


Abstract
Patients with an oral squamous cell carcinoma (OSCC) often develop multiple malignant lesions. This report examined whether individual tumours developed in a patient show the same genetic alteration, such as p53 mutations. This case study describes three SCCs and three leukoplakias which developed simultaneously in a single 67-year-old Japanese man. A p53 mutation was detected in two of the three SCCs and one of the three leukoplakias. One SCC had a missense mutation at codon 285 (GAG>AAG, Glu>Lys) and the other a nonsense mutation at codon 336, and the leukoplakia had a missense mutation at codon 273 (CGT>CAT, Arg>His). This case showed that individual oral tumours may have different genetic changes even when they develop in a single patient. Therefore, this report provided strong evidence that in cases of multiple tumours it is necessary to design tailor-made therapies for each individual tumour rather than a single standardised therapy for all multiple tumours.
Oral squamous cell carcinoma (SCC) is a worldwide malignancy (1). Patients with a head-and-neck squamous cell carcinoma (HNSCC) often develop multiple malignant lesions. This notion has led to the field cancerisation theory (2) which hypothesises that the entire epithelial surface of the upper aerodigestive tract has an increased risk for the development of malignant lesions because of the multiplicity of genetic abnormalities in this wide tissue region. However, it is now clear from recent studies that molecular changes underlying the cancerisation field are not confined to areas with altered histology, as initially assumed (2). It is frequently observed that genetic damage persists beyond the histological border of precancerous lesions and tumours often develop far from the precancerous site (3).
Loss of heterozygosity (LOH) on chromosome 17 is one of the most frequent genetic alterations associated with the progression of malignant oral tumours and it may involve several loci. The p53 tumour suppressor gene is located on human chromosome 17p13.1 and frequently mutates in around half of human carcinomas (4, 5).
