


Abstract
Many environmental compounds with oestrogenic activity are measurable in the human breast and oestrogen is a known factor in breast cancer development. Exposure to environmental oestrogens occurs through diet, household products and cosmetics, but concentrations of single compounds in breast tissue are generally lower than needed for assayable oestrogenic responses. Results presented here and elsewhere demonstrate that in combination, chemicals can give oestrogenic responses at lower concentrations, which suggests that in the breast, low doses of many compounds could sum to give a significant oestrogenic stimulus. Updated incidence figures show a continued disproportionate incidence of breast cancer in Britain in the upper outer quadrant of the breast which is also the region to which multiple cosmetic chemicals are applied. Conclusion: If exposure to complex mixtures of oestrogenic chemicals in consumer products is a factor in breast cancer development, then a strategy for breast cancer prevention could become possible.
- Environmental oestrogens
- breast cancer
- cosmetics
- antiperspirant
- deodorant
- paraben
- aluminium
- organochlorine
- phytoestrogen
- breast cysts
- review
Breast cancer is not a new condition but has formed a component of mankind's struggle against disease since ancient times. Egyptian papyrus scrolls dating from 3000 BC describe tumours of the breast, and cases of breast cancer were recorded in ancient Greece by Hippocrates (460-375BC) (1). However, the unprecedented worldwide increase in incidence over the past 50 years has turned this disease into the most common cancer of women in much of the Western world (2, 3). In England and Wales alone, breast cancer incidence has nearly doubled over the past 30 years from 21,446 new cases recorded in 1979 (84.5 per 100,000 population) to 40,452 new cases recorded in 2006 (145.6 per 100,000 population) (4).
Along with the rising incidence, it seems that the biology of breast cancer may also be altering. In the UK in the early 1970s, fewer than 10% of breast tumours were ductal, lobular or medullary tumours but by the end of the 1990s, this percentage had risen to 75%, with ductal carcinomas alone comprising 60% of all breast cancer cases (5). In addition, the relative proportion of breast tumours which contain oestrogen receptors (ER) and are hormone responsive has also been reported to be rising, not only in the UK (6, 7) but also in France (8) and the USA (9, 10). Another notable change has been in the relative rise of breast cancer in the UK amongst affluent women which cannot be attributed solely to higher compliance with screening and which is in striking contrast to other types of cancer where the deprivation gap continues to widen (5).
Although many risk factors have been identified for breast cancer, the underlying causes of the rising incidence remain to be identified. Loss of function of breast cancer susceptibility genes such as BRCA1 and BRCA2 which function in DNA repair processes can predispose to breast cancer development in about 5% of cases (11). Lifestyle factors such as smoking, alcohol, radiation exposure and diet have also been identified as components of risk (2, 3). However, the main influence in development of breast cancer remains hormonal and, in particular, related to lifetime exposure to oestrogen (2, 3). Epidemiological evidence has established links between breast cancer development and exposure to physiological oestrogens through early onset of menarche, late menopause, nulliparity, late age of first pregnancy, practices of breast feeding (2, 3), and exposure to pharmacological oestrogens through use of the contraceptive pill (12) and hormone replacement therapy (13, 14). In addition to the epidemiological evidence, the ability of oestrogen to drive the growth of breast tumours in vivo is well established in both clinical studies and animal models, and oestrogen action on growth of breast cancer cells in cell culture systems in vitro has been extensively documented (15, 16). This involvement of oestrogen in the progression of breast cancer is the basis for the successful use of endocrine therapy as a targeted treatment for breast cancer (17).
The case for a Contributory Role of Environmental Oestrogens in Breast Cancer
Since epidemiological, experimental and clinical studies leave no doubt that oestrogen is involved in the development and progression of breast cancer, the ability of environmental chemicals with oestrogenic properties to drive the development and growth of breast tumours is also worthy of serious consideration. Over the past 15 years, it has become evident that pollutant chemicals with oestrogenic properties, which are present in the environment, can impact on endocrine health of wildlife, influencing reproduction, particularly in aquatic populations (18-21). However, it remains to be determined as to whether the oestrogenic properties of these same chemicals can impact on human health and specifically on breast cancer (18, 22). Many of these environmental oestrogenic chemicals can be measured in the human breast, and although their presence does not of itself imply any causality, it does confirm that many such chemicals are now ubiquitously present in human breast tissue (22).
Environmental oestrogens may enter the human breast from dietary consumption of residues of organochlorine pesticides or polychlorinated biphenyls (PCBs) (18, 23-25) and of phytoestrogens (26), or from exposure in the domestic environment to bisphenol A (27) and phthalates (28, 29) of plastics, alkyl phenols (30) of detergents, or polybrominated diphenylethers (PBDEs) (31-33) in soft furnishings. Topical application of cosmetic chemicals with oestrogenic properties provides another exposure route (22, 34-36) and evidence for the presence of cosmetic chemicals with oestrogenic activity in the human breast is summarised in Table I (37-78). Studies over the past 10-15 years have fallen short of linking any one chemical to causation of breast cancer but the environmental reality is that the human breast is exposed not to one but to a multitude of oestrogenic chemicals (79, 80), that variations in lifestyle will result in individuals being exposed to different mixtures, and that alterations may occur in timing of exposure which may be critical for breast cancer, which can begin many years before symptoms appear (81).
