


Abstract
Antitumour effects of third-generation bisphosphonates (BPs), such as zoledronic acid (ZOL), and the combined effects of ZOL with other anticancer agents against osteosarcoma cells have been reported previously. The aim of this study was to identify further combined antitumour effects using BPs and radiation in osteosarcoma cell lines. Materials and Methods: Cell proliferation, cell cycle analysis, and nuclear morphology were examined in each osteosarcoma cell line divided into three groups (ZOL alone, radiation alone and the ZOL/radiation combination). Results: Combined therapy (low-concentration ZOL and low-dose radiation) had significant growth inhibitory effects compared to the use of ZOL or radiation individually. Flow cytometric analysis revealed an increase in cells in the sub-G1 phase by combined treatment, and apoptotic cells were also observed. Conclusion: These findings suggest that combination therapy using BPs and radiation may be a promising therapy for osteosarcoma, producing fewer side effects and complications in the near future.
Osteosarcoma is a high-grade malignant bone neoplasm that commonly occurs in juvenile patients. Although the prognosis of these patients has improved substantially through the development of effective adjuvant or neoadjuvant regimens of chemotherapy, >20% patients still die as a result of tumour metastasis and unresectable tumour (1-5).
Chemotherapy for bone and soft tissue tumours is problematic since high-dose drugs are required compared with other tumour types due to the low concentration of drug reaching the tissue, and serious adverse drug reactions often oblige chemotherapy to be halted in patients such as those with elderly onset tumours. Therefore, new antitumour drugs and new therapy methods are urgently needed for bone and soft tissue tumours. Various new osteosarcoma therapies have been investigated worldwide, with many clinical trials performed on novel agents. Among these agents, the antitumour effects of bisphosphonates (BPs) have been recently reported (6-8).
BPs are effective inhibitors of bone resorption and have been used for the past three decades in the treatment of metabolic bone diseases (9). BPs can be divided into two classes based on differences in the structure of the R2 side-chain. Nitrogen-containing BPs (N-BPs), or so-called second- and third-generation BPs, have a basic nitrogen-containing moiety in the R2 side-chain. Non-nitrogen-containing BPs (Non N-BPs), or so-called first-generation BPs, do not contain a nitrogen in the R2 side-chain and are less potent antiresorptive agents than N-BPs.
N-BPs induce apoptosis in osteoclasts by inhibiting protein prenylation in small G-proteins through inhibition of farnesyl pyrophosphate synthase in the mevalonate pathway (10).
It has previously been reported that third-generation BPs, such as zoledronic acid (ZOL) and minodronic acid (YM529), show direct antitumour effects and synergistically augment the effects of anticancer agents in various cancer cell lines (11-15). Recently, several investigators have reported the anti-osteosarcoma effects of third-generation BPs in vitro (16-21) and in vivo (22-24).
In addition, the antitumour effects and the mechanism of third-generation BPs have previously been reported in murine osteosarcoma cell lines in vitro in order to clarify the direct anti-bone tumour effects of BPs. As a result, third-generation BPs halted the cell cycle at the S-phase, leading osteosarcoma cells to apoptosis (20).
However, BPs cannot overcome drug resistance alone; therefore, combination therapy with various antitumour drugs and third-generation BPs has been investigated (21). Those data revealed that BPs inhibit the growth of murine osteosarcoma cell lines by combination therapy compared with individual therapies.
Another well-established treatment modality for the local treatment of bone metastases is radiotherapy. Combined chemotherapy and radiotherapy for osteosarcoma has already been used clinically (25). Likewise, combined therapy using ZOL and radiotherapy may further inhibit cell growth, thereby decreasing the drug concentration and amount of irradiation to ultimately be safer than when used alone, with lower side effects.
Recently, there have been several reports concerning the combined effects of third-generation BPs with radiation in various cancer cell lines; for example breast cancer (26), prostate cancer, myeloma (27), lung cancer (28). However, there is no report on the combined effect of ZOL with radiation in osteosarcoma cells. Therefore, this study aimed to clarify the combined effect of BPs and radiation, and to analyse the cell cycle and induction of apoptosis in osteosarcoma cells.