The present study reports on a patient with multiple primary carcinomas, consisting of five separate carcinomas and three leukoplakias of the head and neck region. To determine whether the individual head and neck carcinomas were of multiple origins but genetically related, or whether they were metastases, analysis of p53 mutation by yeast functional assay and subsequent sequencing analysis were performed. The yeast p53 functional assay tests the ability of p53 to activate transcription in vivo in yeast (2). It was demonstrated that the p53 status is diverse in oral SCCs and leukoplakias, suggesting that the tumours in a multiple carcinoma may have independent origins.
Case Report
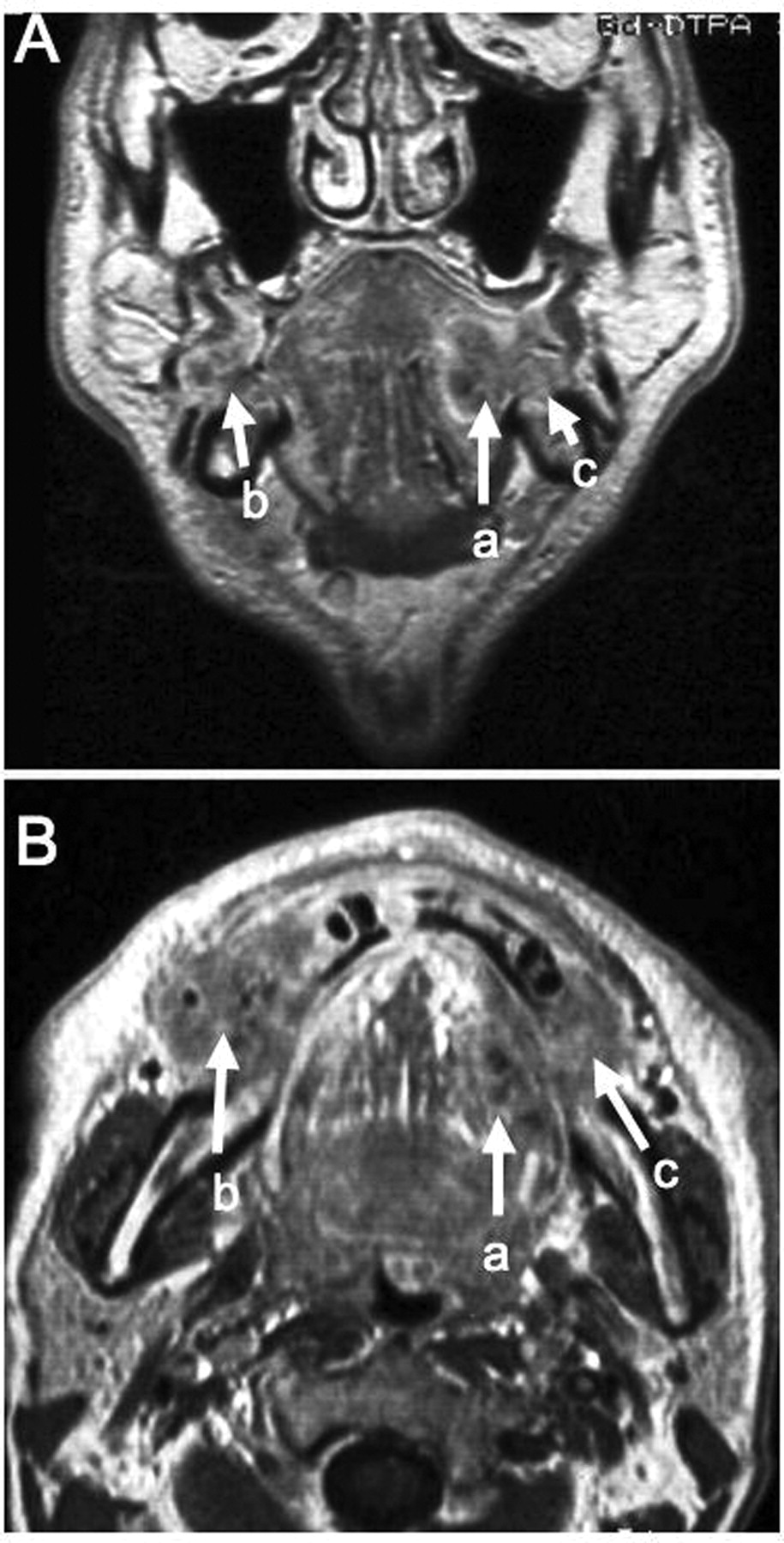
A 67-year-old man was referred to the Outpatient Clinic of Hokkaido University Dental Hospital in September 2003. He had an ulcerative lesion at the right (lesion 1) and left (lesion 2) lower gingiva and left side of the tongue (lesion 3) with a continuous dull pain in the most part of the mandibular area. He also had white patches (leukoplakia) in the upper left (lesion 4) and right (lesion 5) gingiva and left side (lesion 6) of the buccal mucosa (Figure 1). He had a long history of cigarette smoking (20 cigarettes a day) and alcohol intake (beer 500 ml + sake 300 ml a day) for about 48 years. Family history was unremarkable except that his mother had died of gall bladder carcinoma. Physical examination disclosed hard swelling of sub-mandibular lymph nodes at both sides of the neck: one at the right sub-mandibular, two in the right jugulo-digastric area, two in the left sub-mandibular and one in the left jugulo-digastric area. Magnetic resonance imaging (MRI) revealed ill-defined, hypointense masses in the lower right and left gingival regions and in the left side of the tongue. Both lesions in the gingival regions showed invasion of the medial surface of the mandible and extension into the bone marrow (Figure 2).
After being admitted to the Department of Oral Maxillofacial Surgery, the patient received 40 Gy preoperative irradiation in 20 sessions over 4 weeks along with chemotherapy consisting of CDDP (6 mg/m2, four times a week) and TXT (15 mg/m2, once a week). In December 2003, removal of the tumours and radical neck dissection were carried out under tracheostomy and general anaesthesia. Resection of the left half of the tongue and segmental resection of the most part of mandible body were performed. The mandible was reconstructed with titanium plates and the defects of the oral mucosa were repaired with rectus abdominis myocutaneous free flap. After the surgery, the patient was observed without adjuvant therapy.