Mechanisms of Action of Environmental Oestrogens
Within the cell, oestrogens act by binding to intracellular oestrogen receptors (ERα and ERβ) which function as ligand-activated transcription factors (82). Binding of an oestrogenic compound results in release of associated heat-shock proteins, dimerisation of receptor ligand complexes, binding of the dimers to oestrogen response elements in the DNA and transactivation of gene expression. Global gene expression analysis using microarrays has shown that oestradiol regulates the expression of hundreds of genes (83, 84), and whilst environmental oestrogens can regulate the expression of some genes in a similar manner, the global patterns of gene expression with different environmental oestrogens can vary (84). The realisation that so many environmental compounds can interact with specific biological receptors has challenged concepts of classical toxicology because this mode of action allows for compounds to act at lower concentrations and for effects to be targeted via the genome to influence patterns of gene expression. Although this has been the most studied mode of action, environmental oestrogens may also influence non-genomic pathways of oestrogen action (85) and synthesis or bioavailability of physiological oestrogens (86).
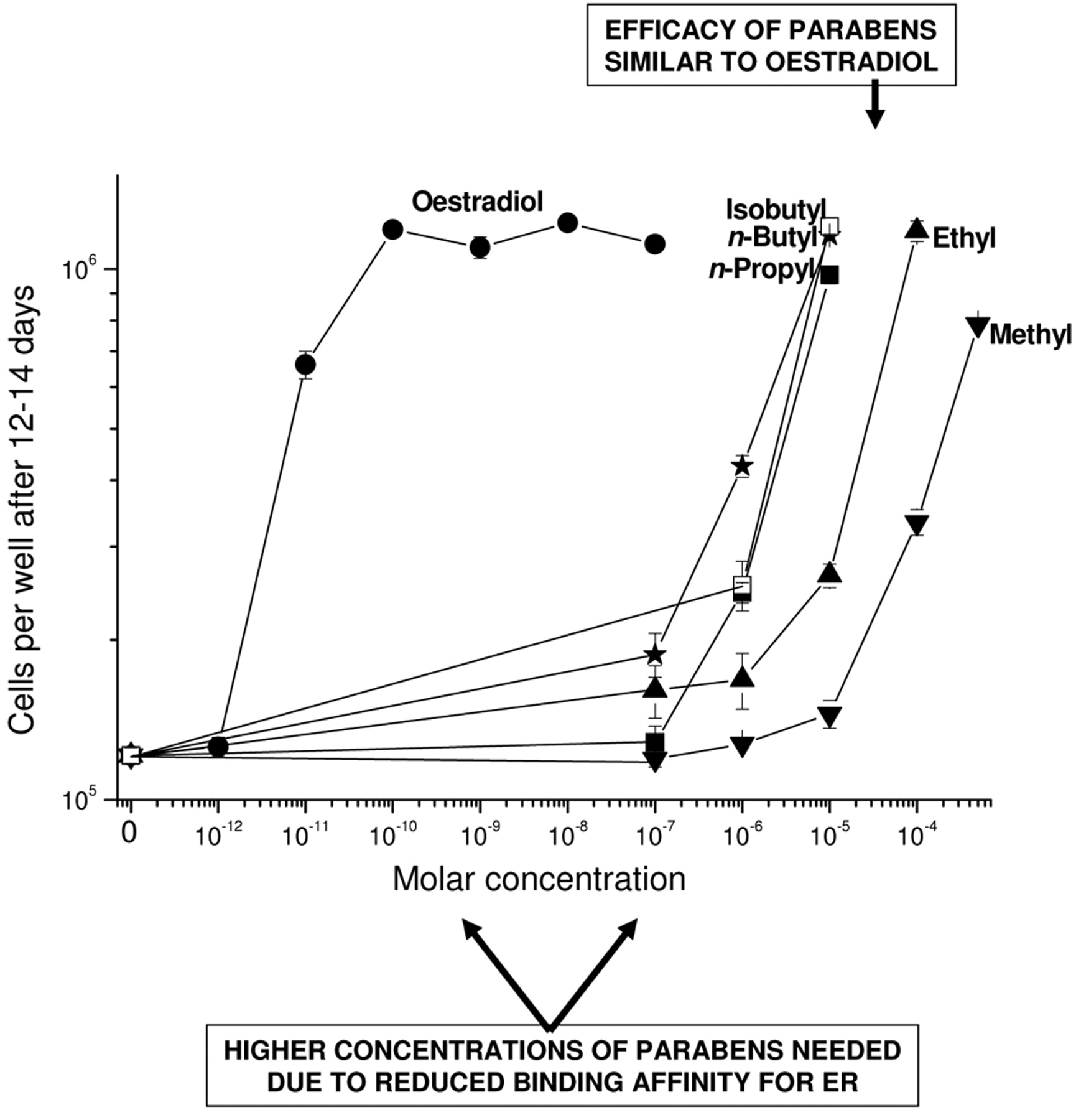
Many studies have now reported on the ability of a range of environmental compounds to competitively bind to oestrogen receptors, to transactivate gene expression and to influence the growth of cells dependent on oestrogen for their growth (87). Animal models have shown that oestrogenic actions can also be found in vivo, most noteably in increasing uterine weight in the immature rodent (88). One universal observation has been that such compounds bind more weakly to oestrogen receptors than do physiological oestrogens and in competitive binding assays, higher concentrations of the environmental compounds are invariably needed compared with 17β-oestradiol (89). This weaker binding affinity has resulted in such compounds being labelled and even dismissed as ‘weak’ oestrogens. However, when ligand efficacy is considered as well as ligand binding affinity (90), the efficacy of many of these compounds is not correspondingly low and they can give the same magnitude of response as 17β-oestradiol when sufficient concentration is present (41). Figure 1 shows the growth of MCF7 human breast cancer cells in culture with five different alkyl esters of p-hydroxybenzoic acid (parabens) compared to 17β-oestradiol (91, 92). The lower ER-binding affinity of parabens compared with 17β-oestradiol (91, 92) necessitates higher concentrations of the parabens to be added to the growth assay but when sufficient concentrations are present, growth occurs to a similar extent as with 17β-oestradiol. In this context then, the designation of such compounds as ‘weak’ oestrogens is inappropriate and the relevant consideration becomes the concentration of the compound present.