Materials and Methods
Reagents. ZOL, (1-hydroxy-2-(1H-imidazole-1-yl) ethylidene-bisphosphonic acid, was obtained from Novartis Pharma AG (Basel, Switzerland). ZOL was dissolved in Ca+ Mg+ phosphate-buffered saline (PBS) and stored at −20°C. Appropriate drug concentrations were made by dilution with fresh medium immediately before each experiment.
X-Ray irradiation. Cultured cells were irradiated with 150-400cGy X-Ray using SOFTEX M-150WE (SOFTEX CO, LTD, Tokyo, Japan). The irradiation conditions selected were a distance of 1 cm from the focus to the specimen, an irradiation rate of 0.5 Gy/min in air.
Cell lines. A murine osteosarcoma cell line, LM8, was established from the murine Dunn osteosarcoma cell line (29). The MOS cell line was established from the murine osteosarcoma model developed at Massachusetts General Hospital (30). MG-63 was used as human osteosarcoma cells (31). These cells were maintained in Dulbecco's modified Eagle's medium supplemented with 15 mM HEPES buffer, 10% foetal bovine serum, and antibiotic solutions of penicillin (100 U ml-1) and streptomycin (100 μg ml-1). All cells were cultured at 37°C in a fully humidified incubator with 5% CO2. All experiments described were performed at least three times using cells in the exponential growth phase.
Concurrent exposure to ZOL and radiation MTT assay. Proliferation of the cell lines was determined using the methylthiazol-diphenyl-tetrazolium (MTT) assay, as previously described (32). LM8, MOS and MG-63 cells were cultivated in a flat-bottomed 96-well plate (Greiner Labortechnik, Frickenhausen, Germany) at 1×104 cells per well in 100 μl medium and incubated for 24 h, followed by incubation with various concentrations of ZOL and/or radiation at various doses for a further 72 h. The means of six data values for each treatment were calculated. For all cell lines, the linear relationship between the degree of proliferation and cell number was evaluated within the range of the experiment. Half-maximal inhibitory concentrations (IC50s) were determined and, based on the IC50s, the combined effects of ZOL at lower concentrations than IC50 with radiation at a lower dose than IC50 were investigated. LM8, MOS and MG-63 cells were treated with various lower concentrations of ZOL combined with various lower doses of radiation for 72 h. After 72 h, the rate of growth inhibition was evaluated by MTT assay. Data from three independent experiments were collected and Student's t-test was used to evaluate the efficacy of sequential treatment of ZOL and to compare the effects of each radiation alone or combination. P-values <0.05 were considered statistically significant and were derived from two-sided statistical tests.
Cell cycle analysis. To explore the possible mechanisms of ZOL alone, radiation alone or the combined effects of ZOL and radiation, LM8 cells were cultivated in a flat-bottomed 6-well plate at 2×104 cells/ml and analysed for cell cycle alterations by staining with propidium iodide (Sigma Aldrich, St. Louis, USA) after exposure to ZOL and/or radiation at various doses for 24 h, as previously described (33). The stained nuclei were analysed using a FACSCalibur flow cytometer (Becton Dickinson, Franklin Lakes, USA). DNA histograms were created using Cell Quest™ software for Apple Macintosh (Becton Dickinson).
Analysis of nuclear morphology. LM8 cells treated with ZOL and radiation under appropriate conditions were cultured for 72 h, fixed with 2% paraformaldehyde in PBS for 10 min, and then stained with DAPI (4′,6-diamidino-2-phenylindole dihydrochloride) (Nacalai Tesque, Inc, Kyoto, Japan) at 4°C in the dark. For fluorescence microscopy, cells were cytospun onto slides and examined using a universal microscope (Nikon, Tokyo, Japan) with UV illumination. Apoptotic cells were identified on the basis of characteristic changes, including nuclear condensation, fragmentation, and apoptotic bodies.
Results
Growth inhibitory effects of ZOL against murine and human osteosarcoma cells. ZOL inhibited the growth of murine and human osteosarcoma cells (LM8, MOS, MG-63) dose dependently. The IC50 values of ZOL for LM8, MOS, MG-63 after 72 h exposure were 8.5, 2.4 and 27 μM, respectively, as shown in Figure 1. ZOL effectively inhibited osteosarcoma cell growth; however, the IC50 of ZOL of the human osteosarcoma cell line was higher than that of murine osteosarcoma cell lines.