Lesions 1, 2 and 3 were pathologically diagnosed as squamous cell carcinomas. The final TNM staging was pT4N2cM0. The patient was discharged in May 2004. Four months after discharge, he was admitted to a local hospital for terminal care, where he died of sudden severe bleeding due to a locally recurrent invasive tumour.
The histopathological study of the surgical specimens confirmed that lesions 1 and 3 were well-differentiated SCC, while lesion 2 was a moderately differentiated SCC. Leukoplakias (lesions 4, 5 and 6) showed hyperkeratosis with a low-grade dysplasia but no evidence of malignancy (Figure 3, Table I). Specimens of the tumors and leukoplakic lesions were subjected to yeast functional assay. The yeast assay which screens human p53 function in yeast is now described (6). The reporter yeast strain (yIG397) contains an integrated plasmid with the ADE2 open reading frame under the control of a human p53-responsive promoter. When the strain is transformed with a plasmid encoding mutant p53, the yeast strain becomes defective in adenine synthesis due to a mutation in the endogenous ADE2 gene. Therefore, colonies expressing mutant p53 are red, whereas colonies expressing wild-type (WT) p53 become white. In this system, when more than 20% of colonies are red the sample is considered positive for a p53 gene mutation (7) and plasmids recovered from at least five red colonies are sequenced for verifying the presence of clonal mutation(s).
p53 mutation was observed in two of the three SCCs and one of the three leukoplakias. In the SCCs, one missense mutation (lesion 1) at codon 285 (GAG>AAG, Glu>Lys) and one nonsense mutation (lesion 3) at codon 336 were observed. In the leukoplakias, one missense mutation (lesion 5) at codon 273 (CGT>CAT, Arg>His) was observed (Table I). All mutations were identified as clonal because the sequences from the five red colonies were identical. These results showed that two of the three mutations were G to A transition, being consistent with the record in the IARC TP53 database (http;//www.p53.iarc.fr), showing that the G: C to A: T transition is the most prevalent in oral SCCs in smokers (detailed in Discussion).
In addition, to detect human papillomavirus (HPV) infection of SCC samples, genomic DNA extracted from the tumour specimens was tested by multiplex PCR (8). No HPV infection was detected in any form of HPV subtypes (genotypes 6, 11, 16, 18, 30, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, and 66) (Table I).
Discussion
SCC is thought to progress through a series of well-defined histopathological stages that run parallel to specific genetic changes. Patients with a primary malignancy (especially in the head and neck area) are at high risk for developing additional primary malignancies (9). The oral cavity presents a field which, if exposed to carcinogens, may allow multiple precancerous and tumourous lesions to develop synchronously and metachronously. Generally, multiple primary tumours account for 3-5% of all malignant tumours. They most often have secondary malignant tumours; triple tumours occur in 0.5%, while quadruple tumours occur in 0.3% of all malignant tumours (10).
The criteria for diagnosing multiple primary tumours are: (i) each tumour presents a definite picture of malignancy, (ii) each tumour is distinct, (iii) there is no possibility of a metastatic lesion from one of the other tumours and (iv) the tumours are multicentric, if they are formed at one site and of an identical histological type (9, 11). The histologically verified SCCs in the present case were proven to be distinct by the MRI findings (Figure 3) and the macroscopic findings during surgery. However, it was impossible to exclude the possibility that the tumours may be metastatic lesions or disseminated from one of the tumours within the multiple tumour, either by image diagnosis or from pathological findings. The various p53 mutations found in the tumours (Table I) strongly suggested that they were of different clonal origin. Therefore, the tumours in the present case were defined as multiple and multicentric, fulfilling the above criteria (i) to (iv).

Preoperative state of the tumours. Arrows indicate cancerous ulcerations: on the left side of the tongue (a), on the right side of the lower gingiva (b) and on the left side of the lower gingiva (c). Circles indicate leukoplakic lesions: in the right (d) and left upper gingiva (e) and in the left side of buccal mucosa (f).