Evidence for the presence of cosmetic chemicals with oestrogenic activity in the human breast.
Whilst the quantity, chemical combinations and metabolism/clearance are all important components, the timing of exposure may also be relevant. One unresolved issue remains the potential for an impact of oestrogenic compounds in the presence of physiological oestrogens. In this context, the impact might be expected to be more significant at times when physiological oestrogens are at their lowest levels, which would implicate life stages prior to puberty, after menopause or at times of the monthly menstrual cycle when oestrogens levels fall, and there is evidence for concern of an adverse consequence of oestrogenic overload at all these times. There is evidence that the breast may be especially susceptible to carcinogenesis before puberty (81), which is substantiated in survivors of the atomic bomb in Japan in 1945 where the greatest risk of subsequent breast cancer development was in girls who were prepubertal at that time (93). Furthermore, the increased incidence of breast cancer not only in mothers who were exposed to diethylstilboestrol during pregnancy (94), but also in their daughters (95) demonstrates a link between breast cancer development and exposure, even in utero, to a potent synthetic oestrogen. However, since the majority of symptoms of breast cancer only become apparent after the age of 50 (2, 3), exposure to chemicals after the menopause could also be significant. This is the time of greatest body burden from bioaccumulated chemicals and the breast is known to be sensitive to oestrogen at this stage from the impact of hormone replacement therapy (HRT) on breast cancer incidence (13) and the influence of phytoestrogen-containing plant products on menopausal symptoms, including breast changes (26). Furthermore, the finding of higher levels of ER in postmenopausal than premenopausal breast tumours (96) could result in sensitivity to lower concentrations of oestrogenic chemicals at that time because it is already known that higher levels of ER in breast cancer cells can result in oestrogen hypersensitivity (97). That there can also be an impact of oestrogenic overload between puberty and menopause is also implicated from studies on oral contraceptives and breast cancer risk (12).

Efficacy of parabens compared with 17β-oestradiol on the growth of MCF7 human breast cancer cells in monolayer culture. Cells were grown as described elsewhere (91, 92) in phenol red-free RPMI-1640 medium with 5% dextran-charcoal stripped foetal calf serum with the indicated concentrations of 17β-oestradiol, methylparaben, ethylparaben, n-propylparaben, n-butylparaben or isobutylparaben. Error bars are the standard error of triplicate wells.
Environmental Oestrogenic Organochlorine Compounds
Many man-made organochlorine compounds have been released into the environment from agricultural spraying (such as DDT, dieldrin, lindane), or as byproducts of industrial processes (PCBs) and waste disposal (dioxins). Many of these compounds have been shown to act as oestrogen-mimicking chemicals, are persistent in the environment and due to their lipophilic properties can pass up the food chain dissolved in animal fat (18, 98, 99). Although human exposure to these compounds is only at low levels in the diet, many of these compounds are not readily metabolised and can accumulate over time in fatty tissues of the body. The breast has a particularly high fat content and the epithelial cells, which are the main target for cancer, are embedded in a fatty stroma, providing an opportunity for concentration of these lipophilic oestrogenic pollutants in the vicinity of the target cells for breast cancer. Although these persistent organochlorine pollutants (POPs) have been measured in many independent studies in the ng/g tissue range in both human breast adipose tissue and in human breast milk (reviewed in 18 and 22), it remains unclear as to whether their presence alone in the breast is sufficient for adverse consequences. Several studies have tried to address the question by comparing measured levels of compounds in breast cancer tissue either with those in adjacent non-affected breast tissue from the same patient, or with breast tissue from matched patients without breast cancer (18, 22). Such studies have many inherent problems which have resulted in rather varied conclusions without any general overall consensus emerging. A main problem is that since breast cancer may start many years before symptoms appear, measurement of chemical load in those with breast cancer may not be representative of the chemical load at the time of carcinogenesis. A second problem is that most of the larger studies with statistical power have measured chemical concentrations in blood serum and this may not reflect levels in the breast, or breast cells, neither in every individual nor for every chemical (22, 100, 101). Thirdly, the absolute level of any chemical may not be the sole determinant but only one component influenced by individual variations in susceptibility and genetic background. Finally, since the environmental reality is that the breast is exposed to multiple not single chemicals, it may be that consideration needs to be given to the overall mixture of chemicals within a single breast (80). Similar oestrogenic loads may be generated through exposure to mixtures of different oestrogenic chemicals, and similar carcinogenic actions may be generated through exposure to chemicals with varied mechanisms. Since breast carcinogenesis may be stochastic, it may not be that higher levels of chemicals are even needed, but simply that the presence of chemicals in the breast gives rise to adverse reactions in a stochastic manner within a field of cells made susceptible through the consequential actions of the chemical mixture present (102). In this context, it could be concluded as significant that a wide range of organochlorine pollutant chemicals have been measured in the human breast but the lack of a global consensus in differences between chemical loads of cancerous and non-cancerous tissues cannot be taken to imply a lack of mechanistic involvement.