Growth inhibitory effect of ZOL. The ability of ZOL to inhibit the growth of LM8 (A), MOS (B) and MG-63(C) cells was determined by MTT assay, respectively. Data are presented as the mean±s.d. of three independent experiments.

Growth inhibitory effect of radiation. The ability of radiation to inhibit the growth of LM8 (A), MOS (B) and MG-63 (C) cells was determined by MTT assay, respectively. Data are presented as the mean±s.d. of three independent experiments.
Growth inhibitory effects of radiation against murine and human osteosarcoma cells. Radiation inhibited the growth of murine and human osteosarcoma cells, dose dependently. As shown in Figure 2, the IC50 values of ZOL for LM8, MOS, MG-63 after 72 h exposure were 300, 360 and 530cGy, respectively. The irradiation amount at IC50 for MG-63 cells, the human osteosarcoma cell line, was higher than for LM8 or MOS cells, murine osteosarcoma cell lines. Radiation showed almost the same antitumour activity for human and murine osteosarcoma cell lines.
Growth inhibitory effects of combination therapy against murine and human osteosarcoma cells. The combined effects of ZOL at lower concentrations with radiation at lower doses than IC50 for murine and human osteosarcoma cells, LM8, MOS and MG-63 were examined. The combined use of lower doses of ZOL and radiation induced significantly higher antitumour effects than when used alone, as shown in Figure 3. A significant growth inhibitory effect of combination with ZOL at higher than 5 μM under all irradiation conditions against LM8 cells was observed. ZOL 5 μM with irradiation at 100cGy inhibited the growth of LM8 cells to the IC50 level. In particular, the