


Abstract
Background: A cross-sectional study was performed on a cohort of colorectal cancer (CRC) patients to reveal any influence of age, gender, and subsite on grades of malignancy. Patients and Methods: Data from histopathological grading according to WHO criteria were pooled into groups of low-grade (well and moderately differentiated) and high-grade (poorly and undifferentiated) cancer and analyzed for associations. Results: In general, women with CRC were significantly older than men (p<0.05). In particular, women with high-grade cancer in the proximal and distal colon had a median age of 75 years and were thus 10-15 years older (p<0.01 and p<0.05, respectively) than their male counterparts. In contrast, high-grade rectal cancer developed in both genders around the early age of 60 years. Conclusion: Women are protected from more aggressive cancer in the colon though not in the rectum until well after menopause. This likely reflects the differential sensitivity of the mucosa at these sites against the anticancer effects triggered by activation of estrogen receptor-β.
Colorectal cancer (CRC) is the second leading cause of cancer deaths in Central European countries (1) and in the United States (2). In Austria the prevalence of colorectal cancer per 100,000 is 202 in men, and 231 in women, amounting to 10 and 8%, respectively, of all malignancies (1). CRCs can arise proximal or distal to the splenic flexure with different incidence rates [cf. (3)]. Men have higher incidences of colon and especially of rectal cancer than women (4-6). Beyond 50 years of age, CRCs occur in men typically 4 to 8 years earlier than in women (7).
Incidence of CRC at specific subsites varies considerably with age, gender, and race (8), perhaps due to different environmental, lifestyle or socioeconomic factors. For example, a large retrospective cohort study in Ohio showed that women presented with proximal colon cancers at a significantly higher age than men, and were less likely to have carcinoma in situ than men (9). A higher incidence of proximal colon cancer has been reported in low poverty compared to high poverty areas of the US (10). In some studies, age-related incidence of cancer was higher in the proximal colon compared to distal sites (11) but showed different patterns in men and women. In another study, based on 28 US cancer registries, the male-to-female ratio increased as the site shifted from the proximal to the distal colorectum (5).
There is increasing evidence that risk factors vary for colon and rectal cancer: Data from two large population-based studies indicate that, among others, age, gender, family history, consumption of red and processed meat, as well as alcohol are associated with significant relative risks for colon cancer, whereas only age and sex were associated with rectal cancer (6). In a study of over 140,000 adults in Austria, Rapp et al. (12) found significant relations between body mass index (BMI) and colon as well as rectal cancer, but only in men not in women. Larsson and Wolk (13) concluded from a meta-analysis of thirty prospective studies that a 5-unit increase in BMI was related to an increased risk of colon and rectal cancer in men, whereas in women only colon but not rectal cancer was associated with BMI. Data from the First National Health and Nutrition Examination Survey (NHANES I) indicated that bone mineral density, which is considered a surrogate marker for long-term exposure to calcium, vitamin D and estrogen, is inversely associated with incidence of colorectal cancer in general (14). In postmenopausal women, i.e. after cessation of ovarian estrogen production, an inverse relation was still found between bone mass and incidence of colon cancer (15, 16) though not between bone mass and rectal cancer (15). This is consistent with observations that vitamin D and calcium protect against development of cancerous lesions in the colon more than in the rectum (17-19).
Incidence of CRC in 102 patients grouped according to sex, anatomical location and histopathological grade.
For prevention, treatment and prognosis of CRC, it would be important to know whether age, gender and lifestyle-related factors have a specific impact on levels of malignancy of cancer at different sites along the colorectum. To investigate this issue, which had not been addressed in any of the aforementioned studies, we initiated a cross-sectional study on a cohort of colorectal cancer patients from whom tumor biopsies were also available for further pathohistological, immunocytochemical and molecular biological investigations (20).