Environmental Oestrogens from the Domestic Environment
The inclusion of chemical components with oestrogenic activity in consumer products used widely in the domestic environment points to the need for a heightened awareness of the potential for exposure to environmental oestrogens on a daily basis in the home. Plastics are used ubiquitously in home life and provide a source of exposure to bisphenol A and phthalates for all age groups. Bisphenol A has oestrogenic properties (103), has been shown to cause mammary hyperplasia in animals (104) and has been measured in human milk (27). The oestrogenic properties of phthalates (70-72) and their adverse effects on male reproduction in rodents (105) have established them as endocrine disruptors and several phthalates have also been measured in human milk (28, 29). The ubiquitous use of PBDEs as flame retardants in soft furnishings has resulted in body burdens of these chemicals across exposed human populations. PBDEs also possess oestrogenic properties (106) and have been measured in human milk (31-33).
Phytoestrogens in the Diet
Several flavonoids and lignans occurring naturally in plants have also been shown to possess oestrogenic activity (26, 77) and consumption of certain phytoestrogen-containing plant supplements can have beneficial effects in alleviating menopausal symptoms (26). However, the mechanisms of phytoestrogen action in breast cancer development remain to be resolved. The relatively higher consumption of phytoestrogens by Asian women compared with Western women and the lower incidence of breast cancer in Asia compared with the West (107) has posed the question of whether plant products might actually protect against breast cancer despite the presence of phytoestrogens, some of which have relatively high binding affinity for the ER (77). Animal studies have suggested that phytoestrogen consumption at a young age may be protective against breast cancer development whilst in animals with breast tumours, phytoestrogens may increase tumour growth (108, 109). Human dietary intervention studies have also suggested that phytoestrogen consumption would not be beneficial in breast cancer patients (110). In view of the many Western women now opting for plant-based supplements rather than HRT in the menopausal years, more research into the effects of these complex plant extracts on breast cancer risk and development is justified.
Oestrogenic Components of Cosmetics
An alternative route for exposure to oestrogenic chemicals is through the topical application of a variety of cosmetic products containing oestrogenic chemicals (22, 34-36, 41, 42, 111) (Table I). Many of these cosmetic products are applied on and around the human breast on a daily basis, often multiple times a day, and under current cultural pressures are used with increasing frequency and quantity. Breast exposure to a range of cosmetic oestrogens can occur not only through use of antiperspirant/deodorant products but also body sprays/lotions, moisturising creams, breast firming/enhancing creams and suncare products. These cosmetics are left on the skin of the breast region, allowing not only for continuous direct dermal exposure but also consequent absorption into underlying tissues (22, 34-36, 41, 42, 111). Since shaving can create abrasions in the skin, current practices of cosmetic application after shaving may further increase the likelihood of chemical components entering underlying tissues. The extent to which chemicals entering tissues through dermal absorption can escape metabolism remains unknown, but they would certainly evade the systemic metabolism to which orally derived chemicals would be subjected (41, 42, 111). With increasing quantities reapplied multiple times a day, chemical absorption may not occur through normal physiological mechanisms associated with the vasculature and lymphatic drainage of the breast region (22, 34-36, 41, 42, 111). The range of different consumer products available and the diversity in practices of use provide numerous possibilities for cancer to arise through quantity applied, specific product formulations, mixtures of products applied, or individual susceptibility to different components or mixtures. The increasing useage by some young children and babies could also provide for variations in cancer development later in life.
Dermal Absorption of Topically Applied Cosmetic Chemicals with Oestrogenic Properties
The belief that chemical components of cosmetics cannot be absorbed is no longer valid because many of the component chemicals have been measured in the human body and some absorbed components have been shown to have a physiological/endocrine impact. Administration of HRT by skin patches relies on the ability of components to be absorbed through the skin and to influence menopausal symptoms, but an equal consideration needs to be given to daily dermal application of cosmetic products with oestrogenic components. The case of the Mortician's Mystery published in the New England Journal of Medicine in 1988 is a reminder that oestrogenic components of cosmetic products (in this case, embalming creams) applied to the hands cannot only be absorbed dermally but have a consequent impact on endocrine function, including undesired growth of breast tissue in a man (112). Many other studies have also reported endocrine-disrupting effects of oestrogenic chemicals of cosmetics (36), and more recently, thelarche in a 36-month girl from exposure to her mother's shampoo (113), youth enhancement in a 46-year-old (presenting with ER-positive breast cancer) after 4 weeks of use of a skin moisturiser containing oestrogens (74) and abnormal genital bleeding in a 93-year-old (presenting with breast cancer) after exposure to an ethynylestradiol-containing body cream (75). In this context, natural products are also not without effect and cosmetics containing lavender and tea-tree oils have been shown to expand breast tissue in men giving rise to gynecomastia (78).