antitumour effect when treated with 7.5 μM ZOL combined with 150 cGy irradiation was stronger than when treated alone. Concerning MOS cells, no significant difference was observed in the combination of ZOL at 0.4 μM with irradiation at 50 cGy. A significant growth inhibitory effect was observed with ZOL at higher than 0.8 μM and irradiation at higher than 100 cGy. Cell growth could be inhibited to the IC50 level by the combination of ZOL at 1.2 μM with irradiation at 150 cGy. In Figure 3C, a significant growth inhibitory effect was observed under all conditions against MG-63 cells. The combination of ZOL with radiation strongly inhibited cell viability in each cell line compared to when used alone, even if at a higher concentration or higher irradiation amount.
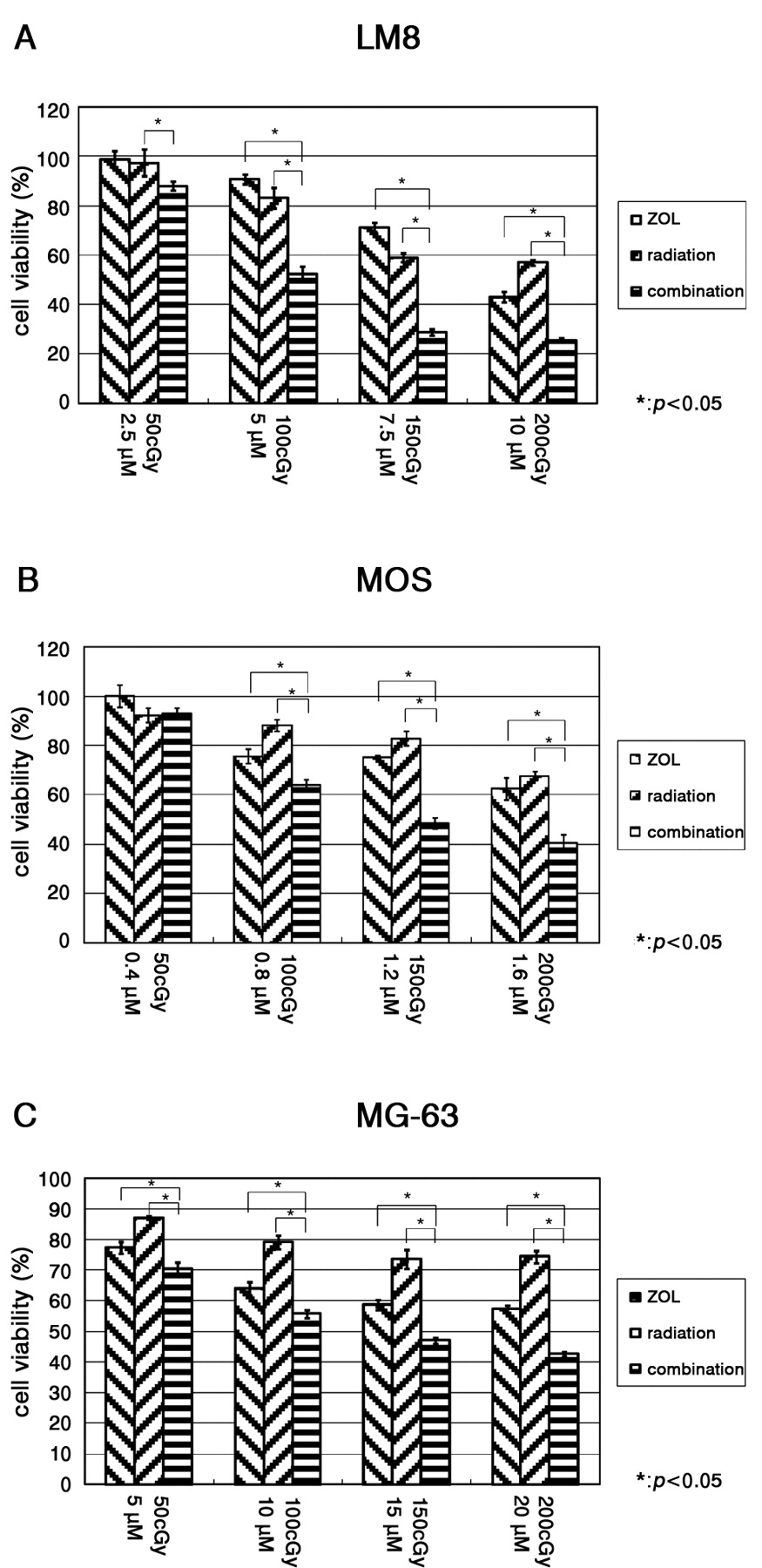
Growth inhibitory effect of combination. The ability of combination to inhibit the growth of LM8 (A), MOS (B) and MG-63 (C) cells was determined by MTT assay, respectively. Data are presented as the mean±s.d. of three independent experiments.
Combined effects of ZOL with radiation on the alterations of cell cycle. When LM8 cells were treated with 7.5 μM ZOL combined with 150 cGy radiation for 72 h, there was an increase of cells in the S-phase between G0/G1 and G2M-phases and in the rate of LM8 cells in sub-G1 compared with ZOL and radiation alone (Figure 4A). Three patterns for the proportions of the cell in the sub-G1 are shown in Figure 4B. When LM8 cells were treated with ZOL 7.5 μM with irradiation of 150 cGy, many cells in the sub-G1 increased in contrast to other conditions.
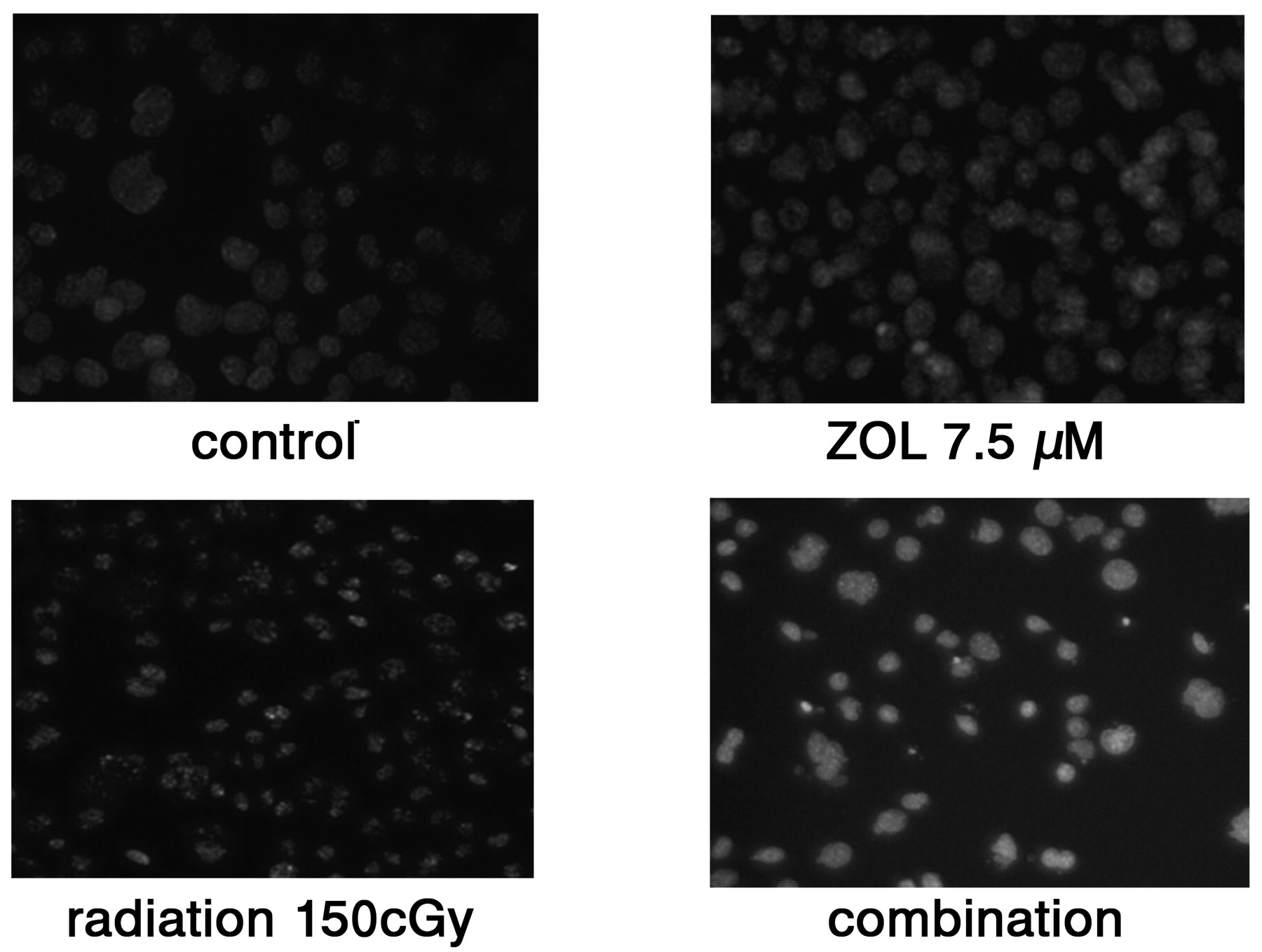