Patients and Methods
Information on 102 randomly selected patients, who had undergone surgery for colorectal cancer during an 18-month period in 2001/2002, was obtained from the medical records of the Hospital Rudolfstiftung, Vienna. Data were pooled according to anatomical subsites, namely proximal or right colon (cecum, ascending and transverse colon), distal or left colon (descending and sigmoid), and rectum. Adenocarcinomas were graded according to the WHO classification (21) as well- and moderately differentiated, i.e. low-grade (G1 and G2), and poorly and undifferentiated, i.e. high-grade (G3 and G4) cancer.
Statistical methods. Statistical analyses were conducted using software packages S-PLUS (version 4.5, Lucent Technologies Inc., Murray Hill, NJ, USA) and SPSS (version 12.0.1, SPSS Inc., Chicago, IL, USA). The normal distribution of any data (sub)set under investigation was verified with the one-sample Kolmogorov-Smirnov goodness-of-fit test for continuous variables, or by the one-sample χ2 goodness-of-fit test for discrete variables. Normally distributed data were subjected to pairwise examination with Student's t-test and comparisons between more than two groups were carried out using one-way analysis of variance. Data that were not normally distributed were analyzed non-parametrically with the Wilcoxon rank-sum test for pairwise comparisons. Differences and correlations were considered statistically significant at p<0.05.
Relation between age, sex and subsite incidence of CRC.
Results
Baseline characteristics. Table I lists information on incidence of CRC in the study group in relation to gender, anatomical location and malignancy. In total, 102 carcinomas were diagnosed in the study group, of which approximately one-third each originated in the proximal and distal colon as well as in the rectum (Table I). However, it seemed that in women, carcinomas in the rectum were more frequent than in the distal or proximal colon, whereas in men the highest incidence was observed in the proximal colon (Table I).
Data on associations between age, sex and subsite incidence of CRC are given in Table II. Importantly, female CRC patients were significantly older than male patients (median age 73 vs. 63 years, p<0.05, Wilcoxon rank-sum test). The more advanced age of female cancer patients compared with males was primarily the result of age differences in proximal colon tumor patients (p<0.05, Student's t-test): Men presented at a median age of 60, whereas the women's median age was 75 years. No such correlation between age and sex was found for any other tumor site.
There was also no significant association of age with a specific tumor site, although patients with rectal cancer tended to be younger than those with a distal colon malignancy (p=0.058, Student's t-test). Within the group of female patients, those with proximal colon tumors tended to be older, whereas women with rectal cancer tended to be younger (data not shown).
Tumor grade and age, sex and subsite specificity of CRC. Of 102 carcinomas, 55 were of low grade, and 47 of high grade. Low-grade as well as high-grade cancer developed to the same percentage in men and women (Table I). The numbers of low- vs. high-grade carcinomas were 17 vs. 19 in the proximal colon, 19 vs. 11 in the distal colon, and 19 vs. 17 in the rectum (cf. Figure 1).
