


Abstract
Background: This study investigated the potential of HE4 to predict disease-free survival for patients with breast cancer. Patients and Methods: One hundred and twenty-nine patients with breast cancer underwent surgery from January 2004 to September 2009. Immunohistochemical analysis (IHC) and RT-PCR were used to determine the expression of HE4 which was compared with the clinicopathological factors or prognosis. Results: A total of 71 of 129 cases (55%) were HE4 positive and two cell lines expressed HE4 protein and mRNA. No correlation was found between HE4 expression by IHC and clinicopathological factors; however, lymph node involvement was closely associated with HE4 expression. Five-year disease-free survival in the HE4-positive group (58.6%) was significantly worse than that in the negative group (85.6%, p=0.04). Conclusion: These data showed that HE4 expression is associated with lymph node involvement and is a possible predictive factor of breast cancer recurrence.
Approximately 25-30% of breast cancer patients with negative lymph nodes will develop distant metastases within ten years of surgery (1). In addition, there is a need to find an improved marker to stratify breast cancer patients into different risk groups more accurately than can be achieved with current clinicopathological factors; therefore, low-risk favourable patients can be spared unnecessary treatment, avoiding side-effects and reducing the cost of treatment. Furthermore, it might be possible to separate out high-risk patients and offer them customized (more aggressive) treatment modalities. A new method of gene profiling has recently been provided as a powerful tool for predicting the clinical outcome (2).
Human epididymis 4 (HE4) gene product, also known as whey acidic protein (WAP) four-disulphide core domain protein 2 (WFDC2), was identified as the transcript expressed in the epididymis and respiratory tract (3). HE4 is a member of the WAP domain family and this domain shows 50 well-conserved amino acid motifs. This protein has a variety of functions, such as antiproteinases, leukocyte protease 1 (SLPI) and elafin, which show antibacterial activities and anti-inflammatory effects (4, 5).
As recently reported, HE4 is also expressed in ductal carcinoma of the breast (6); however, the function of this protein in breast cancer remains unclear. In this study, it was hypothesised that the alternative expression of HE4 is associated with breast carcinogenesis or tumour progression. This study therefore investigated the expression of HE4 in breast cancer and the correlation between lymph node metastasis and HE4 expression.
Patients and Methods
Patients and samples. Between January 2004 and September 2009, 129 samples from breast cancer patients who had undergone surgery were obtained from Oita University Hospital (Oita, Japan). The study was approved by the Institutional Review Board of Oita University hospital and all patients gave informed consent. The samples were histologically diagnosed for primary adenocarcinoma of the breast by hematoxylin and eosin (H&E) staining. None of the patients had received radiation therapy or chemotherapy before surgery.
Immunohistochemical analysis. Four micrometer sections were prepared for tissue slides. Antigen retrieval was performed at 121°C for 10 min in an autoclave with citrate buffer (pH6.0) after deparaffinization. Ten percent goat serum (Nichirei, Tokyo, Japan) and 0.5% BSA were used to block nonspecific binding. Staining with polyclonal anti-HE4 antibody (Abcam, Tokyo, Japan) with diluents, 1:20, was performed overnight at 4°C. After reacting with 3% hydrogen peroxide for 10 min at room temperature, polymer anti-rabbit (goat) antibody (K4002; Dako Glostrup, Denmark) for HE4 was applied and incubated for 30 min at room temperature. Negative controls were incubated without the primary antibody, and human normal epididymis was used as a positive control.
Patient characteristics.
The IHC staining grade was evaluated as follows: 0, negative; 1+, weak; 2+, moderate; 3+, strong cytoplasmic staining and the percentage of positive cells (0, 1 (1-24%), 2 (25-49%), 3 (50-74%), and 4 (75-100%)) with discrepancies resolved by consensus. The grades were multiplied to determine the H-score as described in a previous report (6). H-Scores for tumours with multiple cores were averaged. Protein expression was then defined as negative (score=0), weak (1-3), and strong (≥4).