Combined effects of ZOL with radiation on nuclear morphology. When LM8 cells were treated with 7.5 μM ZOL combined with 150 cGy radiation for 72 h and stained with DAPI, the nuclear fragmentation and apoptotic bodies characteristic of apoptosis were observed (Figure 5).
Discussion
BPs are widely used to treat bone diseases, such as osteoporosis and metastatic bone tumours. Recently, there have been reports on their antitumour effect. The mechanisms of the antitumour effects of BPs are thought to be ‘BP triangle’ effects, i.e. the integration of the following three factors: changes in the bone marrow micro-environment with apoptosis of osteoclasts, immunological mechanism through γδT-cells induced by N-BPs, and direct antitumour effects by inhibiting protein prenylation in small G-proteins (34). It has been shown that BPs provide useful information on various malignant tumours according to previous reports; however, one of the problems in clinical use is that the IC50 is high, because BPs are rapidly cleared from the circulation within a few hours (35-37).
Current trends in the treatment of human tumours are the combination of BPs with anticancer agents. This approach results in improved responses as well as the ability to use lower and less toxic concentrations of the drugs. Other investigators have demonstrated the synergistic or additive growth inhibition of ZOL and various antitumour drugs against leukemia (11, 12), lung cancer (13), bladder cancer (35), and breast cancer (36, 37). It has also been demonstrated that the combination of ZOL with doxorubicin, cisplatin, paclitaxel or gemcitabine may be effective against murine osteosarcoma cells, compared to any of these agents alone (21).