Many oestrogenic chemical components used in cosmetic products have now been measured as being present in the human breast (Table I). However, the ubiquitous use of many of these chemicals in a wide range of consumer products makes it impossible to know the specific origin of the chemicals as measured in any one human breast. Parabens are added as preservatives to cosmetic products (114) and have been shown to possess oestrogenic activity (41-42), to be absorbed in humans from dermal absorption of cosmetic cream (44-45) and have been measured in human breast tissue at an average concentration of 20 ng/g tissue (43). Aluminium salts used as the active antiperspirant agent in cosmetics (115) have been shown to be absorbed through intact skin of the human underarm (39) and have been linked to adverse physiological effects (extreme fatigue and bone pain) following absorption (40). Aluminium is a metalloestrogen (37) and aluminium levels measured in human breast tissue have been shown to be higher in outer than inner regions of the breast, which might be expected if resulting from application to the underarm region (38). Chemicals which absorb UV radiation are added to cosmetics to prevent skin damage from UV light in suncare products and to prevent product spoilage by UV radiation. Many of these UV filters have been shown to possess oestrogenic properties (49-53), to be absorbed in humans from dermal application of cosmetic cream (55-56) and have been measured in human milk (54). Synthetic musks and other organic chemicals are added as fragrance and fragrance fixers in cosmetics. Both polycyclic musks (57-61) and nitromusks (61) have been shown to possess oestrogenic activity, as have benzyl salicylate, benzyl benzoate and butylphenyl methylpropional (64). Some have been measured in human milk (62-63). Phthalate esters, used as plasticizers and moisturisers in cosmetics, have been shown to be oestrogenic (70-72), to be absorbed in humans from dermal application of cosmetic cream (44-45, 73) and have been measured in human milk (28, 29). Triclosan is an effective deodorant and preservative used in cosmetics with oestrogenic properties (46) and measurable in human milk (47-48).
The reported measurements of so many of these chemicals in human breast tissue or human milk demonstrates that chemical components used in cosmetics are entering the human breast but it remains unknown as to whether they originate solely from cosmetics or also from other consumer products and whether they are present from continuous use or are accumulated from long-term exposure. Furthermore, whilst it is evident that their presence serves no useful function, it remains to be determined whether or not there is any causal relationship of individual or combinations of chemicals with development of breast cancer, taking into consideration the same limitations of chemical measurements as was outlined for the POPs.

Trend in proportional annual incidence of female breast cancer in the upper outer quadrant (UOQ) of the breast from 1979 to 2006 in England and Wales. Each point represents the ratio of recorded incidence in the UOQ to the total incidence recorded in that year with site-specific information. (A total of 302,793 returns were made with site-specific information between 1979 and 2006.) Linear regression analysis was used to calculate the line of best fit (correlation coefficient R was 0.71 with a standard deviation of 0.01 (p<0.0001)). This updates to 2006 the data which were published previously for 1979 to 2000 (116).
The Disproportionate Incidence of Breast Cancer in the Upper Outer Quadrant, the Region of Underarm Cosmetic Application
One of the most evident anomalies of breast cancer incidence is the disproportionate number of tumours originating in the upper outer quadrant (UOQ) of the breast. This has been reported in clinical studies dating back decades, but the published disproportionality appears to rise chronologically from around 31% in reports of the 1920s up to 61% in reports in the 1990s (116). In order to determine whether this was a function of time or a reflection of different study populations, the quadrant incidence of breast cancer was studied in two independent single populations using recorded quadrant incidence in England and Wales and independent recorded values in Scotland. Notwithstanding the incomplete nature of national data, 212,677 returns were made with site-specific information between 1979 and 2000 in England and Wales, and over this 21-year time span, the incidence of breast cancer in the UOQ relative to total site-specific returns had risen disproportionally from 47.9% in 1979 to 53.3% in 2000 and had done so on a linear annual basis (correlation coefficient R of 0.713 with a standard deviation of the fit of ±0.014 and a p-value from the F distribution of <0.001) (116). Independent data collection from Scotland gave 17,911 returns with site-specific information and these data revealed also an increase in the disproportionality of UOQ returns, from 38.3% in 1980 to 54.7% in 2001 which was also increasing linearly on an annual basis (correlation coefficient R of 0.800 with a standard deviation of the fit of ±0.028 and a p-value from the F distribution of <0.0001) (116). Since recordings have now been collated for up to 2006 from these national offices, updated analysis has been performed to extend the published values (116) up to 2006, and the results are shown in Figure 2 for England and Wales and Figure 3 for Scotland. Within the returns with site-specific information, the incidence of breast cancer in the UOQ relative to total site-specific returns has remained fairly level in England and Wales between 2000 and 2006, remaining at 53.3% (Figure 2), but in Scotland, there was a further increase in UOQ incidence to 57.0% in 2006 (Figure 3).

Trend in proportional annual incidence of female breast cancer in the upper outer quadrant (UOQ) of the breast from 1980 to 2006 in Scotland. Each point represents the ratio of recorded incidence in the UOQ to the total incidence recorded in that year with site-specific information. (A total of 25,259 returns were made with site-specific information between 1980 and 2006.) Linear regression analysis was used to calculate the line of best fit (correlation coefficient R was 0.78 with a standard deviation of 0.03 (p<0.0001)). This updates to 2006 the data for1980 to 2001 which were published previously (116).
