


Abstract
Tissue inhibitor of metalloproteinase-1 (TIMP-1) is a major endogenous regulator of matrix metalloproteinases. This study examined the relation between TIMP-1 gene expression and postoperative mortality in patients with colorectal cancer (CRC). Specimens of CRC were obtained from 202 patients. The relative expression levels of TIMP-1 mRNA in cancer and in normal adjacent mucosa were measured by quantitative real-time reverse-transcriptase polymerase chain reaction. The expression level of the TIMP-1 gene was categorized as low or high according to the median value. The TIMP-1 level did not correlate with any clinicopathological feature. On Kaplan-Meier analysis, the 5-year overall survival rate was significantly lower in patients with high TIMP-1 (62.6%) than in those with low TIMP-1 (80.6%; p=0.0113). High TIMP-1 mRNA expression was associated with significantly poorer overall survival on univariate Cox regression analysis (p=0.0013) and multivariate analysis (p=0.0070). Overexpression of TIMP-1 thus correlated with poor outcomes in patients with CRC. Our results suggest that the TIMP-1 gene expression level might be a useful, independent prognostic factor in CRC.
Colorectal cancer (CRC) is now the third-leading cause of death from cancer in Japan (1). The prognosis of CRC depends on the extent of invasion and metastasis. An essential step in tumor invasion and metastasis is degradation of the extracellular matrix (ECM) (2).
Matrix metalloproteinases (MMPs) are the main group of enzymes involved in matrix degradation. Increased production of MMPs is associated with increased invasive and metastatic potential in many types of carcinoma (3). The activities of MMPs depend on the balance between the levels of the activated enzymes and the regulators of MMPs (4). Tissue inhibitors of metalloproteinases (TIMPs) are the major endogenous regulators of MMPs. Four homologous TIMPs (TIMP-1 to -4) have been identified. TIMP-1, a 28 kDa glycoprotein, specifically binds to progelatinase B, a pro-form of gelatinase B (MMP-9), and strongly inhibits its transformation to gelatinase B (5). TIMP-1 can inhibit proteolysis, and such inhibition should suppress cancer progression (6). On the other hand, TIMP-1 has been shown to have functions that promote cancer progression, such as stimulation of cell proliferation, inhibition of apoptosis, and regulation of angiogenesis (7, 8). A better understanding of the expression patterns of TIMP-1 and MMPs may provide important insight into the mechanisms of ECM degradation and tumor metastasis (9).
Overexpression of TIMP-1 mRNA and its protein has been found in several cancer types (10). However, the clinical significance of TIMP-1 gene expression in CRC remains to be clarified.
We measured expression levels of the TIMP-1 gene in specimens of CRC tissue and adjacent normal mucosa. We then examined the correlation between expression levels of the TIMP-1 gene and clinicopathological features. Finally, we assessed whether TIMP-1 gene expression was related to outcomes in patients with CRC.
Materials and Methods
Patients and samples. We studied surgical specimens of cancer tissue and adjacent normal mucosa obtained from 202 patients with untreated CRC. The patients underwent surgery at the Gastroenterological Center of Yokohama City Medical Center and at Kanagawa Cancer Center between 2002 and 2006. Informed consent was obtained from each patient. The Ethics Committees of Yokohama City Medical Center and the Kanagawa Cancer Center approved the protocol before initiation of the study. Each tissue sample was embedded in O.C.T. compound (Sakura Finetechnical Co., Ltd., Tokyo) and immediately stored at −80°C until use. No patient had any other malignancies. The specimens were stained with hematoxylin and eosin and were examined histopathologically. Sections consisting of >80% carcinoma cells were used to prepare total RNA.
Quantitative real-time reverse-transcription polymerase chain reaction (PCR). Total RNA isolated from CRC and adjacent normal mucosa was prepared with the use of Trizol (Gibco, Life Tech, Gaithersburg, MD, USA). Complementary DNA (cDNA) was synthesized from 2 μg of total RNA with an iScript cDNA Synthesis kit (Bio-Rad Laboratories, Hercules, CA, USA). After synthesis, the cDNA was diluted 1:4 with water and stored at −20°C until use. Quantitative real-time PCR was performed with an iQ SYBR-Green Supermix (Bio-Rad Laboratories). PCR reactions were carried out in a total volume of 15 μl, containing cDNA derived from 75 ng of RNA, 0.27 μM of each primer, 7.5 μl of iQ SYBR-Green Supermix containing dATP, dCTP, dGTP, and dTTP at a concentrations of 400 μM each, and 50 units/ml of iTag DNA polymerase. The PCR consisted of 10 min at 94°C, followed by 50 cycles of denaturation of the cDNA for 30 s at 94°C, annealing for 30 s at 58.9°C, and a primer extension for 1 min at 72°C followed by 10 min at 72°C. The PCR primer sequences were: TIMP-1 forward primer: 5′-CTG TTG TTG CTG TGG CTG ATA G-3′, TIMP-1 reverse primer: 5′-CGC TGG TAT AAG GTG GTC TGG-3′; β-actin (ACTB), used as an internal control, forward primer: 5′-AGT TGC GTT ACA CCC TTT CTT GAC-3′, β-actin reverse primer: 5′-GCT CGC TCC AAC CGA CTG C-3′.
