


Abstract
Background: Serum tumor markers show low sensitivity, making them unsuitable for early detection of cancer. Activated macrophages (AM) from peripheral blood can accumulate tumor marker substances and facilitate early detection in prostate cancer. Here it was investigated whether carcinoembryonic antigen (CEA)-containing macrophages (CEACM) can be used to detect colorectal cancer (CRC) at earlier stages than can serum CEA. Patients and Methods: Peripheral blood was collected from patients with CRC (n=48), inflammatory colorectal disease (n=5) and from healthy controls (n=18). After separating and labeling AM with CD14-APC/CD16-FITC, AM were intracellularly labeled with anti-CEA antibody and flow cytometrically analyzed. Serum CEA and C-reactive protein (CRP) were measured. Results: The fraction-size of CEACM discriminated between controls and CRC patients, irrespective of AJCC stage (AJCC stage I-IV, p≤0.0001). Serum CEA values were significantly elevated in AJCC stage II, III and IV (p=0.02, 0.006 and <0.0001, respectively). Combining CEACM with CRP levels separated CRC from inflammatory colorectal disease. Conclusion: CEACM combined with CRP appears to have diagnostic potential in early CRC.
Early detection of cancer in general is assumed to improve the possibilities for curative interventions and for this reason many efforts have been undertaken to achieve this goal. When Gold and Freedman presented carcinoembryonic antigen (CEA) (1), people had great expectations but in time learned that CEA serum assays cannot be used for the detection of colorectal cancer (CRC). Both sensitivity and specificity of this marker were insufficient to support this. This applies in general for all known tumor markers, with exception of human chorionic gonadotropin (HCG) and lactate dehydrogenase LDH (2, 3). Recently we improved the method published by Herwig et al. (4) and demonstrated that activated macrophages, expressing both CD14 and CD16 on their membranes, had ingested prostate-specific antigen (PSA)-containing material. The size of the fraction of PSA-containing macrophages correlated well with the presence of prostate cancer (5). Activated macrophages can also be found as tissue macrophages in the interstitial space of many tissues and in particular in the stroma of neoplastic proliferations (6). These cells have the capacity to migrate from peripheral blood and accumulate substances in tumor tissue and tumorsurrounding tissue (7, 8). If they can phagocytize PSA in prostate cancer, it could be hypothesized this mechanism also applies to other tumor markers in other types of tumors and may achieve increased diagnostic sensitivity as well. Although not specific, CEA is present in high amounts in CRC tissue (9). For this reason, we selected CEA as a candidate to test this hypothesis for colorectal cancer. We initiated a prospective study where we compared the presence of CEA in activated macrophages in different stages of cancer and inflammatory disease with serum CEA values and the level of CRP.
Patients and Methods
Specimen collection. Medical ethical approval was obtained. Patients were included after histological confirmation of cancer on endoscopic biopsies was obtained and after informed consent. Consecutive inclusion was performed in the outpatient clinic or preoperatively on the ward. Classification in AJCC staging groups (9, 10) was based on histopathological evaluation. Control persons were selected and included by matching the participating cancer patients for age and gender and if possible for social and environmental influences (e.g. spouses). Table I displays included patients and healthy controls. Two EDTA tubes, two serum tubes and one heparin tube of venous blood were collected. The heparin tube was used for determination of CRP. One serum tube provided a serum CEA level within three hours after the vena puncture, the other serum tube was centrifuged at 4°C and the supernatant was stored at -70°C for future analysis. One of the EDTA tubes was used for a complete blood count (CBC). The remaining EDTA tube was kept at room temperature (RT) and processed for flow cytometry within 24 hours after vena puncture.
Patient and control group demography.