The current explanation for more breast tumours starting in the UOQ is that this region of the breast contains a greater proportion of epithelial tissue which is the target tissue for most cases of breast cancer. However, this anatomical explanation alone is inadequate in accounting for annual increases in the incidence of breast cancer in the UOQ (116). Such an increase is, however, compatible with the increasing application to the adjacent underarm region of cosmetic products containing chemical components with oestrogenic and/or other adverse properties (22, 34-35).

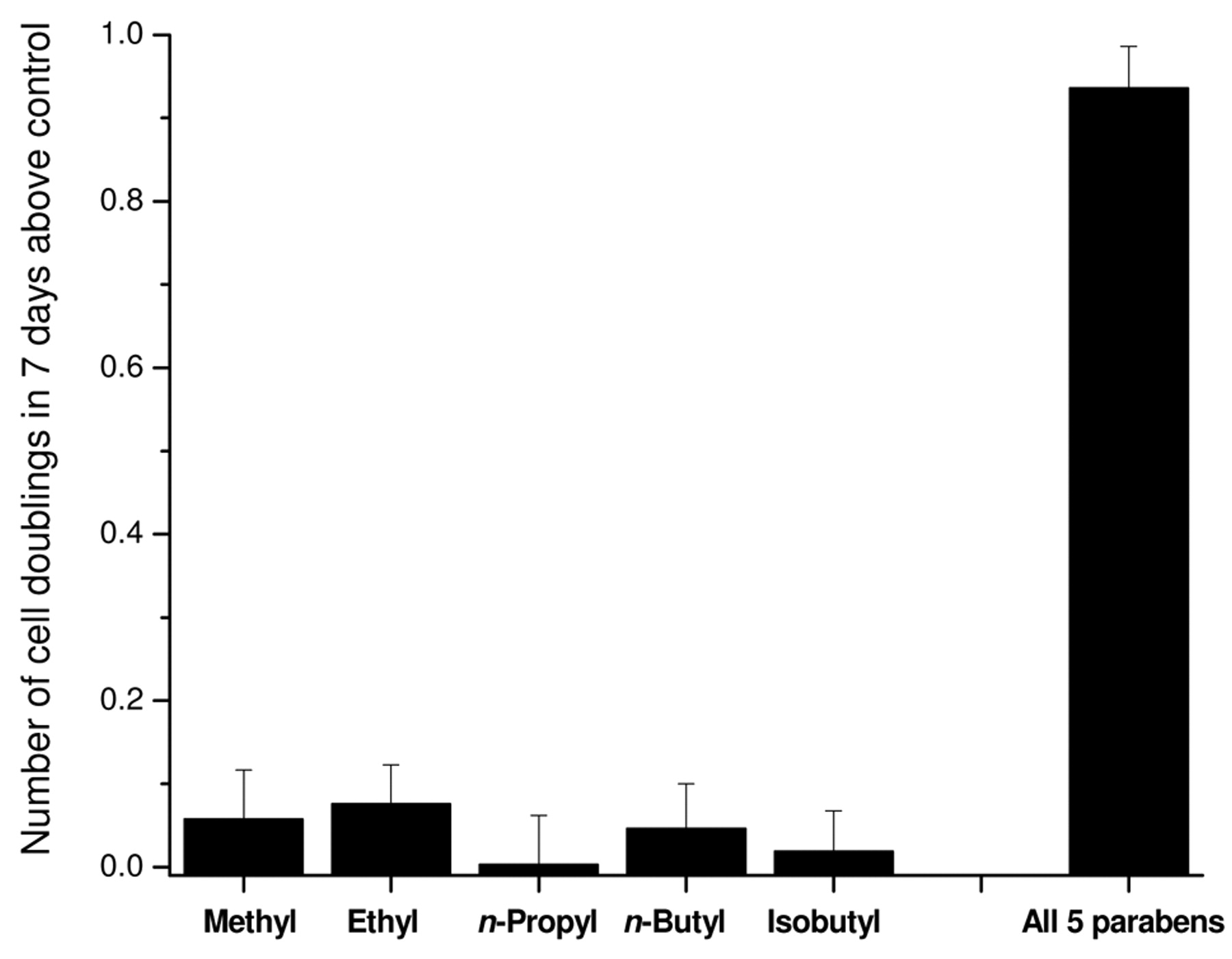
Additive effects on growth of MCF-7 human breast cancer cells when parabens are combined at no-observed effect concentrations (NOEC). Cells were grown as described elsewhere (91, 92) and growth presented as the number of cell doublings above the control value for either individually methylparaben (2×10−5M), ethylparaben (8×10−7M), n-propylparaben (2×10−7M), n-butylparaben (2×10−7M) or isobutylparaben (10-7M) or all five parabens in combination at these same concentrations.
Cosmetic Chemicals and Benign Breast Disease
Although cancer is the main concern, it actually only represents about 5% of clinical abnormalities of the human breast, with benign conditions such as breast cysts and fibroadenomas being the most common abnormalities (117). The reasons for such a high incidence of benign breast conditions remain unknown but it is noteable that the most common site of occurrence of breast cysts and fibroadenomas is also the UOQ (117). Although these benign conditions are not life threatening, they do entail invasive procedures and create anxiety, and in some cases may be indicative of an increased risk of subsequent cancer development (118-119).