Statistical analysis. Gene expression levels of CRC were compared with those of normal adjacent mucosa with the use of the Wilcoxon test. The relation between gene expression and potential explanatory variables were evaluated with the χ2 test. Associations between variables were assessed using the Mann-Whitney U-test. Postoperative survival rates were analyzed with the Kaplan-Meier method, and differences in the survival rates were assessed with the log-rank test. Overall survival was evaluated by univariate and multivariate analyses. We performed a Cox regression hazard analysis to calculate the hazard ratios of death according to clinicopathological features and TIMP-1 mRNA expression level. All statistical analyses were performed using Dr. SPSS II, version 11.0.1 J for Windows (SPSS, Inc., Chicago, IL). Two-sided P-values were calculated, and differences were considered significant at values of <0.05.
Results
TIMP-1 gene expression level was significantly higher in cancer tissue (5.96±12.45, mean±SD) than in adjacent normal mucosa (0.66±2.53; p<0.001) (Figure 1). The expression level of the TIMP-1 gene in cancer tissue was categorized as low or high according to its median value. Therefore, there were 101 low TIMP-1 patients and 101 high TIMP-1 patients. Relations between the expression of the TIMP-1 gene and clinicopathological features were then examined. TIMP-1 expression level was unrelated to age, gender, tumor location, tumor size, histological type, depth of invasion, lymph node metastasis, lymphatic invasion, venous invasion, and liver metastasis (Table I).
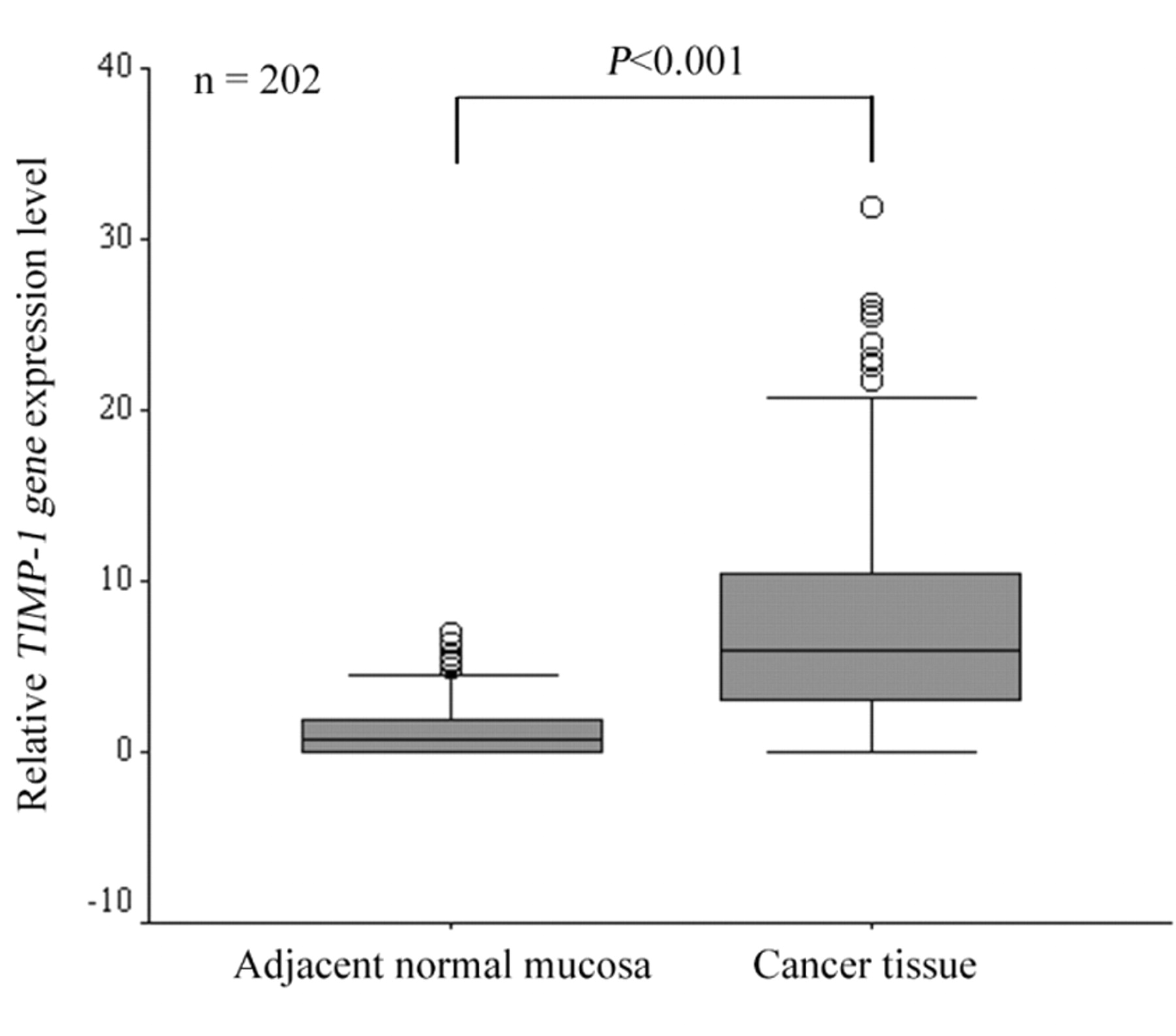
Comparison of TIMP-1 mRNA expression levels between colorectal cancer tissue and adjacent normal mucosa.
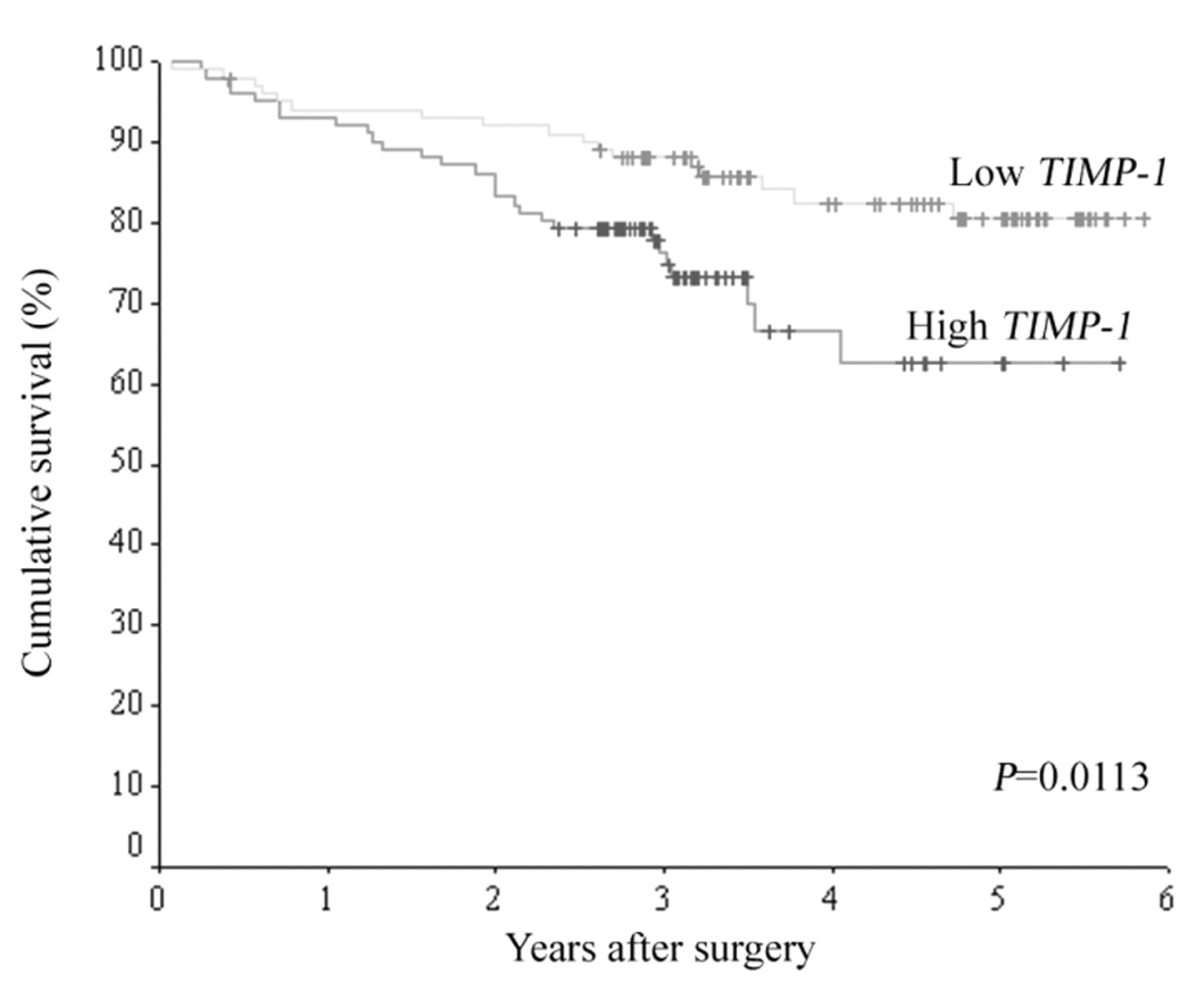
The median follow-up period was 1177 days. The Kaplan-Meier curve of overall survival according to TIMP-1 mRNA expression is shown in Figure 2. The 5-year overall survival rate was significantly lower in patients with high TIMP-1 (62.6%) than in patients with low TIMP-1 (80.6%; p=0.0113).