On the other hand, there are several reports concerning the combined effects of third-generation BPs with radiation in various cancer cell lines, for example breast cancer (26), prostate cancer, myeloma (27) and lung cancer (28) to obtain further antitumour effects. The IC50 of MCF-7, a human breast cancer cell line, was 20 μM by ZOL alone, 500 cGy by irradiation alone, and 10 μM and 200 cGy for the combination of ZOL with irradiation (26). According to Algur et al., the IC50 of C4-2, a human prostate cancer cell line, was 82 μM with ZOL alone, 1314.6 cGy with irradiation alone, and 32 μM and 320.4 cGy for the combination of ZOL with irradiation ZOL (27). In this report, it was shown that the combination of ZOL with radiation showed true synergism, rather than when used alone, as shown clearly by the growth inhibitory effects against murine and human osteosarcoma cells (Figure 3). Stronger combination effects were observed in MG-63 than prostate cancer and were equal to breast cancer. In this study, it was reported that the combined use of lower doses of ZOL and radiation enhanced the antitumour effects than when used alone in murine and human osteosarcoma cells, LM8, MOS and MG-63, through an increase in the ratio of cells in sub-G1, growth inhibition, and apoptosis induced by nuclear fragmentation. Thus, combination therapy using BPs and radiotherapy may be useful to increase the antitumour effects and to decrease side-effects and complications. According to previous reports, the IC50 of ZOL in osteosarcoma cell lines is lower than in other cancer cell lines; therefore, treatment of osteosarcoma with a lower concentration of ZOL is achievable clinically. These results of the combination of BPs and radiation are novel and intriguing, suggesting the clinical utility of using BPs combined with radiation, especially in patients with osteosarcoma.
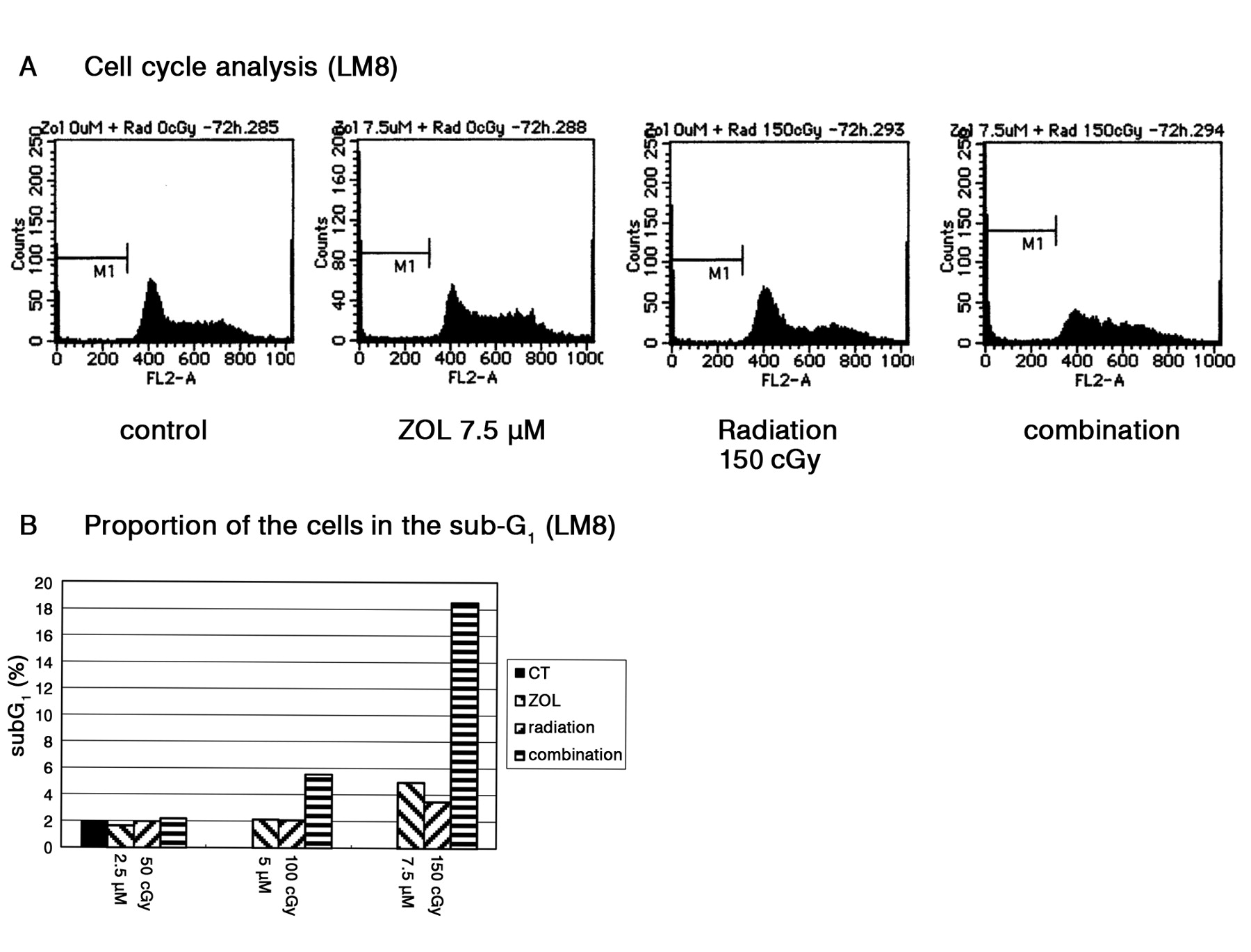
Cell cycle analysis and proportion of the cell in the sub-G1. A: Cell cycle analysis of combined treatment of ZOL with radiation. The effect of agents on the cell cycle was evaluated by flow cytometry of osteosarcoma cells that had been exposed to 7.5 μM ZOL combined with 150 cGy radiation for 72 h. B: There was a significant increase in the ratio of LM8 cells in sub-G1 compared with ZOL (at 5 μM or 7.5 μM) or radiation (at 100 cGy and 150 cGy) alone.
However, the precise synergistic mechanism of ZOL and radiation is currently unknown. The biochemical mechanism of action of BPs is now well documented, with N-BPs such as ZOL affecting cellular behavior through inhibition of the mevalonate pathway (9). In a previous paper, the potential mechanisms of the antiproliferative effect of ZOL, which include direct apoptosis induction, and indirect anticancer effects were reviewed (34).