It has been suggested previously that excessive antiperspirant use in the underarm region might provide an explanation for the disproportionate incidence of breast cysts in the UOQ of the breast (22, 35). Since antiperspirant aluminium salts are designed to prevent perspiration by blocking underarm sweat ducts (115) and breast cysts arise from blockage of breast ducts in the adjacent area of the body (117), it is possible that breast cysts might also arise from antiperspirant use if sufficient of the salts are absorbed over a long period of useage (22, 35). If such an association exists, then it might be expected that aluminium would be measurable at elevated levels in the cyst fluids. The recent measurement of higher levels of aluminium particularly in type 1 human breast cyst fluids (median 150 μg/l; n=27) compared with human serum (6 μg/l; n=30) or human milk (25 μg/l; n=45) now warrants further investigation into a link between antiperspirant use and development of gross cystic breast disease (120).
Evaluation of Long-term Low-dose Exposure to Multiple Oestrogenic Chemicals
Most assessments of the potential for environmental oestrogens to impact on breast cancer development have tended to be limited to consideration of single oestrogenic compounds in isolation, and in general have concluded that levels of single compounds measured in the human breast are below the levels needed for effects in assay systems. Given the real-life situation of the many chemicals now known to be present in the human breast (22, 41), it is likely that it will not be the concentration of any one chemical which is relevant but the total oestrogenic load imposed by all the chemicals present in any one breast at any one time. Since different lifestyles and consumer choices will inevitably result in individual variations in the composition of the mixtures of chemicals present, the total oestrogenic load must be considered rather than the specific individual components in isolation.
Experimental data are beginning to demonstrate that multiple oestrogenic chemicals present together can add up to give measurable oestrogenic responses at concentrations where each alone would have been ineffective (121), which implies that low-dose exposure to multiple oestrogenic chemicals can no longer be dismissed as insignificant (80). Other studies have shown that increasing the time of experimental assays can also allow for oestrogenic responses to be observed which would not be seen in the short term (46, 64), which is highly relevant in environmental situations where chemicals are not cleared quickly from the body, or where there is a source of continued exposure to the chemicals. Measurement of parabens in archival human breast cancer tissue samples from the 1980s showed that levels of individual parabens were present at below the level required for maximal effect in experimental models (43). However, further experimental work in cell culture has shown that lower concentrations of parabens can give measureable oestrogenic effects on growth of human breast cancer cells when acting in combination (Figure 4). Since similar effects have been observed when combining other cosmetic chemicals with oestrogenic activity (52, 53) and indeed with other xenoestrogens (121-122), the question arises as to how low a concentration there would need to be of individual cosmetic oestrogenic chemical residues for there to be no measurable effect when considering tens or even hundreds of residues that might be present in a human breast. The ability to carry out the required risk assessments for such evaluation remains limited, however, by the lack of information concerning profiles of overall chemical load within individual human breasts.
Genotoxic Activity of Environmental Oestrogens
Although oestrogen is established as a factor in the growth and progression of primary and metastasic breast cancer cells (15, 16), the potential for genotoxic actions of oestrogen to influence initiating events in carcinogenesis is also now recognised (123-124) and some environmental oestrogens such as the organochlorine DDT (125) and bisphenol A (126) have been linked to breast carcinogenesis. The clinical report that increased levels of genomic instability can be measured in outer regions of histologically normal breast tissue (127) suggests that the breast is not exposed evenly to genotoxic insults. Instability of the genome can contribute genetic changes that drive carcinogenesis and a region where genetic changes are greater might be expected to predispose to an increase in development of cancer (102). This would be consistent with the disproportionate incidence of breast cancer in the UOQ of the breast (see earlier) but poses a question as to the origin of such an asymmetric genotoxicity. Unless physiological lymphatic or blood circulation predisposes to genotoxic compounds accumulating in the outer regions of the breast, the source of the genotoxicity would be likely to be non-systemic and result from application of components to outer regions of the breast. In this context, it is plausible that an explanation might reside in the absorption of genotoxic cosmetic chemicals applied to the underarm region. Aluminium has a known genotoxic profile (128-130) and breast exposure from use of aluminium-based antiperspirant salts is high (115).
Inheritance of reduced ability to repair DNA due to the loss of function of tumour suppressor genes such as BRCA1 and BRCA2 can predispose to early-age breast cancer (11). However, the reported increasing penetrance of these genes in Iceland has shown that underlying mechanisms of susceptibility have an environmental as well as a genetic component (131). Although it is possible that breast cancer arises in these susceptible women from an inability to repair random replication errors, it is also possible that there could be increased susceptibility to DNA damage from genotoxic pollutant chemicals which enter the human breast, including cosmetic chemicals from excessive use of underarm products.
