cancer and dysplasia, mutation of K-RAS and APC are relatively rare (29-32), and in contrast, p53 mutation is frequently positive (31, 33, 34). Moreover, hypermethylation of genes such as the p16 gene has recently been detected (35, 36). Although several such studies have been reported, the effectiveness of surveillance to mitigate cancer risk in UC has not been firmly established. At present, no predictive test exists for UC-associated neoplasia with high positive and negative predictive values using clinical and endoscopic features alone of patients with UC.
On the basis of previous reports suggesting that expression of CL-1 is altered in invasive colon cancer (18, 37-42), we hypothesized that modified expression of CL-1 could be associated with the increased risk of CRC with UC. However, CL-1 distribution and expression has not been characterized in UC-associated pre-malignant colonic dysplasia and CRC.
To assess the association between altered CL-1 expression in UC and neoplastic risk, we compared the expression in non-neoplastic UC and UC-associated CRC and dysplasia. Increased expression of CL-1 was present in UC-associated CRC and dysplasia. Given the emerging association of neoplastic risk in UC with inflammatory activity, these data suggest that increased expression of CL-1 in this setting may contribute to neoplastic progression. Although this change in CL-1 expression is expected to impact a barrier function, it is not clear that barrier modulation is the mechanism by which CL protein expression influences neoplasia. It is possible that CL protein interacts with signaling pathways, including transforming growth factor-beta (TGFβ)/SMAD and β-catenin (43) (37), in a manner that is separate from their effects on the barrier function. The previous observation that CL-1, which is a TJP, is regulated by β-catenin/TCF/lymphocyte-enhancer factor (LEF) signaling (37, 44, 45) suggests that the increased CL-1 expression observed may be due to β-catenin activation. We therefore assessed β-catenin expressed in dysplasia and UC-associated CRC tissues. As expected, increased translocation of β-catenin from the lateral membranes to the nucleus was strikingly present in high-grade dysplasia and UC-associated CRC. This observation designates β-catenin as an upstream regulator of CL-1 in UC.
We previously reported that a CL-1-overexpressing CRC cell line was generated, and the effects on the tight junctional barrier, cell morphology, proliferation and migration were analyzed in order to find the relationship between this protein and CRC (17). Concretely, CL-1 overexpressing cells grew as aggregates in contrast to the monolayer formation of the parental cells, and the expression of CL-1 at the mRNA and protein levels was found to increase in the CRC tissue in comparison to that in the normal tissue specimens. Therefore, CL-1 plays a pivotal role in the regulation of the cellular morphology and behavior in the colonic epithelium.
This study also suggests that high-grade dysplasia and UC-associated CRC in patients with UC results in an increase in β-catenin transcriptional activity that may contribute to increased CL-1 expression. Thus, increased CL-1 expression may contribute to carcinogenesis in UC. We speculate that increased CL-1 expression may be involved in the early stages of transformation in IBD-associated neoplasia. CL-1 protein may therefore be a good candidate for surveillance of patients with UC using biopsy samples. In further studies, it will therefore be important to investigate CL-1 for its potential clinical use in UC-associated CRC therapy and diagnosis.
Acknowledgements
This study was supported by a Grant-in-Aid for Scientific Research (No. 21591740), Japan.
- Received June 8, 2010.
- Revision received July 17, 2010.
- Accepted July 20, 2010.
- Copyright© 2010 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}