


Abstract
Background: Recent studies indicate a possible relationship between hypothyroidism and breast cancer in vivo. In addition, oestrogen-like effects of thyroid hormones on breast cancer cell growth are seen in vitro. Therefore, this study evaluated thyroid function in breast cancer patients, women with benign breast tumour and healthy controls. Patients and Methods: Breast cancer patients (n=65), women with carcinoma in situ (n=13) or benign breast tumour (n=27), and healthy controls (n=38) were included in the study. Thyroid history was reported. Thyroid hormones (fT4, fT3, TSH) and thyroid antibodies (TPO, TRAK and TG) were determined. Statistical analysis was performed by Mann-Whitney U and Fisher's exact test (p<0.005 significant). Results: fT3 and fT4 levels were highest in breast cancer patients, and differed significantly from controls (fT3 and fT4: p<0.001) as well as from patients with benign breast tumour (fT3: p=0.021; fT4: p=0.017). TSH was highest in the control group without reaching significance. With regard to TRAK antibodies, breast cancer patients showed the highest levels differing significantly from women with benign breast tumours (p=0.048). Conclusion: Significant differences in fT3/fT4 as well as TRAK levels were observed among breast cancer patients, women with benign breast tumours and healthy controls. Further studies using larger patient groups are part of ongoing research.
Breast cancer is the most frequent malignant tumour in women worldwide with about 1 million women being affected (1). In Germany, almost one in ten women is diagnosed with breast cancer. Apart from familial predisposition, occupational, reproductive and hormonal factors, no clinically important risk factors for breast cancer are known. The conventional prognostic markers are: dimension and histopathology type of the tumour, number of afflicted lymph nodes, grading, hormone receptor status and Her/2-neu-status. A high percentage of positivity of antibodies to thyroid peroxidase has been proven in women with breast cancer in comparison to healthy controls (12). Some studies have indicated thyroid autoimmune changes as prognostic factors in breast cancer (2). Recent studies showed increased serum levels of thyroid-stimulating hormone (TSH), with subclinical or manifest hypothyroidism in 10.0-19.7% of breast cancer patients (3, 4).
As early as the early 19th century, thyroid hormones were utilised for therapeutic purposes in breast cancer patients. Since then, many trials have been initiated in order to identify the relationship between thyroid dysfunction and breast cancer disease (5, 6). Some of these studies showed higher incidence of breast cancer in patients with thyroid dysfunction compared to healthy controls (5-8, 10, 24). Furthermore, several studies have provided evidence for the relationship between breast cancer and autoimmune thyroid disorders (9-11). In particular, a high prevalence of thyroperoxidase antibodies (TPO-AB) and autoimmune hypothyroidism is present in breast cancer patients and patients with non-malignant breast tumours in comparison to healthy controls (9). Most of these studies have been retrospective and used different diagnostic criteria for detection of thyroid diseases. However, examination of thyroid hormones was always performed after treatment (breast surgery, chemotherapy). This is particularly important since the (auto)immune system can be influenced by surgery or chemotherapy (12), triggering or worsening autoimmune diseases (13-16).
Therefore, in this prospective case–control study, only patients with newly diagnosed breast cancer or benign breast disease were included before surgery, chemotherapy, radiation or antihormonal therapy. Thyroid function was investigated in breast cancer patients and compared to women with benign breast tumour and healthy controls.
Patients and Methods
The study population consisted of breast cancer patients (Group I, n=65), patients with carcinoma in situ (Tis, Group II, n=13), women with benign breast tumour (fibrolipomatosis, fibroadenoma, mastopathia, ductal and tubular adenoma; Group III, n=27) and healthy controls (mammograms, ultrasound and partially MRI performed; Group IV, n=38) (Figure 1).