Environmental Oestrogens and Endocrine Therapy
Endocrine therapy relies on the ability to reduce oestrogen action in the body through either the inhibition of oestrogen synthesis with aromatase inhibitors, or the antagonism of oestrogen action with antioestrogens (17). However, little attention has been paid to the potential interference in effectiveness of this therapy from the presence of environmental oestrogens entering the breast (22). Theoretically it would seem to be counterproductive to reduce oestrogen synthesis with aromatase inhibitors on the one hand, and yet at the same time to allow entry to the breast of a range of environmental oestrogenic chemicals. Whilst it may be difficult to avoid the oestrogenic chemicals entering as pollutant residues in the diet, the decision to apply oestrogenically active compounds in cosmetic products lies entirely with the user. Perhaps women undergoing endocrine therapy, especially with aromatase inhibitors, should be encouraged to stop using cosmetic products, especially those specifically advertising youth-enhancing or breast-firming properties which are likely to contain oestrogens (22, 74). Many women are aware of the oestrogenic properties of plant products such as soy beans and black cohosh because of their use in countering menopausal symptoms, but they may be less aware of the potent oestrogenic properties of some cosmetics (74).
The Need for Further Research
Research effort is demonstrating that increasing numbers of environmental compounds with oestrogenic properties can be measured in human breast tissues, but at the current time it remains uncertain as to whether or not there is any causal relationship between the presence of any such compounds in the human breast and the development of breast cancer. The established role of oestrogen in breast cancer development (2, 3, 15, 16) and the rising incidence of oestrogen-responsive breast cancer (6-10) makes this an important area of future international research investigation, but exposure to so many different environmental sources through varied lifestyle choices makes it a daunting task to try to devise ways of investigating causality. The realisation that multiple chemicals can act together at lower doses over the longer term has no doubt provided an even greater level of complexity. Without doubt, there is a data gap in information about the overall chemical burden in individual human breasts and more detailed knowledge of the concentrations of oestrogenic chemicals present would enable risk assessment to begin the necessary task of considering complex mixtures of chemicals each at relevant concentrations and relevant combinations as found in the human breast.
The possible role in breast cancer of cosmetic chemicals applied to the underarm and breast area also has potential for further testing. The disproportionate incidence of breast cancer in the UOQ (22, 34-35, 116, 117) and the finding of regions of genomic instability in outer quadrants of histologically normal breast (127) are both consistent with a causal relationship to the application of underarm cosmetic chemicals. The unexplained rise in breast cancer amongst affluent women in the UK is also in striking contrast to other types of cancer where the deprivation gap is widening (5) and whilst this might be explained by many lifestyle practices of affluence, increased cosmetic use would certainly be consistent with an affluent lifestyle. To date, there are only two epidemiological studies directly addressing the issue of underarm cosmetic use and breast cancer (132-133). Since the two studies come to opposing conclusions and both have their limitations, further investigations are warranted. Although individual chemicals in cosmetic products will have been tested according to current safety guidelines, such testing cannot consider long-term consequences and so the effect of widespread and lifetime useage of complex mixtures of these chemicals by large proportions of people across the world remains untested. It is inevitable that use by such a wide proportion of the population in different parts of the world will result in exposure of people with varying susceptibilities, and different cultural practices may also lead to varied outcomes. The advertising pressures to use more of these products raises questions of acceptable maximal limits not only for adults but for pregnant women and for young children and babies. If use of these products is a factor in breast cancer or benign breast diseases such as cyst formation, then options for prevention should become possible. It would be interesting to determine breast cyst recurrence in women who might opt to cease usage of underarm antiperspirant. It would be interesting to investigate breast cancer development in individuals with loss of BRCA1/BRCA2 who have never used underarm cosmetic products or who might wish to cease usage. It would be useful to test the effect of long-term cosmetic use in an animal model (currently cosmetic testing on animals is not allowed in the UK). Strategies for prevention of breast cancer have been long awaited and rigorous scientific testing of the effects of chemicals with oestrogenic and/or genotoxic (and/or other adverse properties) provides an evidence-based starting point for further research.
Acknowledgements
We would like to thank the Office of National Statistics in London, the Welsh Cancer Intelligence and Surveillance Unit in Cardiff, and the Epidemiology and Statistics Group NHS Scotland in Paisley for collating and supplying data. I (PDD) thank the University of Reading Research Travel Board for financial assistance with travel costs to Kos.
Footnotes
- Received November 20, 2009.
- Revision received February 22, 2010.
- Accepted February 24, 2010.
- Copyright© 2010 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- Abstract
- The case for a Contributory Role of Environmental Oestrogens in Breast Cancer
- Mechanisms of Action of Environmental Oestrogens
- Environmental Oestrogenic Organochlorine Compounds
- Environmental Oestrogens from the Domestic Environment
- Phytoestrogens in the Diet
- Oestrogenic Components of Cosmetics
- Dermal Absorption of Topically Applied Cosmetic Chemicals with Oestrogenic Properties
- The Disproportionate Incidence of Breast Cancer in the Upper Outer Quadrant, the Region of Underarm Cosmetic Application
- Cosmetic Chemicals and Benign Breast Disease
- Evaluation of Long-term Low-dose Exposure to Multiple Oestrogenic Chemicals
- Genotoxic Activity of Environmental Oestrogens
- Environmental Oestrogens and Endocrine Therapy
- The Need for Further Research
- Acknowledgements
- Footnotes
- References
- Figures & Data
- Info & Metrics
Related Articles
Cited By...
- Hypersensitivity and Growth Adaptation of Oestrogen-deprived MCF-7 Human Breast Cancer Cells
- Insight into the mechanisms of action of estrogen receptor {beta} in the breast, prostate, colon, and CNS
- Environmental oestrogens and breast cancer: long-term low-dose effects of mixtures of various chemical combinations