Cell culture. Human breast cancer cells, MCF-7 and BT474, were obtained from the Japanese Collection of Research Bioresources (Tokyo, Japan) and cultured in complete medium containing RPMI-1640 supplemented with penicillin, streptomycin and 10% FCS.
Immunofluorescence microscopy. Cells were harvested and fixed with fixation solution of 4% paraformaldehyde: 0.2% Tween-20 for 10 min and washed with PBS three times. After blocking (normal goat serum 10%) for 30 min at room termperature, cells were incubated with the following primary anti-HE4 (1:100) antibody overnight at 4°C followed by PBS washing three times. Cells were then probed by Alexa A488 (rabbit; Invitrogen, Carlsbad, CA, USA) secondary antibody (1:200) for 30 min at room temperature. Before taking images by a Zeiss inverted confocal microscope LSM 510 (Karl Zeiss, Munich, Germany), propium iodide was applied for double staining.
RNA extraction and RT-PCR. Tissue specimens were frozen immediately with RNA later™ (QIAGEN, Tokyo, Japan) and stored at −80°C until RNA extraction. RNA from tissue samples and cells was prepared using an RNeasy Mini Kit (QIAGEN). cDNA was synthesised from the same quantity of total RNA according to the instruction manual of the Transcriptor First Strand cDNA Kit (Roche Diagnostics GmbH, Mannheim, Germany).
The HE4 gene was amplified by the following primer set: forward: tgtcactcccaatttctgagg, reverse:gtgggctggaaccagatg.
The PCR amplification condition was one cycle at 94°C for 15 min, followed by 35 cycles at 94°C for 1 min, 60°C for 1 min and 72°C for 1 min. GAPDH gene amplification was used as a control.
Statistical analysis. All statistical analysis was performed using SPSS 14.0 (SPSS Japan Inc., Tokyo, Japan). Different variables of the tumours and normal tissues were analysed with the chi-square test or Fisher's exact test. Disease-free and overall survival were analyzed using the Kaplan-Meier method and evaluated by the log-rank test. Significant differences were accepted at p<0.05.