Breast cancer was diagnosed by vacuum biopsy and tumour stage was mostly specified as pathological but also partially as clinical stage because some breast cancer patients were at the start of neoadjuvant chemotherapy. Breast cancer was classified according to the TNM system (27): T1 tumours (≤2 cm diameter, n=32, 49.2%), T2 tumours (2-5 cm diameter, n=25, 38.5%), T3 tumours (> 5 cm diameter, n=4, 6.2%), T4 tumours (include expansion of chest wall, oedema, ulceration or inflammatory disease, n=1, 1.5%) and primary metastatic disease (detected by staging examinations, n=3, 4.6%). Furthermore, positive axillary nodal status (N1) was present in 24 patients (36.9%), whereas 39 patients (60%) had negative axillary lymph nodes (pN0). In 2 patients (3.1%), the nodal state was unknown. Tumour grading was subdivided as follows: 4 out of 59 patients with known grading of the tumour (6.8%) had a G1 (low grade) tumour, most patients (37; 62.7%) had a G2 tumour (intermediate grade) and 18 patients (30.5%) had a high grade tumour (G3). Oestrogen receptor (ER, Score 0-12) and progesterone receptor (PR, Score 0-12) scores were determined in 62 out of 65 (95.4%) breast cancer patients. Nine patients (14.5%) had hormone receptor (HR)-negative breast cancer, all other patients had an HR-negative tumour. Her/2-neu-status (0-3+; 12 out of 61 patients (19.7%) Her2-neu-positive) and tumour markers, carcinoembryonic antigen (CEA; U/l) and cancer antigen (CA) 15-5 (ng/dl) were also investigated. Out of 65 breast cancer patients, CEA was increased in 17 patients (26.6%) and CA15-3 in 11 patients (17.2%).
Breast cancer patients, women with benign tumours and healthy controls gave formal consent for participation in the study. Signed informed consent was obtained from all participants, allowing analysis of all clinical and laboratory data mentioned in this paper. The Human Investigation Review Board of the Ludwig Maximilians University Munich approved the study.
Serological determination of thyroid hormones and detection of TPO, TRAK and TG antibodies (concentration, normal range) was performed as follows: serum-free thyroxine (fT4; 0.9-1.7 ng/dl), serum-free triiodothyronine (fT3; 2.5-4.3 pg/ml), thyroid-stimulating hormone (TSH; 0.44-3.80 μU/ml), thyroperoxidase antibodies (TPO; <40 IU/ml normal range), thyrotropin receptor antibody (TRAK; <1.0 mIU/ml normal range) and thyroglobulin antibodies (TG; <100 IU/ml normal range).
Quantification of TSH, fT4, fT3, Anti-TPO, anti-TG, and TSH-receptor antibodies was performed using an automated immunoassay system (Roche Cobas, Mannheim Germany) based on electrochemiluminescence.
TSH values >3.80 μU/ml were considered to indicate hypothyroidism, levels from 3.8-10.0 μU/ml were considered to indicate latent hypothyroidism and values >10.0 μU/ml were considered to indicate manifest hypothyroidism. TSH values <0.44 μU/ml were considered to indicate hyperthyroidism. TPO levels >40 IU/ml were considered to indicate autoimmune thyroid disease and TRAK levels >1.0 mIU/ml combined with TG levels <100 IU/ml were considered to indicate autoimmune disease.
Statistical analysis. Parametrically distributed data are expressed as mean±standard deviation (SD) (minimum, maximum). All other data are presented as the median (Q1-Q3=interquartile range). Independent variables were analyzed by Mann-Whitney-U-test, all others by using Chi-Square and Fisher's exact test. P-values <0.05 were regarded as statistically significant. Data were examined with SPSS for Windows (release 16.0).
Results
Mean age did not differ significantly within the study population (Table I). Focusing on anamnestic data it can be seen that many of the breast cancer patients, but also women with benign breast tumours and healthy controls, showed thyroid dysfunctions.