On univariate Cox regression analysis, high TIMP-1 expression was associated with significantly poorer overall survival than was low TIMP-1 expression (p=0.0013) (Table II). Multivariate analysis with a Cox regression model also showed that high TIMP-1 expression was associated with significantly poorer overall survival and identified high TIMP-1 mRNA expression as a significant independent predictor of overall survival (p=0.0070).
Discussion
Recent studies have proposed that TIMP-1 is a novel, important target for anticancer therapy (11). However, mechanisms responsible for the regulation of TIMP-1 and expression of TIMP-1 gene in CRC remain poorly understood. To evaluate whether the TIMP-1 gene is a prognostic factor in patients with CRC, we measured expression levels of the TIMP-1 gene and studied the relations between such levels and clinicopathological variables, including survival.
Several studies have reported that the level of TIMP-1 mRNA is significantly higher in tumor tissue than in normal colon mucosa (12-14). Consistent with previous results, we found that the expression level of the TIMP-1 gene was higher in cancer than in normal adjacent mucosa. Zeng et al. (15) proposed that increased TIMP-1 expression resulted from increased induction or production of MMPs within tumor stroma by colorectal tumor cells.
Relation of TIMP-1 gene expression level to clinicopathological features.
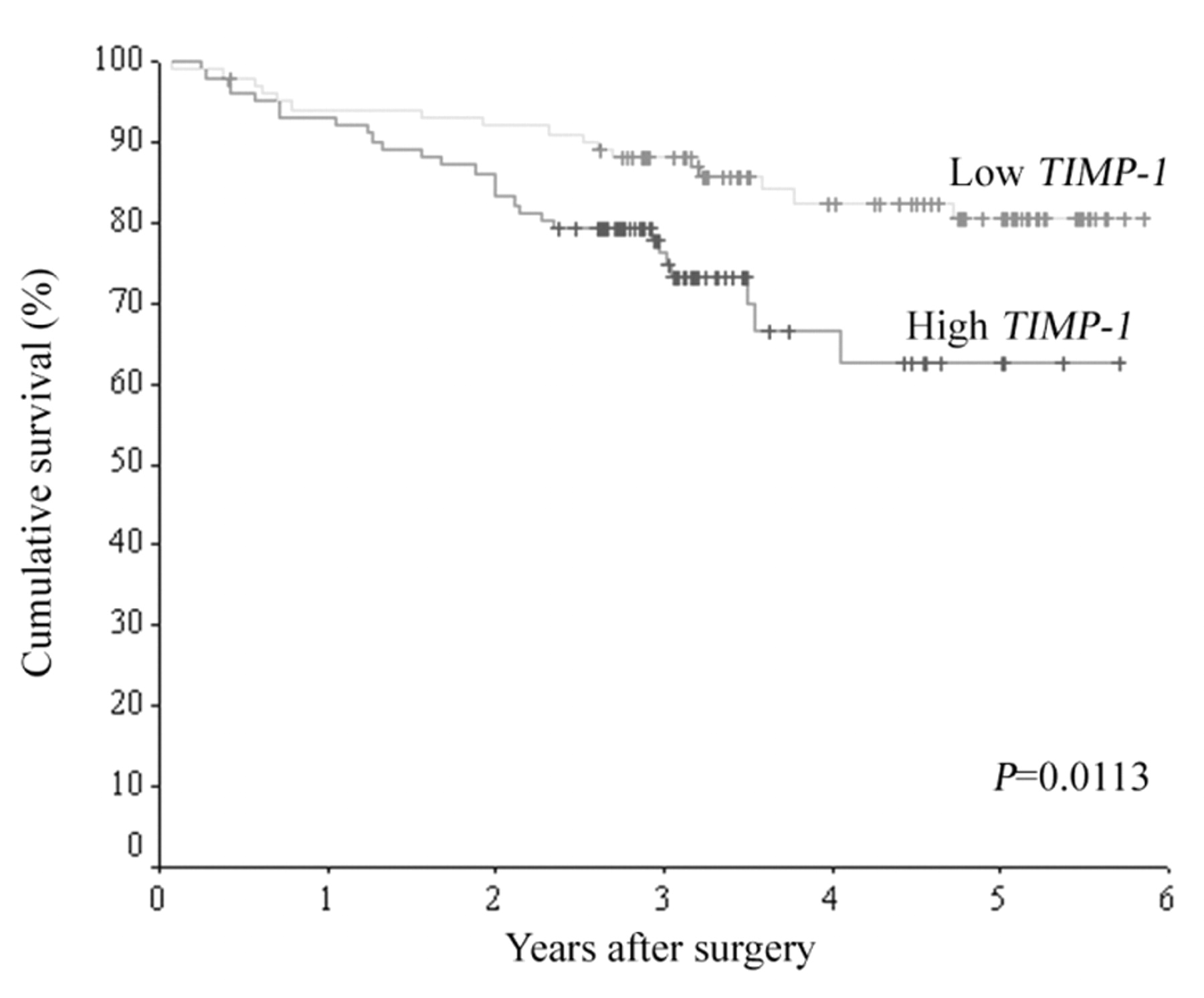
Kaplan-Meier curve showing overall survival according to TIMP-1 mRNA expression level in patients with colorectal cancer.
We also examined the relation between TIMP-1 gene expression levels in CRC and clinicopathological features. Islekel et al. (16) reported that TIMP-1 protein expression in tumor tissue significantly correlates with tumor differentiation. Zeng et al. (15) reported that elevated TIMP-1 mRNA in CRC stroma correlates with lymph node and distant metastases. In contrast, Pesta et al. (17) found no statistically significant correlation between TIMP-1 mRNA expression levels and tumor location or clinical stage. Our study also found no significant relation between the expression level of the TIMP-1 gene and any clinicopathological feature.