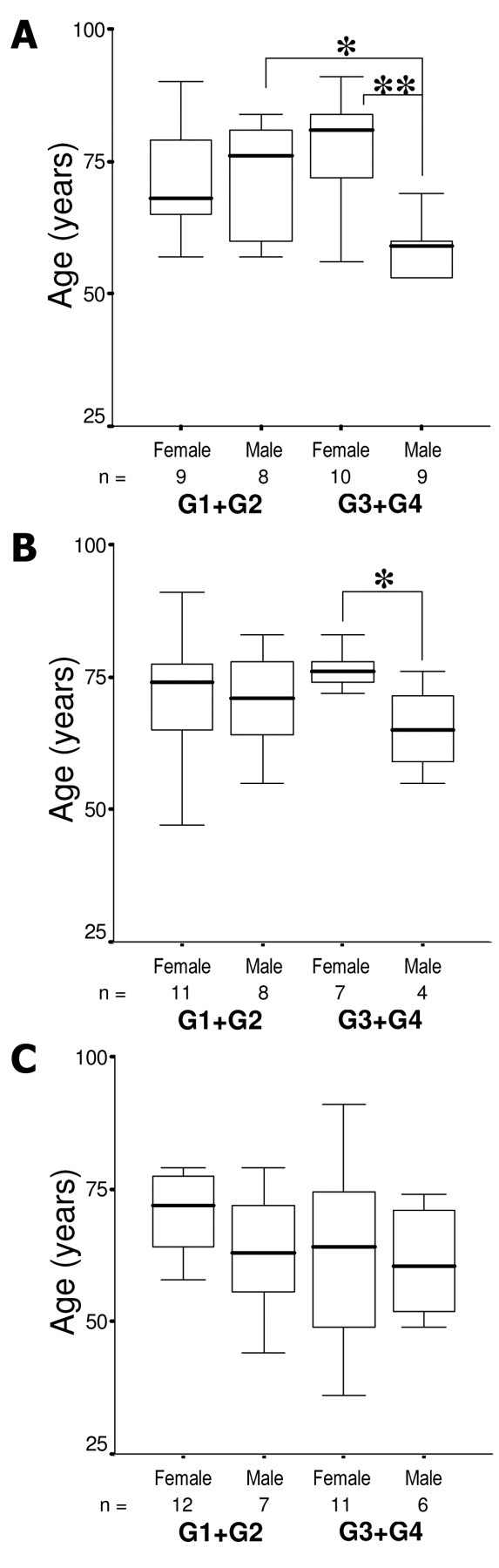
Association of low- and high-grade CRC with sex and age in A, the proximal colon; B, the distal colon; and C, rectum. n, Number of cases. *p<0.05, **p<0.01.
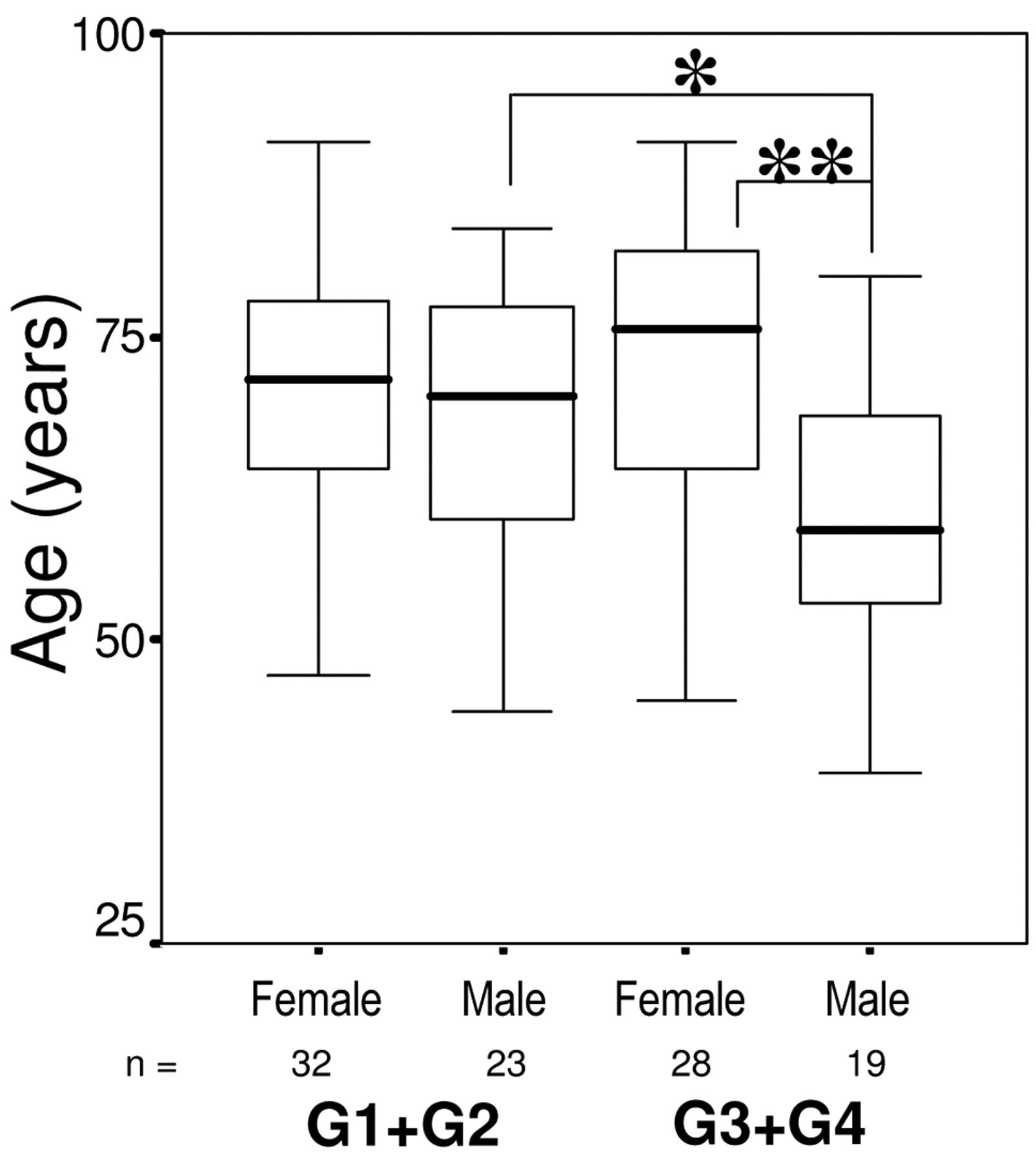
Distribution of low- and high-grade CRC according to sex and age. n, Number of cases. *p<0.05, **p<0.01.
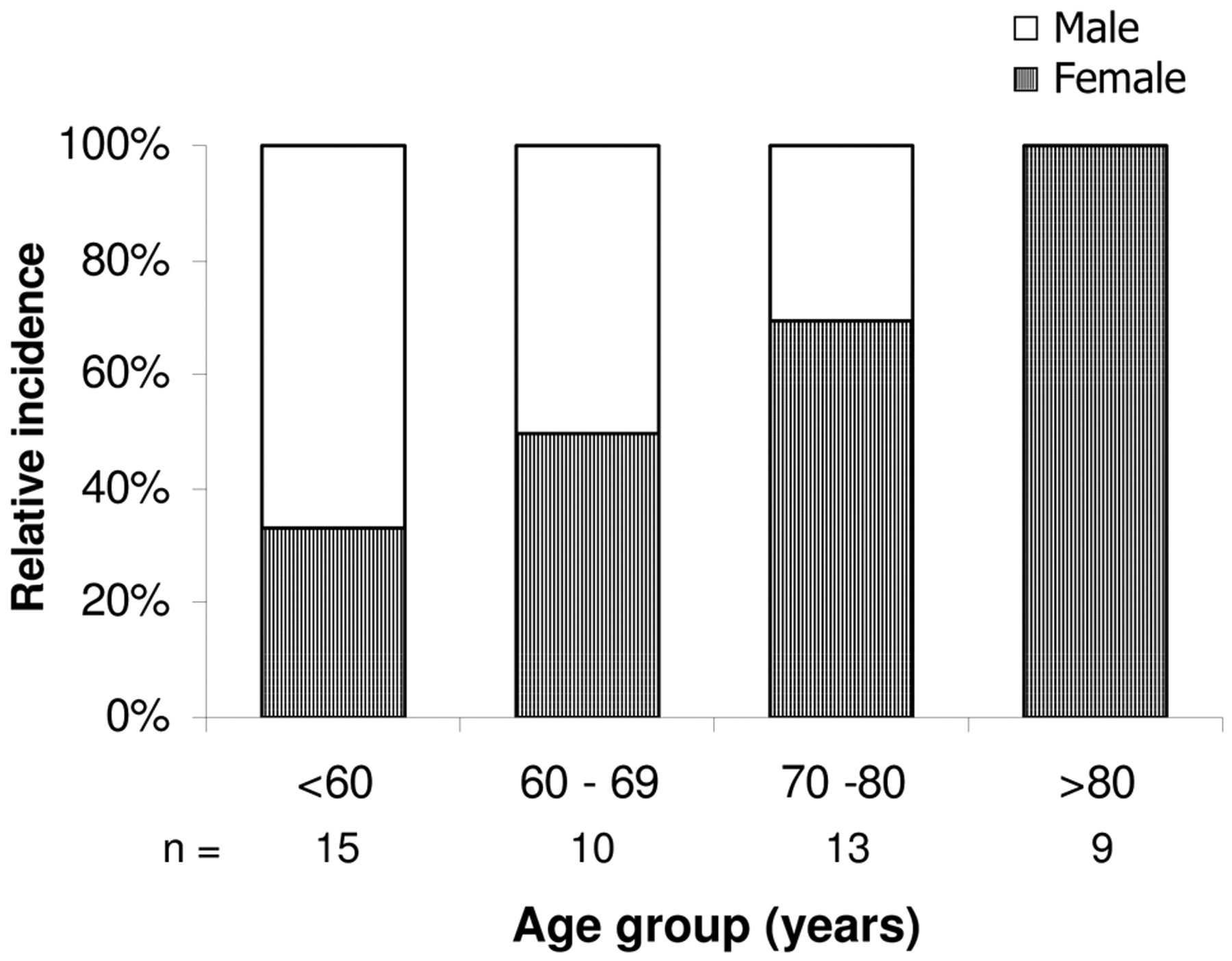
Overall, low-grade and high-grade cancer was diagnosed in the total cohort at nearly the same median age (70 vs. 68 years) (data not shown). When stratified for gender, this was valid for women but not for men, in whom high-grade (G3+G4) cancer developed significantly earlier in life than did low-grade (G1+G2) cancer (p<0.05, Student's t-test; Figure 2). Therefore, the difference in age between female and male G3+G4 patients is highly significant (p<0.01, Wilcoxon rank-sum test; Figure 2). In other words, at age 70-80 years, roughly 70% of patients with a G3+G4 cancer were female, and at age of >80 years, all G3+G4 patients were women. By contrast, at age 60 years and younger, the majority, i.e. 67%, of G3+G4 patients were men (Figure 3).