Mononuclear cell separation and immunocytochemical staining. One 3 ml EDTA blood sample per patient was transferred into a CPT tube (Becton Dickinson (B&D), Franklin Lakes, NJ, USA). A 20-minute centrifugation of the blood sample at 1650 ×g isolated the mononuclear cells in a dense layer between the Ficoll-Hypaque density layer and the serum. This suspension of single cells was transferred into 100 μl aliquots containing±106 cells. To label the macrophages, directly conjugated monoclonal antibodies were added simultaneously. Allophycocyanin (APC)-conjugated monoclonal antibody against CD14 (clone Mø P9, 25 μg/ml; B&D) combined with a fluorescein isothiocyanate (FITC)-conjugated monoclonal antibody against CD16 (clone NPK15, 125 μg/ml; B&D) were added and the cells were incubated in the dark at room temperature for 15 minutes. A Fix & Perm strategy (GAS004, Caltag; Invitrogen, Carlsbad, CA, USA) was performed after a single 2 ml phosphate-buffered saline (PBS) wash procedure. The fixation step consisted of the addition of 100 μl fixation reagent A for 15 minutes at RT and two 2 ml PBS wash steps afterwards. The permeabilization step was subsequently performed by adding 100 μl permeabilization reagent B in the presence of 20 μl biotinylated anti-CEA-antibody (clone II-7, 270 mg/l; Dako Cytomation, Glostrup, Denmark), added for intracellular staining. Biotinylation and subsequent blocking was performed by using an Animal Research Kit (ARK; Dako Cytomation); calculating the needed biotin and blocking-reagent was based on the use of pure anti-CEA antibody Ig-concentration. A 15-minute incubation in the dark at RT preceded two washing steps with 2.0 ml PBS. This was followed by incubation of the cell-pellet for 15 minutes at RT with phycoerythrin-conjugated streptavidin (streptavidin-rPE; 0.5 mg/ml; CAT No. 349023; B&D). After another two 2.0 ml PBS wash-steps, the cell-pellet was resuspended in 0.5 ml PBS and ready for measurement. A negative control (NC) was prepared by incubating cells with non-relevant mouse immunoglobulins which were directly labeled with FITC (10.0 μl IgG1, κ-FITC, clone G18-145; B&D (Pharmingen)) and APC (2.5 μl IgG1, κ-APC, clone G18-145; B&D (Pharmingen)) to reveal background staining by the directly conjugated primary antibodies. Streptavidin-rPE was included in the negative control for detection of possible endogenous biotin binding.
Flow cytometrical analysis. The prepared samples were analyzed with a FACScanto flow cytometer (B&D). Excitation of the cells was performed by a 488 nm, air-cooled solid-state argon laser followed by a 17 mW 633 nm helium/neon laser. A 530-nm band pass filter enabled FITC-fluorescence detection, a 575 nm ± 13 (mean±SD) band pass filter provided PE-fluorescence detection and APC-fluorescence was assessed by using a 660 nm ± 10 (mean±SD) band pass filter. Seven-color setup beads (BD FACS; B&D) were used on a weekly basis for optimal device performance. Automatic compensation settings were obtained by using the FACScanto software (BD Biosciences). At least 30,000 events were counted for each sample. APC, FITC and PE signal data were recorded with logarithmical amplification. BD FACSDiVa software (B&D) was used for analysis of the acquired data; the flow cytometrist was blinded for any clinical information.
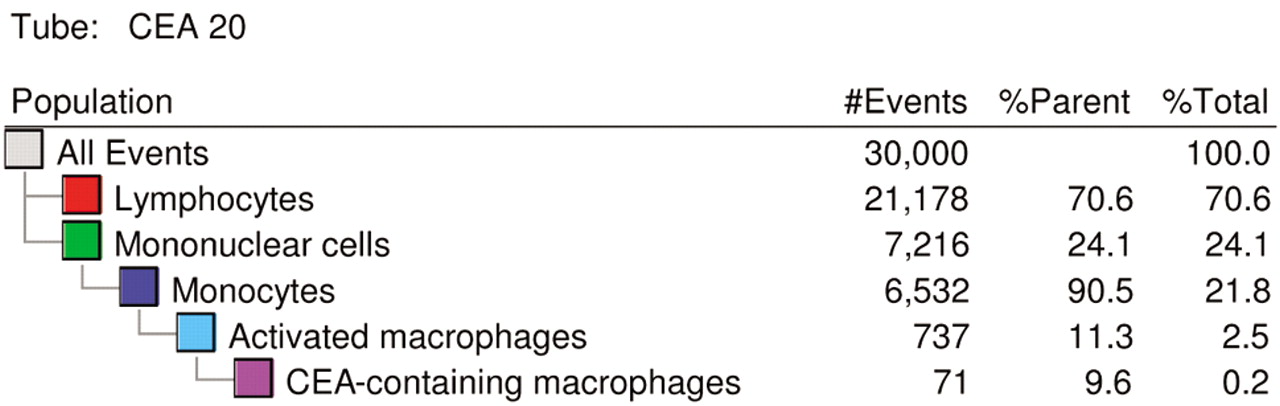
Parental gating structure. Parental gating, starting at the level of mononuclear cells, resulted in a stepwise separation of subpopulations of cells with accumulated complexity of phenotypical characteristics.