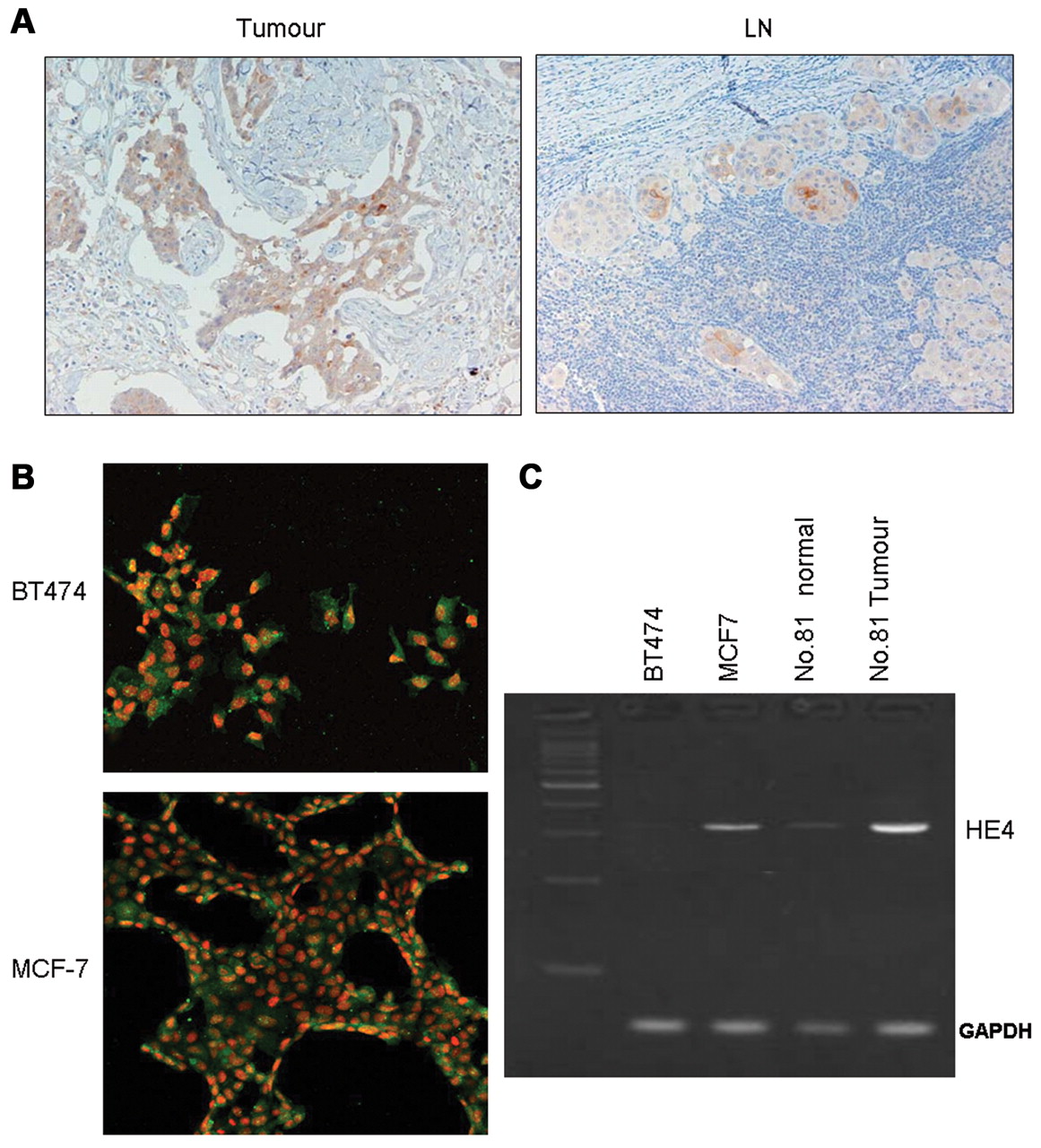
Representative HE4 protein expression in breast cancer by IHC. A: Cytoplasm of cancer cells in both tumour and lymph nodes (LN) was strongly stained (×200). B: Immunofluorescent imaging showed HE4 expression (green) in the cytoplasm of breast cancer cell lines. Propium iodide showed nuclear staining (red). C: Expression of HE4 gene was detected by RT-PCR in human breast cancer cell lines and resected breast cancer specimens. Two cell lines (MCF7 and BT474) were established from breast cancer. No. 81 normal, normal breast tissue from patient No. 81; No. 81 tumor, tumor specimen from same patient.
Results
Relationship between clinicopathological characteristics and HE4 expression by IHC. A total of 71 out of 129 cases (55%) were HE4 positive, and the relationship between the clinicopathological characteristics of breast cancer and HE4 expression was investigated. As shown in Table I, nodal involvement was closely associated with HE4 expression. HE4 expression in node-positive (24 out of 34, 71%) tumors was more frequent than in node-negative (47 of 95, 49%) tumors; however, no correlation was found between HE4 expression by IHC and any clinical factors, except nodal involvement. The expression pattern of HE4 is shown in Figure 1. Positive cases showed strong granular staining in the cytoplasm of cancer cells from the resected specimen of breast cancer (Figure 1A). Furthermore, although normal stromal cells did not show any positive staining of HE4, ductal epithelial cells showed a weak positive expression of HE4. Immunofluorescent staining of HE4 showed cytoplasmic localization of this protein in cultured cells (Figure 1B). Furthermore, RT-PCR showed HE4 mRNA expression in breast cancer specimens and cultured cell lines (Figure 1C). Two cell lines (MCF7 and BT474) expressed HE4 protein and mRNA. The correlation between HE4 and the other markers, including HER2 and Ki-67 was investigated; however, no relationship was found between them.