History of thyroid gland. A history of thyroid disease was known in 16 out of 65 (24.6%) breast cancer patients according to the following classifications: 7 had hypo-, 2 had hyperthyroidism, 1 had hot thyroid nodule and 6 underwent thyroid surgery for thyroid cancer, autonomous adenoma of the thyroid gland or multiple cysts. Breast cancer patients had a more frequent history of thyroid surgery than women with benign tumours or healthy controls (p<0.05). With regard to Tis patients, 30.1% (4 out of 13) had a thyroid disease in the past: 1 had autonomous adenoma and 3 underwent thyroid surgery for thyroid cancer and cold nodules of the thyroid gland. In women with benign tumours, the incidence of thyroid disease was 6 out of 27 (22.2%): 5 had hypothyroidism and 1 underwent thyroid surgery for autonomous adenoma, whereas in healthy controls, only 3 out of 38 (7.9%) had thyroid disorders (all had hypothyroidism).
Thyroid parameters. Six breast cancer patients (6 out of 65, 9.2%) had TSH values below and 2 (3.1%) higher than the normal range; 2 (3.1%) had abased fT4 levels (Table III). Furthermore, 4 patients (6.2%) had fT3 levels below the normal range (Table II). TG antibodies were elevated in 12 (12 out of 65, 18.5%), TPO in 6 (9.2%) and TRAK antibodies in 2 (3.1%) breast cancer patients (Table IV).
With regard to Tis patients, 3 (23.1%) had abased TSH levels and 2 (15.4%) fT3 values under the normal range (Table II); 2 (15.4%) showed raised TG and 1 (7.7%) elevated TPO antibodies.
In the group of patients with benign breast tumours, 2 (7.4%) had TSH values <0.44 μU/ml and 1 (3.7%) abased fT3 levels (Table II). 18% (5 out of 27) had elevated levels of TG-, 7.4% (2 out of 27) of TPO- and 40.7% (11 out of 27) of TRAK antibodies. Furthermore, 11 patients had increased TRAK antibodies (40.1%) (Table IV).
In the control group, 2 patients (5.3%) had abased TSH levels and 2 had elevated TSH levels. Eight patients (21.1%) showed fT3 values under the normal range (Table II).
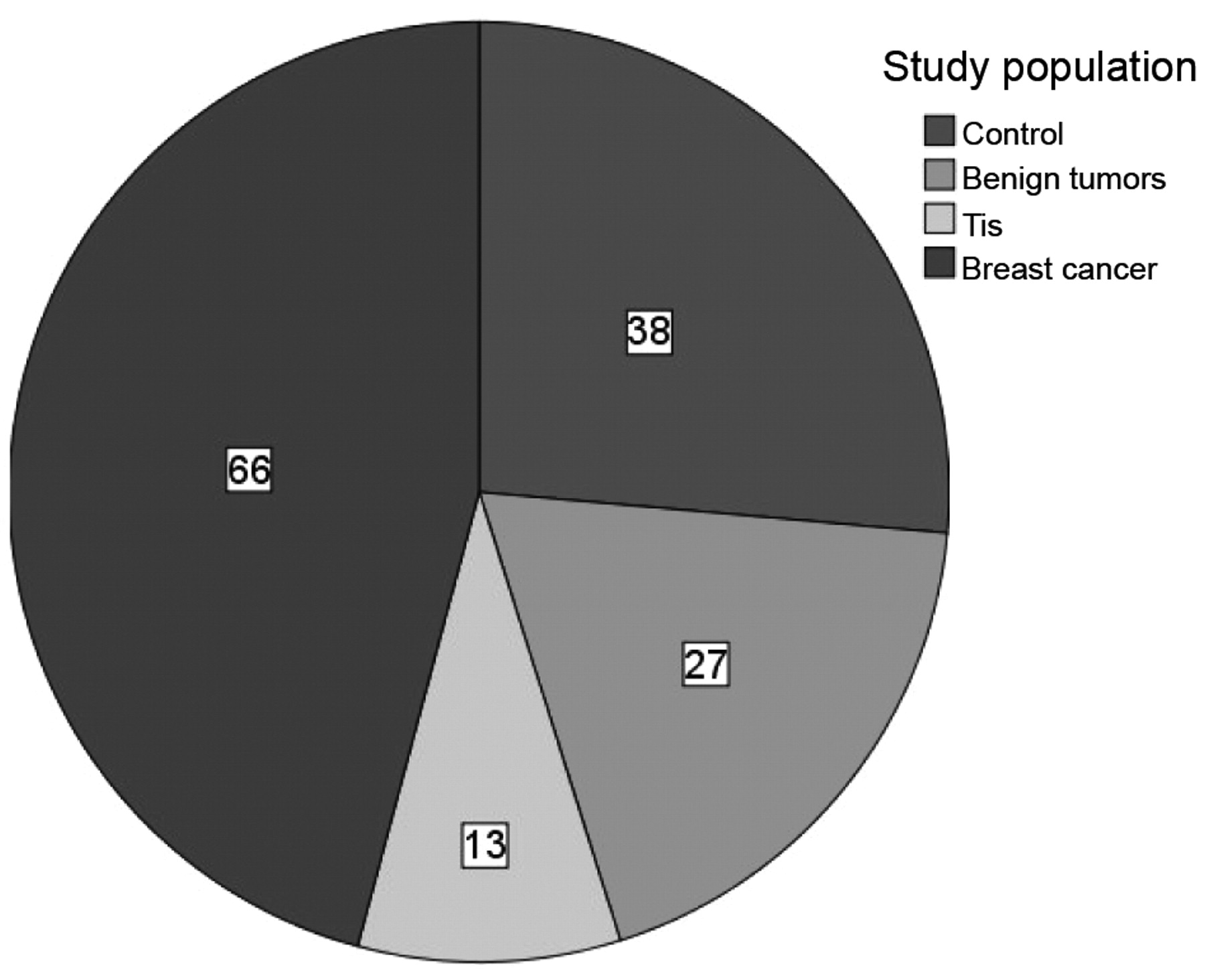
Study population. Number of patients and controls in different study groups.
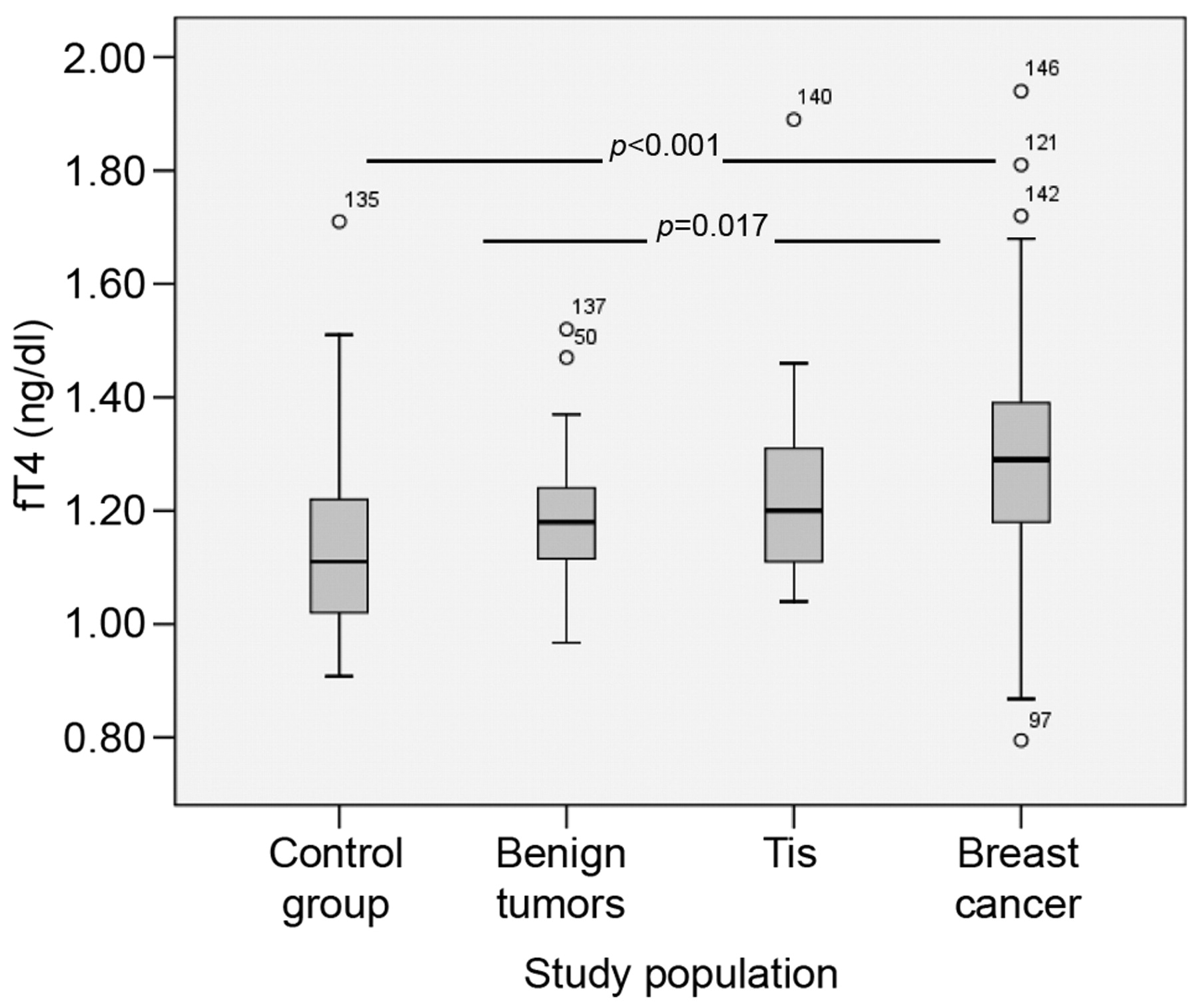
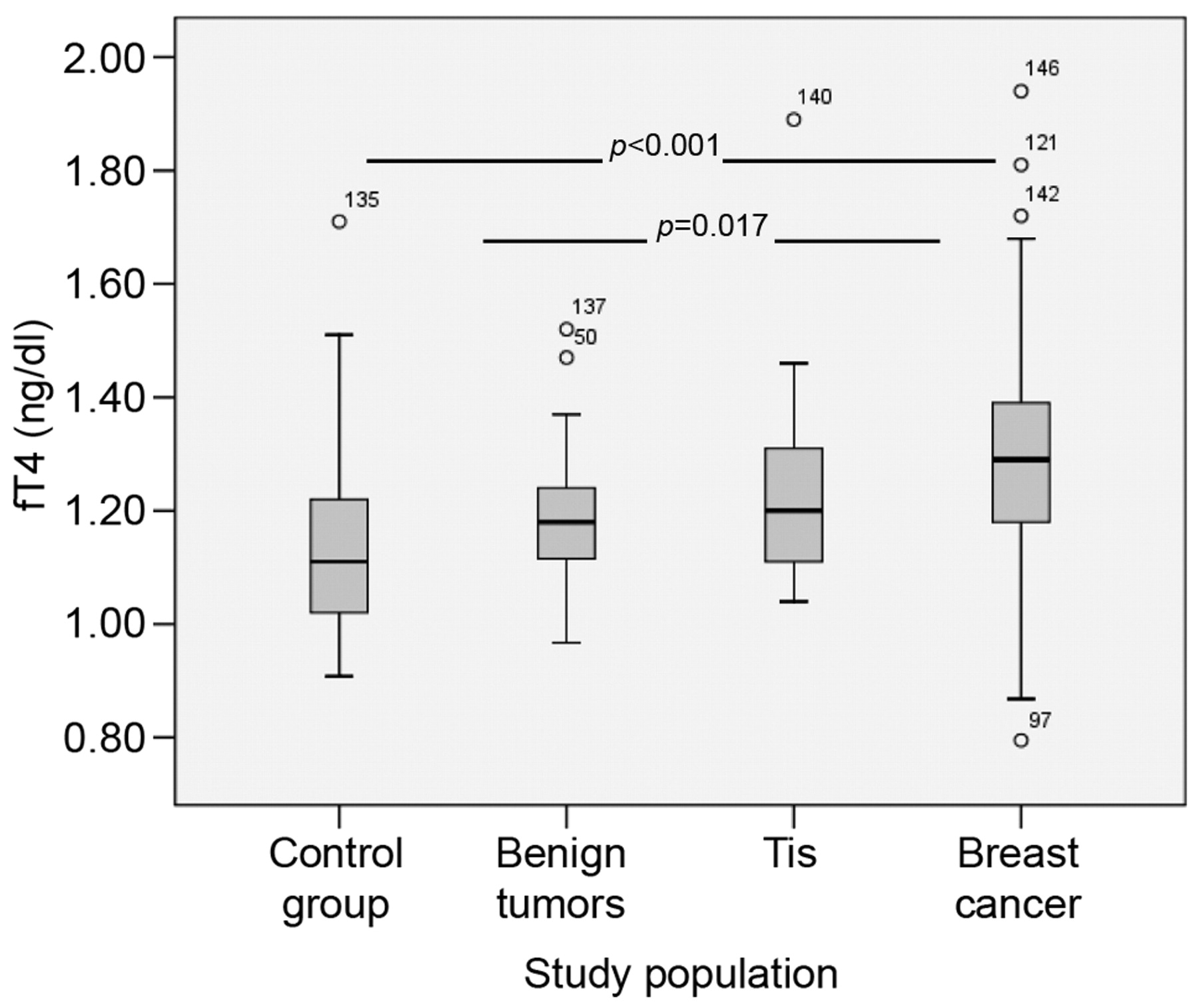