Gating procedure. Mononuclear cells were selected by drawing a gate in the forward scatter (FSC)/side scatter (SSC) plot to separate them from lymphocytes. Parental gating, starting at the level of mononuclear cells, resulted in a stepwise separation of subpopulations of cells with accumulated complexity of phenotypical characteristics (Figure 1). Within the population of mononuclear cells, CD14-positivity identified the monocytes. In the following step, CD14/CD16-positive activated macrophages were gated within the monocyte fraction. Finally, step 3 resulted in identification of the fraction of CEA-containing cells within the activated macrophage fraction (see Figure 2).
Biochemical assays. Serum CEA levels were determined on an Advia Centaur Immunochemistry Analyzer (Bayer Healthcare, Diagnostics Division, Tarrytown, NY, USA). The CEA assay on the Bayer Advia Centaur was a 2-sided dual monoclonal sandwich immunochemiluminescent assay (reference values of <5.0 μg/l (non-smoking population) and <10.0 μg/l (smoking population) were considered normal). Serum CRP levels were tested by particle-enhanced immunoturbidimetric assay (CRPLX, Tina-quant; Roche Diagnostics GmbH, Mannheim, Germany) (reference of <10.0 mg/l was considered normal) on a E170 Modular Analytics System (Roche Diagnostics, Hoffmann-LaRoche Inc, Basel, Switzerland).
Cytospin preparations and immunocytochemistry. After preparation of the cytospins, immunocytochemistry was performed for the detection of the CEA antigen, using the same monoclonal antibody as described above. For this purpose, an indirect streptavidin-biotin method was performed.
Statistical analyses. SPSS Statistical software, version 16 for Macintosh (SPSS Inc., Chicago, Illinois, USA) was used for the statistical analysis. The Mann Whitney U-test was used for analysis of differences. A p-value of less than 0.05 was considered statistically significant. Graphpad Prism, version 4.0 for Macintosh (Graphpad Software Inc., San Diego, CA, USA) was used for creating graphs.

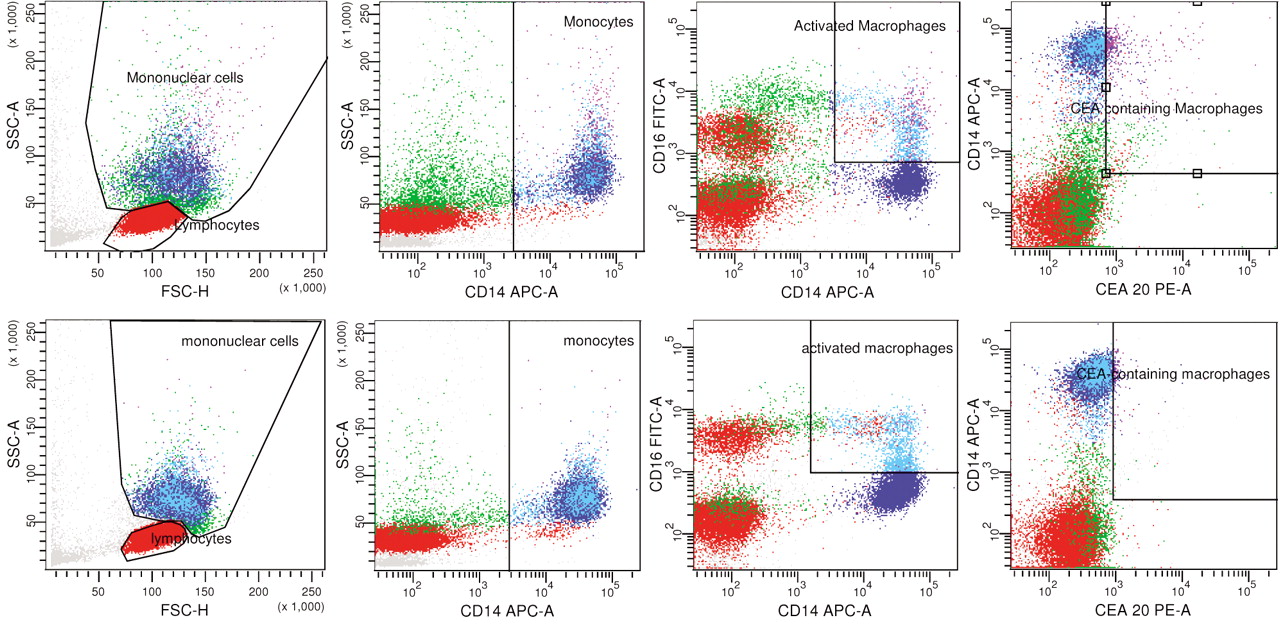
Gated sample of colorectal cancer patient (top row) and healthy control (bottom row). Parental gating is shown starting second plots from the left and in the two consecutive plots towards the right in both rows. More purple colored dots resembling CEACM are visible in the last, right-most plot of the colorectal cancer patient compared to the healthy control.