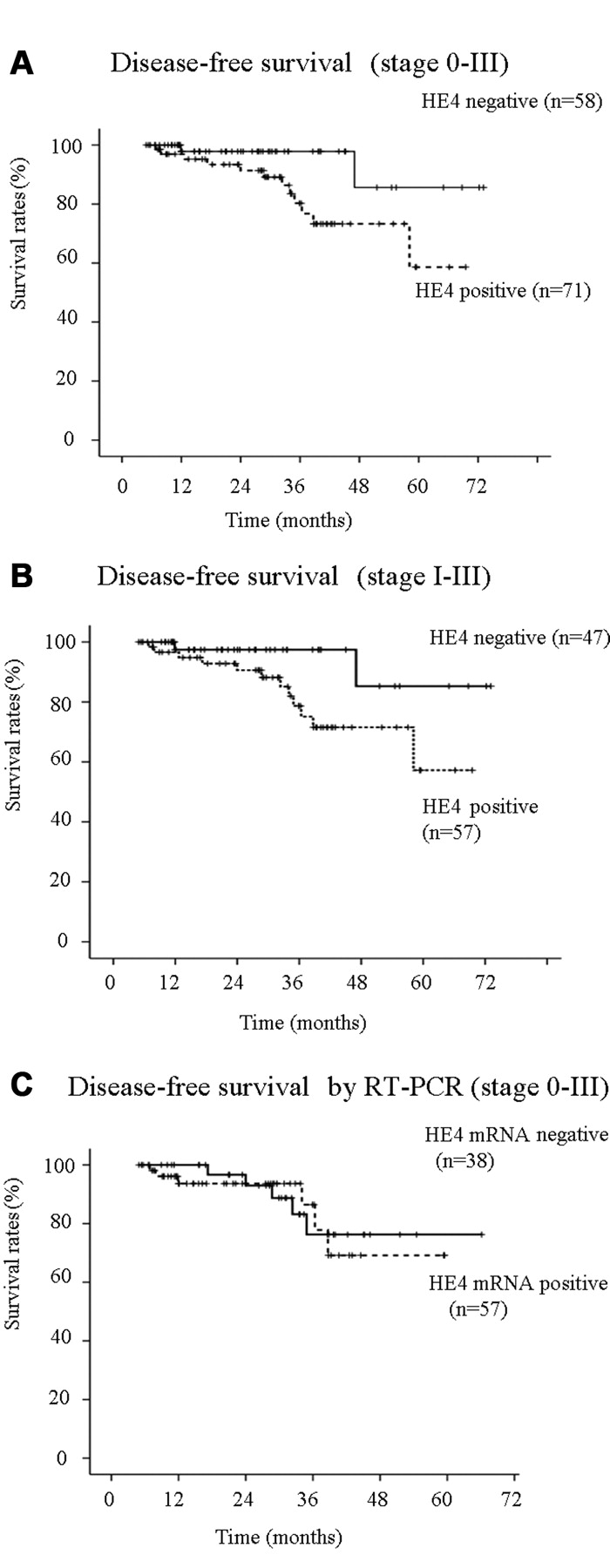
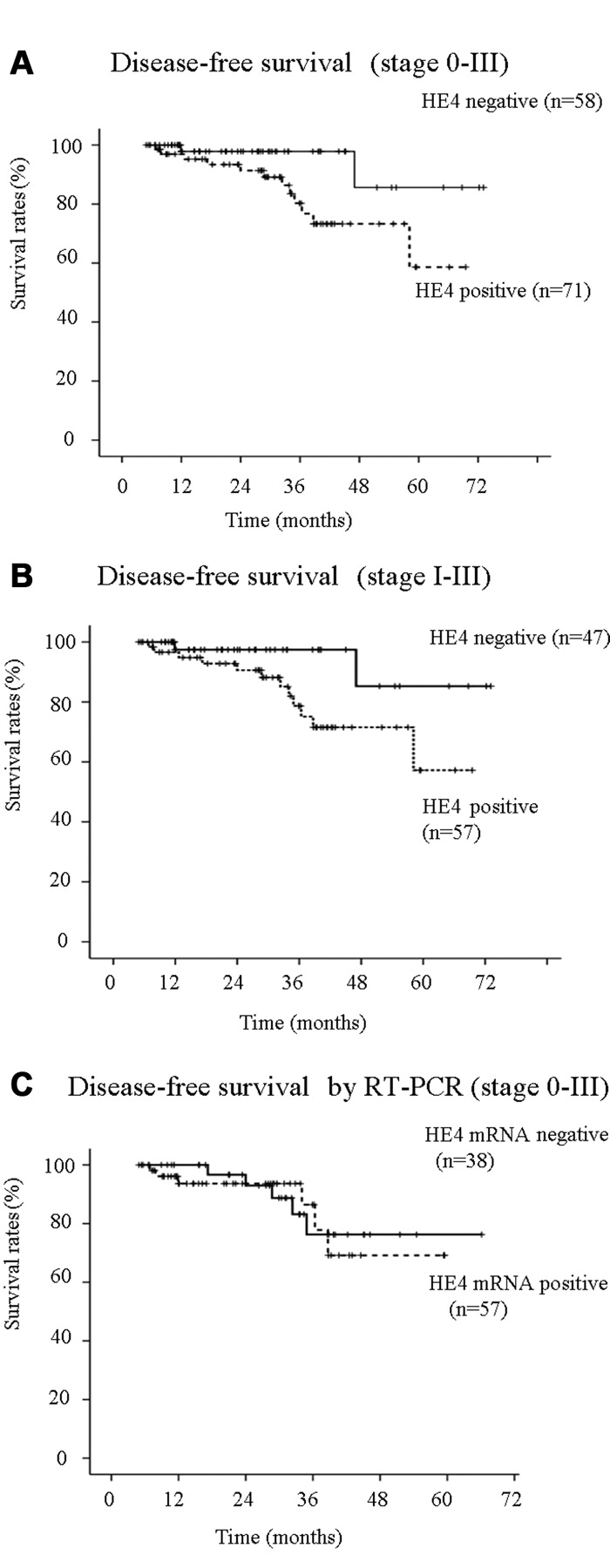
Disease-free survival of all patients (A) and stage I-III (B) according to HE4 protein expression. Five-year disease-free survival 58.6% in the HE4-positive and 85.6% in HE4-negative (p=0.04) groups. Five-year disease-free survival was 57.2% in the HE4-positive group and 85.3% in the negative (p=0.04) group in stage I-III. Disease-free survival of all patients according to HE4 mRNA expression (C). This result was not statistically significant.
Disease-free survival. Figure 2 shows disease-free survival according to the stratification of HE4 expression. Five-year disease-free survival in the HE4-positive group (62.2%) was significantly worse than in the negative group (85.6%, p=0.04, Figure 2A) by IHC. Furthermore, it was found that disease-free survival between positive and negative groups of HE4 expression by IHC without DCIS was significantly different (p=0.04, Figure 2B); however, the potential of a prognostic factor by HE4 expression was not elucidated by multivariate Cox regression analysis (data not shown). The five-year overall survival rates in both groups were not different, because of short follow-up periods. When prognostic value of the expression of HE4 mRNA was evaluated for available cases (positive, 57; negative, 38), quantitative real-time RT-PCR analyses did not show any difference between positive and negative expressions for disease-free survival (Figure 2C).