fT4 levels in study population. fT4 levels differed significantly between breast cancer patients and women with benign breast tumour as well as healthy controls. Data are presented as boxplots and p<0.05 denotes statistical significance. The open circles denote the number of patients with fT4 levels above the interquartile range.
Thyroid parameters of the study population.
Although fT4 and fT3 levels were within the normal range in breast cancer patients, ((mean±SD); fT3: 3.0±0.45 pg/ml and fT4: 1.3±0.2 pg/ml), they were significantly different from the respective levels in patients with benign breast tumour (fT4: p=0.017, fT3: p=0.021) and the healthy controls (p<0.001). Furthermore, breast cancer patients showed the highest concentrations of TRAK antibodies differing significantly from patients with benign tumours (p=0.048). TSH, TPO and TG antibodies did not differ significantly within the study population. Breast cancer patients had the highest concentrations of TPO and the lowest levels of TG antibodies (Table I). Tis patients showed significantly higher levels of fT3 compared to the control group (p=0.028, Table I). The highest concentrations of TG antibodies were measured in patients with benign breast tumours (141±318 IU/ml) without reaching significance (Table I).
Discussion
Many studies investigated thyroid function (fT3 and fT4 levels) in breast cancer patients. In preclinical models, T3 was able to sustain serum-free proliferation of several cell lines, including breast carcinoma cells (17, 18). In rodents, mammary gland development and physiology are sensitive to T3 (19). Epidemiological studies have provided conflicting results regarding the association between thyroid disorders and breast carcinoma risk (20-23). This prospective study confirmed the differences in thyroid hormones and thyroid antibodies in serum blood of breast cancer patients, patients with Tis and women with benign tumours in comparison to control women. Significantly higher levels of fT4 and fT3 (within the normal range) were present in breast cancer patients in comparison to women with benign breast tumours and healthy controls.
fT3 levels within study population.