When grouped according to tumor subsite (Figure 1), in G1+G2 patients there were no significant differences in age between women and men at any subsite of the colorectum. The situation was different in the G3+G4 group, where women with cancer in the proximal or distal colon were significantly older than their male counterparts (p<0.01 and p<0.05, respectively, Student's t-test; Figure 1A and B). However, both men and women presented with high-grade rectal cancer at an early mean age of approximately 60 years (Figure 1C).
Discussion
Because patients in our study, although randomly selected, were from a single large city hospital, the results of the present study are representative for an urban rather than a rural population. We have to acknowledge that the size of the study group was relatively small because we deliberately analyzed data only of those CRC patients for whom surgical tumor biopsies were available for further investigation. Nevertheless, basic data on overall incidence of CRC in relation to age, gender and anatomical location (Table I and II) were similar to those reported from larger studies conducted elsewhere (3-5, 7, 8).

Relative incidence of high-grade CRC by gender and age.
The approximately even distribution of cancer sites within the colorectum found in the present study (Table I) is comparable to that previously reported by Austoker (3) for Great Britain and by Troisi et al. (8) for the USA. It must be noted that a general predominance of proximal over distal and rectal cancer sites, which clearly developed in the USA between 1975-1995 (8), was neither seen in the study of Austoker (3) nor in our present investigation. Most notably however, highly malignant cancer showed a more non-uniform distribution along the colorectum. The incidence rate, as calculated from data shown in Figure 1, was highest in the proximal and lowest in the distal colon, i.e. 53 vs. 37%, and intermediate in the rectum, i.e. 47%.