Patient group profiles showing fractions of activated macrophages and CEA-containing activated macrophages, and pre-operative CRP levels. Clearly the distinction between the healthy (contr.) and the benign (BI) groups, as well as all malignant groups, can be made by measuring CEACM. CRP adds the ability to significantly differentiate between the benign inflammatory patient group and AJCC groups I-III.

Comparison of the fraction of CEA-containing activated macrophages with serum CEA levels in AJCC staging groups. Cut-off values of 5.0 and 10.0 μg/l (healthy and smoking respectively) of the serum CEA assay are displayed by vertical continuous lines. The graph shows mostly higher staging groups being detected by the regular serum CEA assay, but not all such cases. The flow cytometric assay shows much better distinction between early cancer groups and the healthy controls. The horizontal dashed line could be used as a cut-off value for distinction between healthy controls (≤4.25-4.85%) and cases of malignant disease (>4.25-4.85%) depending on diagnostic demand. Sensitivity and specificity in this cut-off value range varied between 97.9-100.0% and 83.3-100.0% respectively.
Results
The size of the fraction of activated macrophages did not differ between the investigated patient groups with CRC (Figure 3). However, we observed that AJCC stage III (mean±SD: 32.68% ±11.46) had significantly higher fractions of activated macrophages compared to healthy controls (20.57% ±8.12, p=0.008), and stage I and stage II colorectal cancer (21.20% ±8.46, p=0.028 and 21.10% ±11.66, p=0.005, respectively). In all patient groups with CRC (AJCC stage: mean±SD), CEACM was significantly higher (stage I: 15.93% ±10.61, stage II: 17.63% ±12.76, stage III: 15.91% ±7.73, stage IV: 16.54% ±8,03, all p<0.0001) in comparison to healthy controls (2.86% ±1.19) (see Figure 3). The differences calculated comparing malignant disease with benign inflammatory disease were not significant; the difference between healthy controls and benign inflammatory disease (15.72% ±22.85) was significant (p=0.005). The pre-operative CRP levels of patients with benign inflammatory disease (165.67 mg/l ±48.38) did significantly differ from that of patients with colorectal cancer (stage I: 3.80 mg/l ±3.63, stage II: 14.75 mg/l ±17.85 and stage III: 11.75 mg/l ±15.90; p-values of 0.024, 0.034 and 0.034 respectively). Combining the measurements of activated macrophages, CEA-containing activated macrophages and pre-operative CRP levels provides a patient group-specific marker profile also separating benign inflammatory disease from cancer (Figure 3).
Serum CEA analysis (Figure 4). The standard serum CEA assay showed significantly elevated values in AJCC stage II to IV CRC (stage II: 6.36 μg/l ±13.49, stage III: 6.51 μg/l ±8.77 and stage IV: 95.18 μg/l ±176.31; p-values of 0.02, 0.006 and <0.0001 respectively) in comparison to healthy controls (1.45 μg/l ±0.70). In AJCC stage I (2.10 μg/l ±2.05), the serum CEA value did not significantly differ from that of healthy controls. In most of the investigated patients (including CRC patients), the serum CEA assay showed outcomes lower than reference values, together with high variance within the CRC groups.

Cytocentrifuged sample stained for CEA as prepared from an analysis sample used for flow cytometry. Visible are the bluish staining for the cell nucleus and the brownish anti-CEA staining inside intracellular vesicles containing CEA.
Photographic proof of CEA-containing macrophages. Immunocytochemical staining procedure of cytospins prepared from the monuclease cell fraction after CPT tube centrifugation showed the presence of vesicles staining positively for CEA in the peripheral zones of the cytoplasm of macrophages with large irregular nuclei (Figure 5).
Discussion
Serum tumor markers were initially thought to be the ideal instrument for early detection of malignant tumors. However, low serum concentrations as a result of dilution effects in the total blood volume, in combination with a majority of smaller primary tumors soon showed that only high-stage tumors or recurrent disease remained candidates for the use of these biomarkers (11, 12). Various committees tried to postulate guidelines for the use of tumor markers based on meta-analyses of international research in randomized controlled setting. The European Group on Tumor Markers (EGTM) (11), the National Academy of Clinical Biochemistry (NACB) (13), the European Society for Medical Oncology (ESMO) (14) and comprehensive cancer centers provide guidelines and quality assessments for the analysis process using serum tumor markers. In the current situation, these guidelines leave the clinician with a tool hardly applicable for use in major patient groups, leaving much room for improvement. At the moment, the only application of serum CEA in CRC treatment guidelines is the use of this value in the follow-up of CRC, not as a solitary marker, but as a small part of an intensive periodical follow-up strategy also including modern imaging techniques, endoscopy and physical examination. It has been shown from meta-analysis that an intensive follow-up strategy gains 7% in mortality reduction (15-17).