In contrast to these findings, Kuijpens et al. (25) showed significantly lower levels of fT4 in breast cancer patients (n=2775) compared to women without breast cancer. This difference in observation may be due to the short observation time in the present study population; however, it is unknown whether the patients in the Kuijpens study that were identified as not having breast cancer had a benign tumour or Tis of the breast.
TSH is the most important thyroid hormone for diagnosis of hypo-/hyperthyroidism, therefore most studies focus on evaluation of TSH values. In this study population, mean TSH values were within the normal range. However, 10% of breast cancer patients showed TSH levels below the normal range.
Within this study, therapeutically adjusted hypothyroidism was more frequent (n=7) in breast cancer patients than in Tis patients, women with benign breast tumour and healthy controls. Furthermore, most patients with anamnestic hypothyroidism had TSH levels within the normal range due to therapeutic suppression. However, Limanova et al. and Jiskra et al. (3, 4) showed increased TSH serum levels and hypothyroidism in almost 20% of breast cancer patients.
Kuijpens et al. did not demonstrate differences in TSH values between breast cancer patients (at the time of diagnosis) and controls (25). However, they were able to demonstrate similar TSH concentrations in peri- and post-menopausal women with previous or current diagnosis of breast cancer compared to women without breast cancer (25). This is consistent with the data of this study.
fT4 levels within study population.
TRAK values within study population.
Thyroid dysfunction (especially hypothyroidism) seems to appear during long-term follow-up of breast cancer patients (26). The cumulative incidence of (subclinical) hypothyroidism was about 50% after 20 years' follow-up (27, 28). Multiple therapies (chemotherapy, radiation and anti-hormonal treatment) may influence the development of thyroid dysfunction via disturbances of the (auto-)immune system (13-16), therefore this study was designed to take place before any treatment regime was started for each individual patient.
Breast cancer patients showed the highest mean concentrations of TRAK antibodies, differing significantly from women with benign tumours, although only 2 patients showed pathological levels. In addition, breast cancer patients had the highest concentrations of TPO and the lowest levels of TG antibodies. Many authors describe a high prevalence of TPO antibodies in breast cancer patients (5, 6, 9, 10). The prevalence of TPO antibodies in the group of breast cancer patients of this study was only 9%. Contrary to other studies (6, 24), this study was not able to demonstrate significant differences in TPO antibodies between breast cancer patients and patients with benign tumours or controls.
In contrast to other studies, this study focused on Tis patients as part of the study group. Tis patients showed significantly higher fT3 levels than healthy controls. Although the Tis group only consisted of a small study population, the Authors do not consider that more details on the pathophysiological input of thyroid function in breast cancer growth can be reached through this specific patient group. Therefore, ongoing studies of our group focus on thyroid function in Tis and breast cancer patients.
This study did not support recent findings of a higher incidence of thyroid disorders such as hypothyroidism, hyperthyroidism or autoimmune thyroiditis (Grave's disease, Hashimoto thyroiditis) (9, 12) in breast cancer patients or patients with benign breast tumours. However, these data must be confirmed in large patient cohorts and long duration follow-up. Further studies are underway to specify the role of thyroid hormones in breast cancer patients and to highlight possible influences on cancer outgrowth and progression.
Footnotes
- Received August 19, 2009.
- Accepted March 15, 2010.
- Copyright© 2010 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Exogenous Thyroid Hormone Is Associated with Shortened Survival and Upregulation of High-Risk Gene Expression Profiles in Steroid Receptor-Positive Breast Cancers
- Thyroid Hormones, Silencing Mediator for Retinoid and Thyroid Receptors and Prognosis in Primary Breast Cancer
- Thyroid Hormones and Vitamin D in Patients with Breast Cancer with Mutations in BRCA1 or BRCA2 Genes
- MECHANISMS IN ENDOCRINOLOGY: Primary HT and risk for breast cancer: a systematic review and meta-analysis