It is widely accepted that alterations in multiple oncogenes and tumour suppressor genes are the genetic basis for human carcinogenesis (12). The p53 gene is the most frequent target of genetic alterations, being mutated in half of all human carcinomas. It is suggested that specific types of p53 mutation have prognostic significance in oral cancer (13). In addition, the p53 mutation usually shows clonality in a carcinoma, implying that the mutation occurred in a very early stage of carcinogenesis, which likewise occurs in oral SCC (7). Consequently, distinct clonal p53 mutation works as a molecular tag that denies the metastatic dissemination cells of single tumour origin (14). This was seen in the present case, as the yeast functional assay and sequence analysis showed a distinct but identical (clonal) mutational status in each SCC: 285K in lesion 1, WT p53 in lesion 2 and 336X in lesion 3. In addition, other genetic alterations such as PTEN or PIK3CA may activate p53-dependent growth suppression in human cells (15). It has been suggested that the other gene alterations are also involved in WT p53 (lesion 2).
The sequences with which multiple tumours emerge are defined as: (i) simultaneous (all malignant tumours emerge at the same time), (ii) synchronous (the second tumour emerges within six months after the first) and (iii) metachronous (the multiple tumour is diagnosed more than six months after the recognition of the previous one) (16). In the present case, according to the patient's statement, three SCCs and leukoplakias of the oral cavity developed within six months. Different p53 mutations and histology demonstrated their