Influence of TIMP-1 mRNA expression on overall survival in colorectal cancer: univariate and multivariate analysis.
Finally, we studied the relation between TIMP-1 gene expression levels and survival in CRC. High levels of TIMP-1 mRNA are known to significantly correlate with shorter disease-free and overall survival in various typed carcinoma (10, 18). In CRC, Sutnar et al. (19) reported that the increased expression of TIMP-1 mRNA in colorectal liver metastases is associated with a short disease-free survival and a strong trend towards the early recurrence of liver metastasis. We found that high TIMP-1 expression was more frequently associated with poorer survival than was low TIMP-1 expression in patients with CRC.
In our study, TIMP-1 mRNA expression was not related to any clinicopathological feature. How TIMP-1 gene expression participates in cancer progression or invasion remains unclear. Recent studies have suggested that two mechanisms underlie the correlation of high TIMP-1 levels with unfavorable outcomes in CRC. Firstly, the TIMP-1 gene may be up-regulated in response to increased MMP activity, thereby inhibiting proteolytic activity associated with tumor invasion and metastasis (20). Secondly, increased TIMP-1 gene expression may be tumor-promoting because TIMP-1 acts as a growth promoter as well as an apoptosis inhibitor (21). For example, Kopitz et al. (22) reported that elevated stromal expression of TIMP-1 gene promotes liver metastasis by inducing hepatocyte growth factor signaling, which regulates a multitude of downstream prometastatic effector molecules, such as urokinase-type plasminogen activator and MMPs, leading to increased expression of other metastasis-promoting genes. Available evidence suggests that the TIMP-1 gene contributes to the progression of CRC through the growth-promoting or metastasis-promoting activities of its proteins.
In conclusion, our results show that overexpression of TIMP-1 gene is associated with poor outcomes in CRC. The expression level of the TIMP-1 gene might thus be a useful, independent prognostic factor in patients with CRC.
- Received June 14, 2010.
- Revision received August 24, 2010.
- Accepted September 2, 2010.
- Copyright© 2010 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}