The results of both our present study and earlier publications (5) illustrate how intrinsic functions of a component of an organism such as tissue macrophages may be used to establish a test that provides insight into the state of health of the entire organism.
In view of the similarity of activated macrophages in the peripheral blood to tissue macrophages (18), we postulate that the success of our method used here is based on a special condition. Activated macrophages are attracted to the tumor stroma and find themselves in close proximity to the damaged tissue. The accumulation of cell constituents inside these activated macrophages leads to concentration. Once saturated, the activated macrophages reach the peripheral blood and are sampled via venapuncture. A second concentration step is built into our assay, namely when the buffy coat is selected. The labeling of the activated macrophages with CD14/CD16 can be regarded as an additional selective step. The last step, where the relevant tissue component is labeled and detected, thus receives a huge boost in sensitivity, which might explain the surprisingly good separation of controls from even AJCC stage I tumors. When comparing serum CEA with the fraction-size of CEACM in all patient groups (Figure 4), again the potential diagnostic power of this new assay even in AJCC stage I is shown. In most cancer cases, the new assay produced an elevated signal, whereas the serum CEA assay lacked this ability. At the time of writing, reference values have not been established. However, our present data seem to provide a preliminary cut-off value of 4.25% (Figure 3) to distinguish healthy controls (≤4.25%) from malignant cases (>4.25%). Using this cut-off, 100.0% sensitivity and 83.3% specificity was reached, even in AJCC stage I. Increasing the cut-off value to 4.85%, the sensitivity decreased to 97.9%, but the specificity increased to 100%. The cut-off value should be chosen according to the diagnostic demand. These characteristics are better than the calculated sensitivity and specificity of currently used diagnostic possibilities (16). These proposed preliminary cut-off values are of course dependent on the chosen gating strategy and may become different in the future.
It appeared in our study that non-malignant disorders of the colorectal mucosa also resulted in increased fractions of CEACM. For differentiation between benign inflammatory and malignant colon disease, the combination with an inflammatory marker, CRP appeared to be a good option. High CRP levels are associated with active inflammation and/or tumor necrosis in higher disease stages, whereas stage AJCC I and II in general show no signs of inflammation (low CRP values). The percentage of activated macrophages in AJCC stage III is elevated in comparison to the lower disease stages and stage IV disease. A possible explanation for this may be that lymph node involvement in stage III disease stimulates the immune system, whereas in stage IV disease the immune system may be suppressed or exhausted.
Differences in macrophage involvement may also be due to the macrophage activation state and macrophage reactions on entering this state. Upon an encounter triggering the macrophage, two possible reactions have been postulated in literature, the M1 and M2 reaction (6, 19). Phagocytosis for instance is performed by the M1-state macrophages, but angiogenesis is stimulated by M2-state macrophages (20) Phagocytosis of tumor remnants or even living tumor cells is of course desirable, but angiogenesis to support tumor proliferation is obviously not. Furthermore, the substances a macrophage encounters differ depending on the macrophage and location. The differences described above may explain why not all macrophages extracted from peripheral blood contain the same substances and also not the same amount thereof.
It can be concluded from data measuring M30, an apoptosis marker (21), in activated macrophages in CRC patients (manuscript in preparation) that this technique of detection of ingested substances in activated macrophages is applicable to whatever is technically detectable inside them. This enhances the diagnostic applicability by a natural, pre-analytical concentration step. A multi-marker strategy for solid tumors could be combined with this flow cytometrical approach, similar to the flow cytometrical analysis of patients with suspicion of bonemarrow-associated malignancies.
Determining the patient profile (Figure 3) considering inflammatory serum parameter levels and, perhaps, multiple flow cytometrically obtained tumor marker-containing macrophage fractions leads to a broader collection of cross-related information. This information may be suitable for predicting the origin of disease and enabling earlier detection of primary disease, at least providing incentive for additional invasive diagnostic procedures. In the context of activated macrophages, there may be a new diagnostic role for CEA in the early detection of colorectal malignancies.
Acknowledgements
Special thanks to F. Nauwelaers, B&D Biosciences for partially providing needed research supplies for the CRC trial and to R.J. Sauren, K. van Boxtel, J. Bransen and N.M. Janssen for providing laboratory assistance.
- Received March 18, 2009.
- Revision received June 2, 2009.
- Accepted June 16, 2009.
- Copyright© 2009 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}