distinctness. Consequently, the lesions in the present case fulfilled the criterion of, and therefore were classified as, synchronous multiple primary malignant neoplasms.
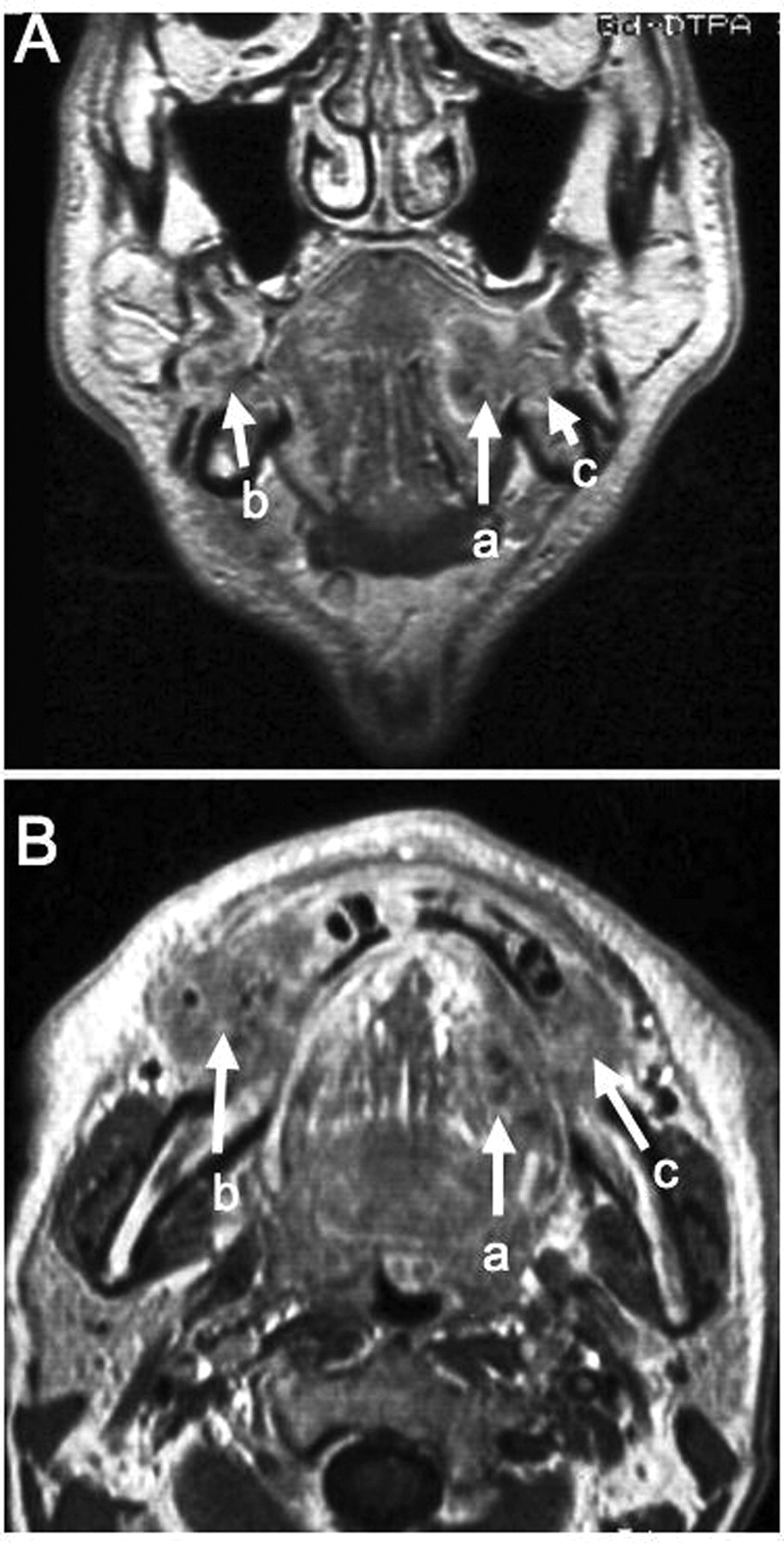
Coronal (A) and axial (B) contrast-enhanced T1-weighted magnetic resonance images, showing ill-defined, hypo-intense masses surrounded by a contrast-enhanced outer margin on the left side of the tongue (a), the right (b) and left (c) molar regions.
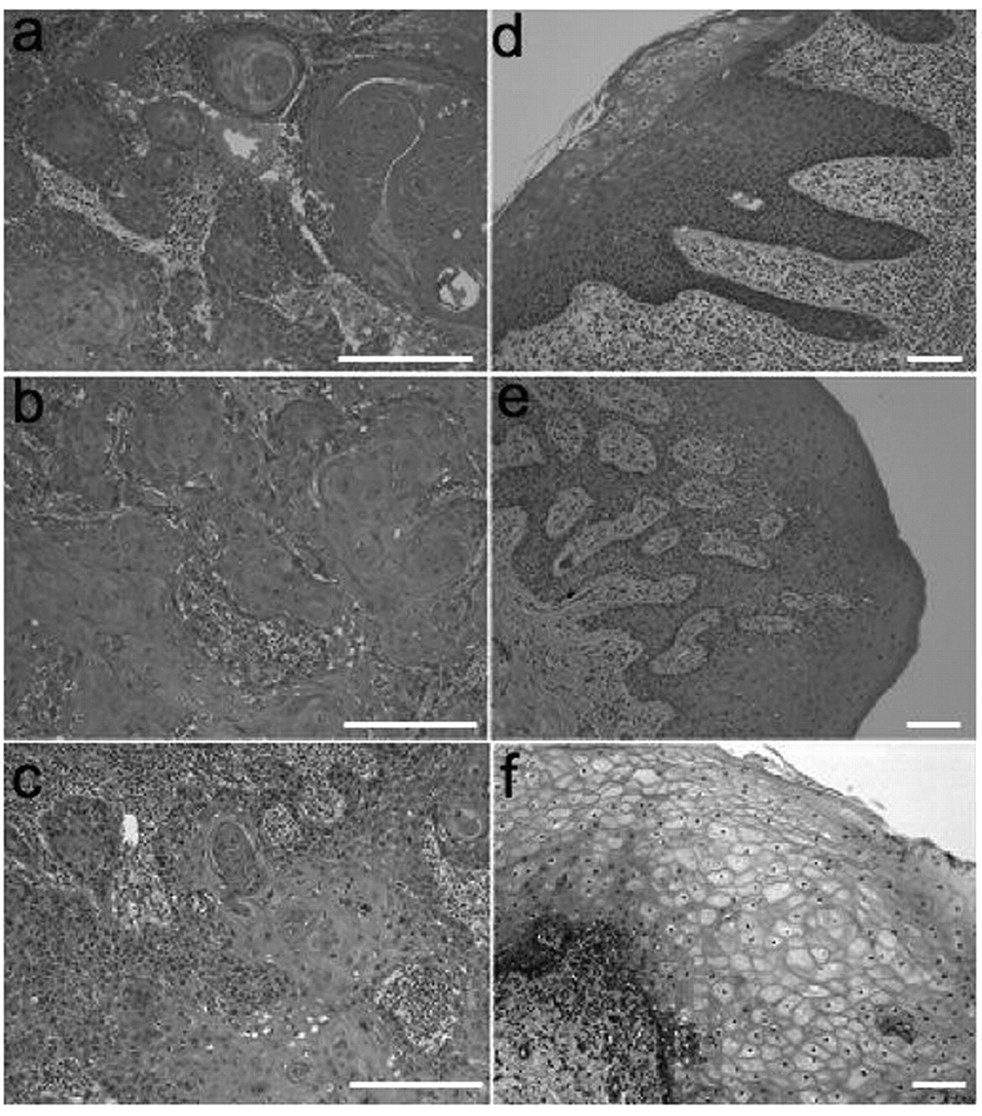
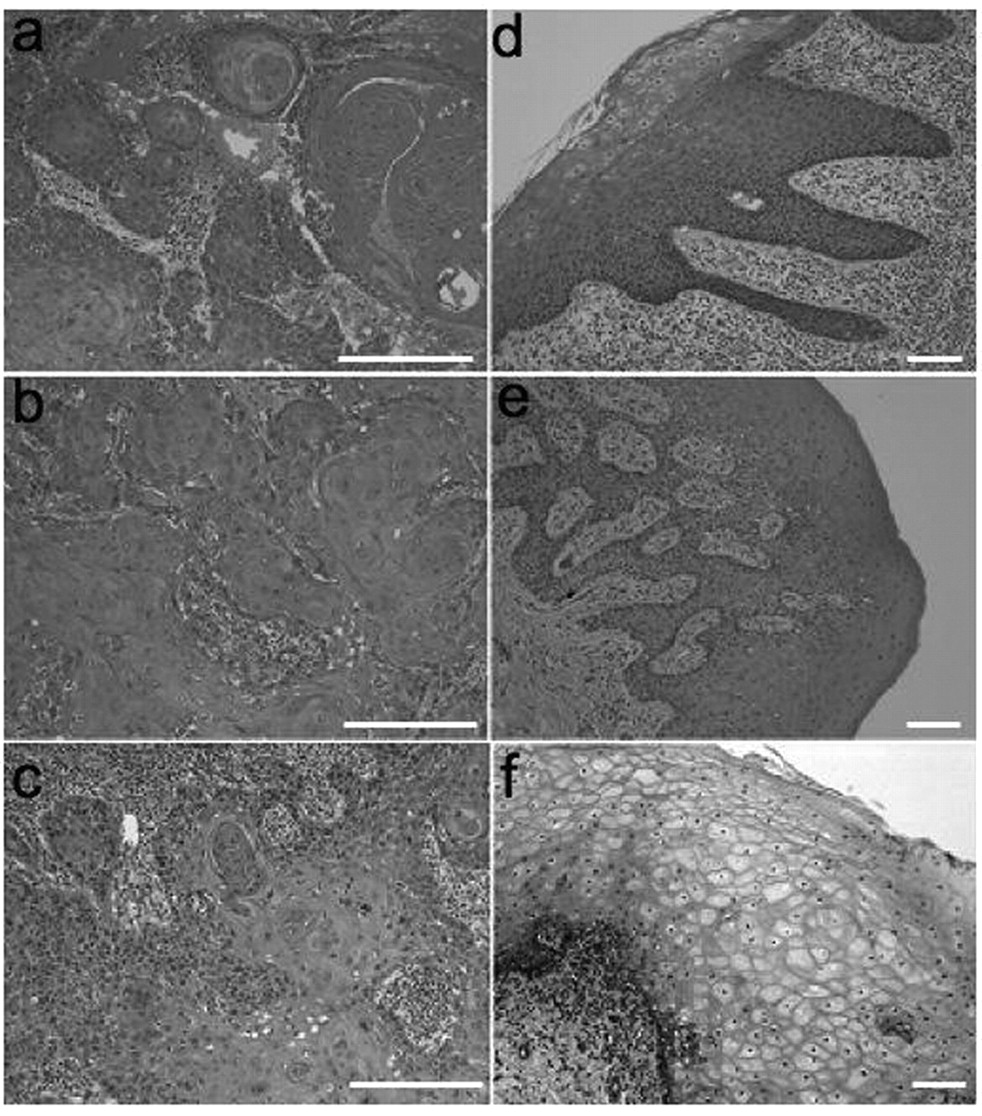
Histopathology of the biopsy specimens corresponding to the lesions in Figure 1. Well-differentiated squamous cell carcinomas (a, b, c), and leukoplakias (d, e, f) showing hyperkeratosis with low-grade dysplasia but no evidence of malignancy. Haematoxylin and eosin stain; scale bars, 100 μm.