Several studies indicated that women are less likely than men to develop CRC at all ages (22, 23). This notion apparently does not apply to high-grade cancer, which in old age is diagnosed in women more frequently than in men (Figure 3). This is particularly obvious in case of high-grade colon cancer, where a gender gap of five to more than 15 years opens, when the tumor site shifts from the distal to the proximal colon: Figure 1A and B illustrate that men are prone to develop highly malignant cancer in the proximal and distal colon much earlier in life than women.
High-grade rectal cancer, which in our study amounted to nearly one-half of tumors at this site, developed in women and men both around the age of 60 years (Figure 1C). The high incidence of poorly and undifferentiated rectal cancer at an early age in women as in men strongly suggests that initiation of screening should be recommended for both genders at the same age (7).
The question why women are protected particularly from more aggressive cancer in early life cannot be easily answered. It has been argued that this may be a result of long-time exposure to estrogens before menopause, or of hormone replacement therapy thereafter (24-27). Because sporadic colon cancer progresses stepwise from adenoma to carcinoma, with a latency period that may last decades (28) and with highest incidence during advancing age, it is conceivable that tumors start developing slowly before menopause, but rapidly progress with cessation of ovarian estrogen production.
Antiproliferative effects of 17β-estradiol are mediated through the estrogen receptor (ER)-β, which is the predominant ER subtype in the human colon mucosa (29). In addition, there is evidence to suggest that the chemopreventive effect of estrogen against colorectal cancer is mediated in part through vitamin D receptor (VDR)-activated antiproliferative intracellular signaling. Early during tumor progression human colonocytes express high levels of the CYP27B1-encoded 25-hydroxyvitamin D-1α-hydroxylase, the enzyme that synthesizes the active vitamin D metabolite, 1,25-dihydoxyvitamin D3 (1,25(OH)2D3), which when bound to its cognate receptor, the VDR, effectively inhibits proliferation and promotes differentiation in human colon cancer cells (30). Estrogens have been shown to increase VDR and CYP27B1 expression and activity in human colonocytes (31-33). In addition, preliminary data from our laboratory indicate that estrogen up-regulates CYP27B1 expression in human rectal epithelium also in vivo (unpublished). Taken together, by enhancing the gene regulatory activity of the 1,25(OH)2D3/VDR complex, estrogen has the potential to intensify the antiproliferative effect of the vitamin D hormone.
Recently, Lin et al. (34) and Berubé et al. (35) reported that in pre-menopausal women, adequate calcium and vitamin D intake was particularly protective against more aggressive cancer. If this is valid also for proximal colon cancer, a compromised vitamin D and calcium status, as frequently observed in the elderly (36), together with diminishing levels of estrogen could explain the high incidence of poorly and undifferentiated cancer in women of advanced age. This notion is consistent with the observation that in postmenopausal women an inverse relation was found between bone mass and incidence of colon cancer (15, 16).
At present it is unclear why estrogens apparently protect against high-grade colon but not rectal cancer (Figure 1). One explanation could be that the density of the ER-β, which mediates the antiproliferative effects of the hormone, is relatively low (37), or epigenetically inactivated (38) at distal compared to proximal sites in the colorectum. Otherwise, activation of antiproliferative 1,25(OH)2D3 signaling by estrogens may be hampered by the high activity of the vitamin D catabolizing enzyme, 25-hydroxyvitamin D-24-hydroxylase, in human rectal mucosa (20). Further studies are needed to understand why rectal cancer in women is apparently insensitive towards estrogen and other modifiable risk factors (6, 13).
- Received April 15, 2009.
- Revision received June 8, 2009.
- Accepted June 18, 2009.
- Copyright© 2009 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}