Discussion
HE4 is an anti-proteinase expressed in the normal reproductive tract and respiratory epithelium of the proximal airways (7). It is reported that HE4 is a tumor marker of serous and endometrioid ovarian carcinoma (8). A recent study showed that serum levels of this protein in patients with ovarian cancer may be a useful marker for tumor progression (9); however, the association between this protein and other types of cancer remain unclear. Galgano et al. reported the positive expression of HE4 in breast cancer (6) and in the current study, a clear immunohistochemical staining of HE4 protein in the cytoplasm of breast cancer was shown. In addition, a high frequency of positive HE4 expression was found in this study. Furthermore, this study showed that HE4 expression was not only found at the protein level but also at the mRNA level in breast cancer cells by RT-PCR. These results may lead to the speculation that a high expression of HE4 has a critical role in tumor progression; however, the prognostic significance of HE4 remains unclear.
In this study, the role of this protein in metastatic potential in breast cancer was investigated by immunohistochemistry. HE4 is closely associated with lymph node metastases. These findings suggest that HE4 is a possible predictive marker of lymph node metastasis and has a critical role in its recurrence. Although HE4 expression by multivariate analysis did not show the prognostic significance of disease-free survival, the disease-free survival curve according to HE4 protein expression showed significant differences between high and low expression groups. Although HE4 mRNA expression was investigated by quantitative RT-PCR to evaluate its potential as a metastatic factor, it was difficult to show this potential because of the contamination of normal duct epithelial cells. Further investigation using laser microdissection may be more successful.
On the other hand, HE4 is a member of the WAP domain protein family, which includes SLP1 and elafin (4, 5). These proteins function in host defence by not only anti-microbial or anti-viral activity, but also a different mechanism (10). Furthermore, the current result that the up-regulation of HE4 is associated with poor prognosis may lead to the assumption that this protein is not related to host defence but to cell proliferation. It has been reported that SLP1 and elafin are associated with tumor progression in addition to proteinase inhibitory function or have a role in the inflammatory response (11). Therefore, it was suggested that tumor cells expressing these protein families take advantage of the anti-proteinase function and act as a defence against the surrounding proteolytic and inflammatory environment. Since HE4 is also a member of the WAP domain family, it is plausible to speculate about the tumor growth activity of this protein. In fact, HE4 is not only a tumor marker of ovarian cancer, but also its expression was increased in pancreatic cancer compared with normal pancreatic ductal epithelium (12). Furthermore, the CGH study of lung cancer cell lines showed 20q gain (HE4, 20q12-13.2), suggesting the potential presence of oncogene in this region (13). Taken together, these data were consistent with the results of the current study and support the hypothesis that HE4 has a critical role in tumor progression. Although normal duct epithelial cells expressed HE4, other surrounding cells did not. These aberrant expressions of HE4 may be associated with carcinogenesis or tumor progression. Further investigation will be needed to clarify this possibility.
In conclusion, this study demonstrated that patients with HE4-positive breast cancer had a high frequency of lymph node metastasis than patients with HE4-negative tumor. HE4 might be a powerful tool to stratify worse candidate groups in breast cancer patients. Further investigation of HE4 might offer new insight into this possibility.
Acknowledgements
The Authors appreciate the technical support of Ms. Yoko Miyanari from the Department of Surgery II, Oita University Faculty of Medicine, Oita, Japan.
- Received July 17, 2010.
- Revision received October 1, 2010.
- Accepted October 5, 2010.
- Copyright© 2010 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Importance of Preoperative Knowledge of the Biomarker HE4 in Early-stage Endometrial Cancer Regarding Surgical Management
- HE4 Tissue Expression and Serum HE4 Levels in Healthy Individuals and Patients with Benign or Malignant Tumors: A Systematic Review
- Serum Human Epididymis Protein 4 and Risk for Ovarian Malignancy Algorithm as New Diagnostic and Prognostic Tools for Epithelial Ovarian Cancer Management
- Breast Cancer Survivorship and Surveillance