Most multiple oral carcinomas are associated with leukoplakia (11); however, in pre-malignant lesions p53 alteration is not found frequently (7). It is most likely that tobacco smoking, as in the present case, causes a high incidence of p53 mutations (17). In the leukoplakias of the present case, WT p53 (lesion 4), 273H (lesion 5) and WT p53 (lesion 6) were also present (Table I). These observations suggest that p53 gene alteration occurred before the carcinogenetic change.
The concept of field cancerisation is used to explain the fact that those who are exposed repeatedly to carcinogenic factors such as tobacco and alcohol have a strong tendency to develop multiple primary tumours, as in the present case. Mutations of p53 gene occur during early stages in the development of head and neck SCCs because they are already present in premalignant lesions (18). In the present case, a hot spot p53 mutation was found in codon 273 in one leukoplakia. It has been shown that the malignant potential of leukoplakia is as high as 23-38% (19); hence mutations of p53 gene may be indicative of the potential of these lesions to develop into SCC. The G to A transition is a predominant mutation observed in oral SCCs caused from tobacco (tobacco-specific N-nitrosomines) (IARC database new version12, p<0.002) (18, 20). The most prevalent type of p53 mutations are G: C to A: T transitions; they were found in the present study twice within three mutations. The remaining mutation, G: C to T: A transition, was also found in the present case; it is also frequently encountered in tobacco smokers, although it is not significant in IARC data (p<0.11) (18, 20).
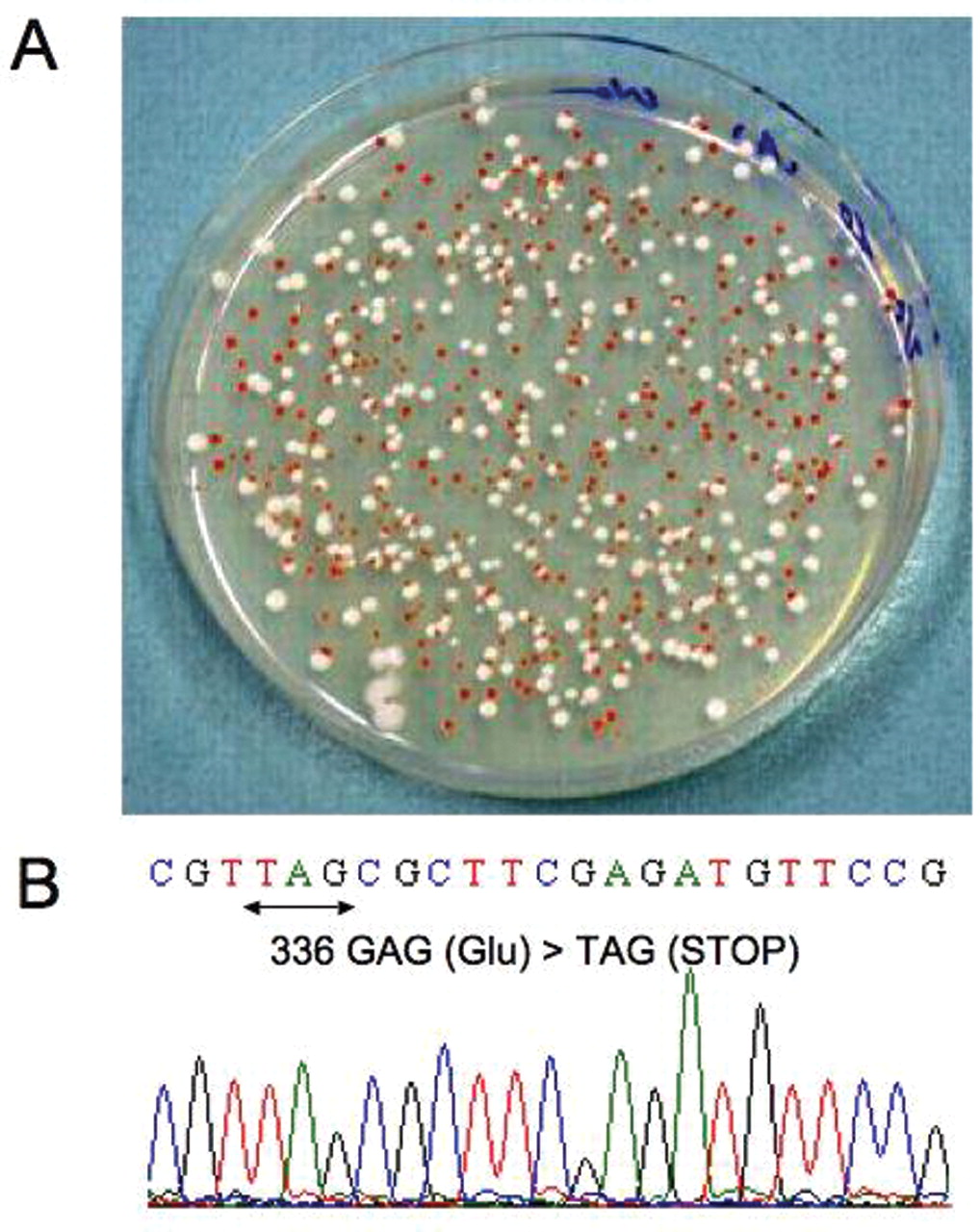