Radiotherapy is one of the most effective treatments for bone metastases (38-41). Generally, tumour cells are usually most sensitive during the latter part of the S-phase and in the G2- or M-phase for radiotherapy (42). Ural et al. reported by flow cytometric analysis of ZOL-treated multiple myeloma cells an increase in the proportion of cells in the S-phase, possibly due to slower progression through the S-phase or a block between the S-phase and G2M-phase in the cell cycle (26, 43). Using a small cell lung cancer cell line, Matsumoto et al. reported that cell growth inhibition may involve not only the induction of apoptosis, but also the prolongation of cell cycle progression by ZOL alone or combined with anticancer agents (13). This ability of ZOL to arrest cells in the G2M-phase or to prolong cell cycle progression raises the possibility of ZOL as a potential cell cycle radiosensitizer because G2 and M cells are more sensitive than cells within other cell cycle phases (44).

DAPI staining (LM8). Untreated LM8 cells or LM8 cells treated with 7.5 μM ZOL, 150 cGy radiation, and combined with both for 72 h were stained with DAPI.
In the present study, the mechanism of the combined effects of ZOL and radiation was investigated using flow cytometry in order to gain further insights into their mechanism of action for osteosarcoma. There was no alteration of the cell cycle by ZOL alone or by radiation alone when we investigated at lower doses of ZOL or radiation than IC50; however, when a lower dose of ZOL was combined with a lower dose of radiation, cells in the S-phase increased, despite the fact that ZOL or radiation used individually did not affect the cell cycle. Moreover, when ZOL with radiation showed a strong antitumour effect against osteosarcoma cells, combined therapy induced not only an increase of sub-G1 cells but also the appearance of apoptotic cells. These results indicated that ZOL and radiation might cause DNA damage and enhance cytotoxic activity together. Therefore, it is difficult to clarify the mechanism of the combined effect of ZOL and radiation although there have been some reports by flow cytometric analysis. Other factors should be considered other than the cell cycle.
In conclusion, the combined use of lower doses of ZOL and radiation enhanced the cytotoxic effects compared to their individual use in murine and human osteosarcoma cells. Combining lower radiation treatment with a lower dose of ZOL might produce the same effect as the standard ZOL and radiation dose, thus producing fewer side-effects and complications. This combination method may be a promising therapy for osteosarcoma in the near future.
Acknowledgements
This work was supported by KAKENHI (Grant-in-Aid for Scientific Research C:20591764 to HM)
- Received April 28, 2010.
- Revision received May 20, 2010.
- Accepted May 25, 2010.
- Copyright© 2010 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}