A: A representative result of the yeast p53 functional assay. Colonies containing mutant-type p53 are red due to accumulation of ADE2 substrate, while colonies containing wild-type p53 are white. The tumour specimen from the left side of the tongue gave 62.5% red colonies, indicating that 62.5% p53 mRNA in the tumour specimen was mutant. B: Sequence chromogram of the p53 cDNA recovered from a red colony. Wild-type sequence was CGT GAG CGC TTC GAG ATG TTC, in which the underlined glutamic acid changed into a stop codon at codon 336 (GAG>TAG).
Some tumours, including oral cancer, inherit gene mutations (21) but there are no published reports of a germline p53 mutation. To single out the specific cause of multiple primary malignant tumours is difficult. It is possible that exposure to carcinogens capable of causing multiple genetic abnormalities may develop carcinomas independently of each other throughout the entire anatomical region.
Multiple carcinomas may occur after successful tumour treatment. Based on molecular findings, a multidisciplinary plan may be designed for multiple cancer patients, providing valuable insight in the prognosis of future carcinomas. Extra care should be taken regarding the awareness of the patient with risk factors for carcinogenesis. The described case provided useful information for predicting the risk of multiple carcinomas.
p53 mutational status and HPV status.
Acknowledgements
This work was supported in part by Grant-in-Aid for Scientific Research (B) (J.H.) and Grant-in-Aid for Scientific Research (C) (H.K.) from the Ministry of Education, Culture, Sports, Science and Technology of Japan.
- Received August 18, 2010.
- Revision received October 16, 2010.
- Accepted October 19, 2010.
- Copyright© 2010 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.